
Abstract
Objectives:
Confocal laser endomicroscopy (CLE) uses a low-energy laser light source to obtain microscopic histology images of bladder tissue exposed to a fluorescent dye. To evaluate the feasibility of using CLE with two fluorophores: fluorescein (FLUO) and hexylaminolevulinate (HAL) to determine histologic and cytologic bladder cancer criteria.
Methods:
Patients eligible for HAL-photodynamic diagnosis-assisted transurethral resection of bladder tumor were included. The procedures were performed with the patient under regional or general anesthesia (60–90 minutes) after bladder instillation of HAL (50 mL, 8 mmol/L; Hexvix®; Ipsen, France). Resected tissue was examined ex vivo using CLE either with Cellvizio® system (CVI) single laser (488 nm) or with Cellvizio Dual system (CVII) double laser (488, 660 nm).
Results:
Twenty-one patients were included, 12 examined by CVI and 9 by CVII. Sample examination on CVI after HAL-CLE-only histologic analysis was not possible because HAL is mostly cytoplasmic and gives poor details on cellular architecture. On the contrary, FLUO-CLE gives good extracellular architecture and not clear information of nucleocytoplasmic abnormality. Samples on CVII for seven out of nine patients clearly showed cytoplasm of suspect cells and nuclei. In real time, fluorescence observed on bandwidth (673–800 nm) with HAL and FLUO was associated with the presence of cancer, with a sensibility and specificity of 80% and 100%, respectively.
Conclusions:
Real-time cytodetection was feasible using two fluorophores (FLUO and HAL) and the new system of CVII. This technology was useful to observe cytoplasm, nuclei, and nucleocytoplasmic abnormality, but an improved system is necessary (to overcome the overlapping of fluorescence) to increase the specificity.
Introduction
B
Inflammatory lesions are often PDD positive, such as carcinoma in situ, sometimes leading to false-positive rates above 60%, even after a learning curve. 5 In many cases, anatomo-pathologic analysis is required to guide interpretation. In this study, we aimed to improve PDD specificity with confocal laser endomicroscopy (CLE).
CLE uses a low-energy laser light source to obtain microscopic histology images of bladder tissue exposed to a fluorescent dye. Classically, CLE with fluorescein (FLUO) provides information on extracellular structure (papillary organization or not) and cell morphology (monomorphism, cohesion, sharp edges). 6,7 For flat lesions, the nucleocytoplasmic ratio (NCR) is a relevant element to distinguish inflammatory from tumor tissue. Unfortunately it cannot be determined with CLE using FLUO as the photodynamic agent. In contrast, HAL, a precursor of protoporphyrin IX (PPIX), is mainly metabolized in tumor cell cytoplasm. 3 Exploiting this difference with FLUO, we hypothesized that dual-band CLE could distinguish cytologic abnormalities.
The aim of this study was to evaluate the combination of CLE with these two fluorophores (FLUO and HAL) to obtain histologic and cytologic criteria, NCR, reported in classical real-time anatomo-pathologic analysis. We compared the preliminary results of our early experience with the CLE-PDD combination using single- and dual-band laser systems. 8
Materials and Methods
The local ethics committee approved this ex vivo prospective single-center study under the following number: NCT 02857634. Patients eligible for TURB with PDD were included in this study from April to June 2010 when CLE was performed with the classical 488 nm laser using the single-band Cellvizio® system with the GastroFlex probe (CVI) and from September 2015 to July 2016 when CLE was performed using the Cellvizio Dual system with the Ultra Mini O probe (CVII) (Cellvizio system; Mauna Kea Technology, Paris, France), which is a prototype. This system has currently no indication in urology.
Procedures were performed under regional or general anesthesia (60–90 minutes) after bladder instillation of HAL (50 mL, 8 mmol/L; Hexvix®; Ipsen, France). After white light and blue light cystoscopy, and immediately after resection of the lesions (26F resector, Exera II system; Olympus surgical and Industrial America, Inc., Center Valley, PA), the samples were studied ex vivo using single-band CVI or 488/660 nm dual-band CVII (samples were kept in isotonic saline). The red fluorescence of the resected samples exposed to blue light was noted ex vivo to select samples for analysis.
All samples were transferred to the pathology laboratory for classical anatomo-pathology study. CLE results were compared to pathology results, sample by sample. For CVI, a 2.7 mm GastroFlex-UHD Cellvizio fiber for confocal microscopy was connected to the CVI system. Fiber contact with the sample tissue produced 60 μm deep images with a resolution ≥1 μm (30,000 pixels) covering a 240-μm-diameter field. Only one laser (488 nm) and one bandwidth (500–633 nm) were used. A first image was recorded with HAL dye alone. Subsequently, 0.05% FLUO was applied to the sample to obtain images under HAL and FLUO with the same bandwidth. For CVII, a 4.2 mm MiniO/30 Cellvizio fiber was connected to the CVII system. Fiber contact with the sample tissue produced 30-μm-deep images with a resolution of 1.4 μm covering a 240-μm-diameter field. To use FLUO and HAL fluorescence both simultaneously and separately, two lasers (488 and 660 nm) and two bandwidths (500–633 and 673–800 nm) were used. Real-time fusion was applied. For each case studied with CVII, autofluorescence was first sought under HAL alone. The contribution of each of the laser observations was tested by alternately stopping one of the two lasers.
For the two systems, 12 images/s video clips were recorded and compared with the anatomo-pathologic findings. The confocal microscopy was performed according to criteria described by Liao. 6 After a first examination in real time, all video clips of CVI and CVII were reviewed by an expert urologist in confocal endomicroscopy for final analysis compared with histopathologic results.
Of the 21 patients included with an average age of 68 years (51–82), 6 (28%) patients had a history of nonmuscular infiltrant bladder cancer [2 pT1 high grade (HG), 2 pT1 low grade (LG), 1 pTa LG, 1 CIS], mean follow-up of 49 months (1–77) and 11 (52%) had no adjuvant treatment without relapse. Biopsy specimens from 21 patients undergoing PDD-directed biopsy after HAL instillation were assessed histopathologically and then further evaluated using CLE: n = 12 with CVI and n = 9 with CVII.
Results
For 15 patients, the pathology examination revealed urothelial cell carcinoma, 11 with nonmuscle-invasive bladder cancer and 4 with muscle-invasive bladder cancer. One dysplasia and five inflammatory lesions were reported. One patient had carcinoma in situ and eight patients had HG cancer.
To obtain a reference CLE image, HAL was not instilled in one patient on CVI (Fig. 1). Suspect HAL fluorescence cystoscopy was obtained in all samples except for the first case chosen as a control with FLUO alone on CVI and three on CVII. A complete histologic analysis could not be achieved with CVI and CVII after HAL-CLE without FLUO because most of the HAL was cytoplasmic, yielding poor details on cell architecture.
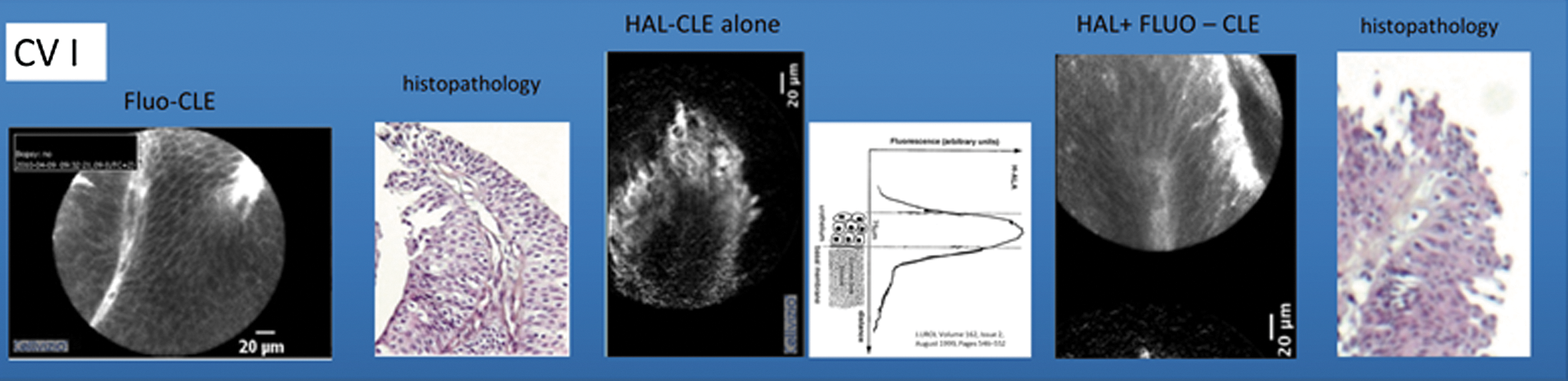
Compare to classical histologic aspect, we show in first result of CLE with FLUO (FLUO-CLE); in second distribution of HAL alone (HAL-CLE alone) on superficial part of papillary tumor; in third, aspect of CLE with HAL in Fluo (HAL+FLUO-CLE). CLE = confocal laser endomicroscopy; FLUO = fluorescein; HAL = hexylaminolevulinate.
Conversely, CVI after HAL-CLE with FLUO provided rich information on extracellular architecture (Fig. 1), but no information on the NCR except few images in three cases.
On CVI system
Image interpretation was more difficult than with FLUO alone. Low-grade lesions were found in 80% with CVI, but no HG lesions could be recognized with FLUO and HAL using the same bandwidths.
On CVII system
For one of nine patients, CVII clearly disclosed cells with suspect cytoplasm and nuclei. Real-time analysis revealed red HAL fluorescence (673–800 nm) separate from the FLUO fluorescence, although HAL fluorescence was colocalized in the 500–633 nm bandwidths with the 488 nm laser (Fig. 2). NCR was estimated normal for six of nine patients (2 LG, 3 inflammatory lesions, and 1 focal HG). A calibration error has made the examination uninterpretable for one patient. In the two last cases, histologic image interpretation was not possible when both fluorescences coexisted. When both lasers were stopped, no autofluorescence was detected; stopping the 660 nm laser had no effect on image editing. The 488 nm laser used alone was necessary and sufficient to observe both frequency bands.
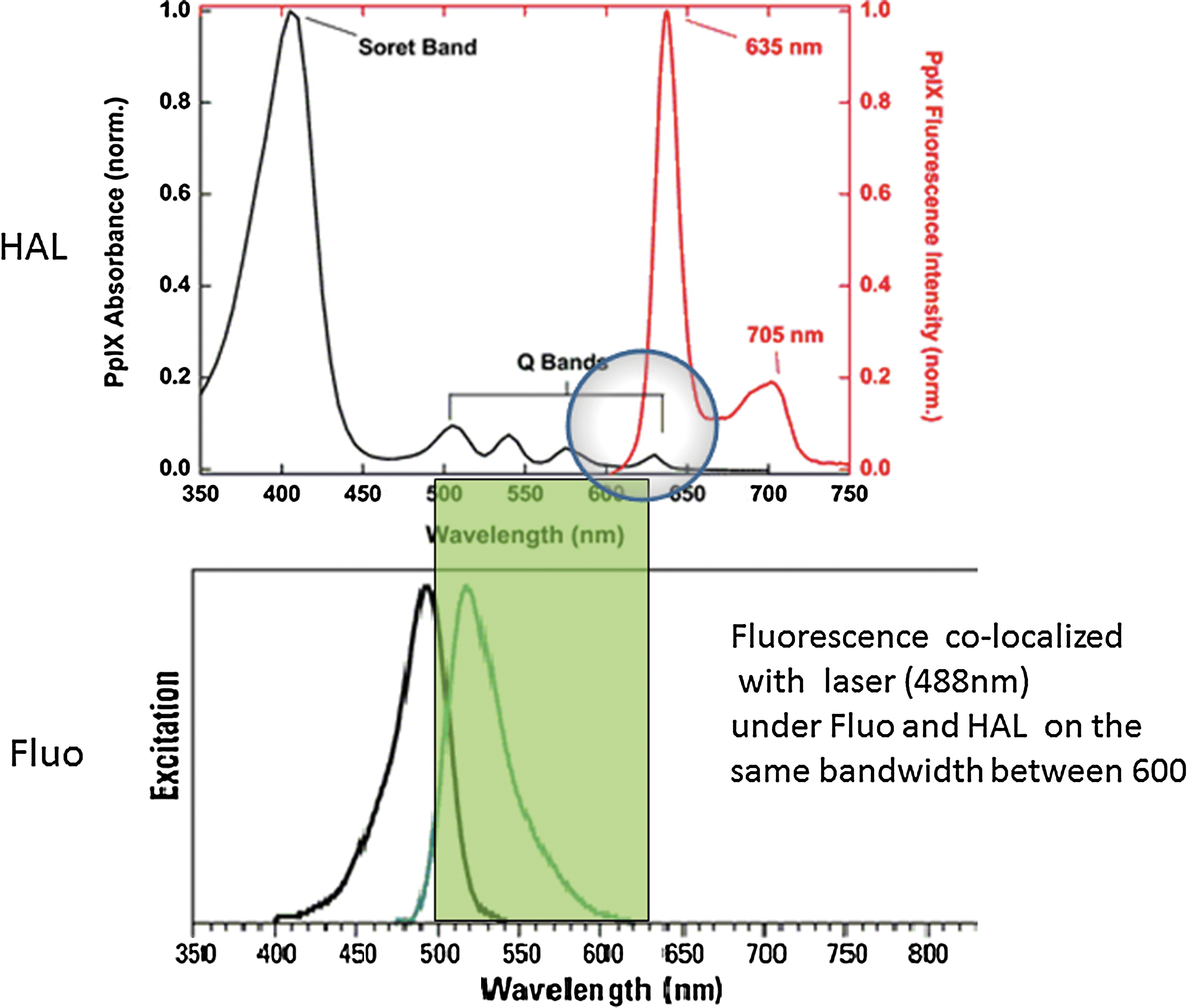
Distribution of HAL and FLUO bandwidth. We can observe an overlap of these two fluorophores on the 600–633 nm bandwidth.
On CVII when visible fluorescence on 673–800 nm under HAL and FLUO was observed, tumor tissue was present in 80% of cases (four of five patients) (Table 1, denoted with *). Except a case that presents a majority of no fluorescence, when no fluorescence was observed on 673–800 nm, no cancer was detected in each case (Table 1, denoted with **). With these criteria on this short sample, the sensibility and specificity were 80% and 100%, respectively.
Majority observation.
CLE = confocal laser endomicroscopy; FLUO = fluorescein; FU = follow-up; HAL = hexylaminolevulinate; HG = high grade; LG = low grade; NA = not applicable; PDD = photodynamic diagnosis; RNU = radical nephrouretectomy.
Comment
Liao's descriptions of confocal microscopy aspects based on histologic organization and morphology contour of urothelial cells are not easily reproducible for flat lesions. 6,9 Based on our experience, the diagnosis of papillary lesions is, in contrast, easier. Carcinoma in situ and inflammatory lesions are difficult to differentiate even with Liao's criteria. The difficulty with carcinoma in situ is that it can take on different aspects: sometimes the urothelium exhibits thickening characteristic while being abrasive among others. Cell characteristics are helpful in recognizing tumors. Generally, tumor cells display enlarged irregular nuclei with an abnormal NCR. Blue light on carcinoma in situ and inflammatory areas is characterized by red fluorescence that can be useful to guide the confocal microscopy exploration but cannot distinguish between tumor and inflammatory tissue. All NCR abnormalities are strongly associated with tumor diagnosis.
After instillation, HAL is actively transported into the urothelial cytoplasm and incorporated in the conventional cellular hem-biosynthesis metabolism. Cellular enzymatic abnormalities, as present in cancer cells and precancerous tissue, lead to accumulation of PPIX (photoactive porphyrins). After instillation in the bladder, HAL predominantly distributes in urothelial cells, decreasing rapidly below the lamina propria. 10
This distribution matches with the exploration field of confocal microscopy that explores a depth of 30–60 μm with CVII and CVI, respectively. Histologic grade, but not tumor stage, can therefore be determined using this technology. After resection, HAL fluorescence is not exploitable in the lamina propria.
As we observed, the second laser (660 nm) is noncontributory, as it does not correspond to peak excitation of the two fluorophores. The maximum peak excitation for PPIX (the HAL cytoplasmic metabolite) is 400 nm. The 488 nm laser corresponds to the peak of FLUO excitation and, in our experience, appears to stimulate PPIX, which exhibits a lower peak excitation at 500 nm. The fluorescence emitted by FLUO between 500 and 550 nm was classically observed by CVI and also by CVII over a bandwidth of 500–633 nm (Fig. 2). CVI got FDA and CEE approval based on its use in urology especially with FLUO.
With 488 nm laser, the fluorescence emitted by PPIX is limited at this bandwidth (500–633 nm) because the fluorescence peak begins at 600 nm to reach a maximum at 635 nm. A second peak at 705 nm was observed and corresponds to the second CVII bandwidth (673–800 nm) (Fig. 2). Nevertheless, despite an overlap, CVII could distinguish two separated fluorescences (FLUO, PPIX), and we have demonstrated in this study many preliminary interesting results (Fig. 3). Initially developed in neuroscience, CVII was not built for urology but was used to test this new concept. Fluorescence with HAL and FLUO was related to the existence of cancer with high sensibility and specificity. We think it may be possible to obtain significant results in the development of one system dedicated to urology.

Interpretation of images obtain on CVII. CVII = dual-band system.
Unlike the CVI results, the CVII results enabled a separate exploitation of FLUO and PPIX fluorescence that when merged provided images of cell contour (with FLUO) and, in negative, nuclear contours (with PPIX). FLUO remains in the extracellular compartment and is not specific to benign, or on the contrary, malignant, tissue. Tissue organization can be observed with FLUO only on CLE.
In our experience, LG papillary lesions retain their histologic organization, making the criteria described by Liao reproducible. Eighty percent of LG lesions are diagnosed with CVI using these criteria. This contrasts with higher grade lesions where cell disruption and noncohesive aspects may suggest a HG lesion but cannot be interpreted with certainty in a context of tissue inflammation or abrasion without cytonuclear aspect as on CVII (Fig. 4).

Histologic and cytologic aspects in grade tumor characterization with CLE.
CLE exploration may be usefully guided by blue light photodetection. CVII visualizes HAL fluorescence in operative specimens since tumor cells preferentially metabolize it. The technique allows an assessment of nucleus volume, given the 1.4 μm resolution with the MiniO/30 probe. The shape of the core can be studied, providing further evidence for a tumor cell. These aspects enable real-time pairing of cytodiagnosis with histodiagnosis provided by confocal microscopy for the first time in urology. Initial results of this preliminary study need to be confirmed since only eight of nine examined by CVII were contributive. Moreover, standardized conditions must be sought to obtain reproducible results.
Provided the technology of CVII can be perfectly integrated into routine blue light TURB, it should further contribute to the CVI by enabling a study of related HAL fluorescence even after FLUO instillation.
With the CVI system used in our in vivo experiment (unpublished results), and as has been described by other authors, 11 it was previously necessary to score suspicious areas under blue light by electrocoagulation resection to make sure such areas would be explored after FLUO instillation.
With CVII, the 673–800 nm fluorescence corresponds to suspicious areas under blue light, while concomitantly observing the 500–633 nm band used with CVI to determine tissue organization. The two fluorescences can always be merged with CVII providing information on the aspect and volume of the nuclei of suspicious cells (Figs. 3 and 4). Theoretically, with CVII, it is no longer necessary to score suspicious areas under blue light because these areas are still detected on 673–800 nm bandwidth after FLUO bladder instillation.
Nevertheless, it must be noted that CVII disclosed suspicious HG architectural modifications in one of three cases despite visible fluorescence in the 673–800 nm band. This finding may be related to our choice of a frequency band that did not cover peak PPIX fluorescence at 635 nm. Conversely, the most contributive CVII observation involved the nature of a sarcomatoid tumor that exhibited large nuclei (Fig. 3), a potentially important aid for diagnosis. Further technical developments will be needed for subsequent studies using CVII to explore urothelial carcinomas. Improvement on separate FLUO fluorescence and PPIX fluorescence could be possible if bandwidths are modified, but further research is needed to establish the place of this technology.
The optical biopsy is not an extensive analysis of the entire tumor because the fiber of confocal microscopy explores few areas of the tumor. For this reason, focal HG could be missing as in one patient on CVII. New methods that do not require fluorophores are also being developed to better define the optical appearance of suspicious areas. These techniques include narrow band imaging 12 and Storz professional imaging enhancement system technology. 13 As always, histologic confirmation will be required before these new methods can be put forward. Optic coherence tomography (OCT) is a suitable technique to define tumor stage. The specificity of OCT within the bladder is not high (65%). 14 No histologic view is possible with this technology, but the average exploration depth is better than with CLE (1–2 mm with OCT vs 30–70 μm with CLE).
Histologic grade and exploration of superficial lesions are generally the main targets of confocal microscopy. The technique was invented by Marvin Minsky in 1931 but did not reach the commercial stage until the late 1980s. Since that time, the Cellvizio system has become the most effective system for this endoscopic exploration because it is compatible with any rigid or flexible endoscope.
In addition, it can be combined with the entire image processing innovations described above. For the first time, this CLE system has provided simultaneous real-time cytologic and histologic analysis of bladder lesions. These results, obtained with CVII, open up a new era for confocal microscopy. The simultaneous use of different fluorophores offers a color vision of histologic elements, and as it occurred for histologic analysis with immunohistochemistry techniques, the advent of new specific fluorophore can be expected to revolutionize the technology. Simultaneous use of multiple lasers can also open up new perspectives. 15 New diagnostic and therapeutic tools will undoubtedly result from the future use of CD47 antibody-coupled nanoparticles. 16
There is no doubt that the diagnosis and treatment of urinary tract tumors will heavily rely on these new technologies. This means the urologist must acquire experience not only toward the macroscopic aspects highlighted by these technologies but also regarding the microscopic aspects of the underlying lesions. A better understanding of tumor phenomena will be essential for proper interpretation of new computer-assisted imaging results. A broader study should be conducted to confirm the results of CVII and limit fluorescence overlap.
Conclusions
We demonstrate the feasibility ex vivo of combining PDD and CLE. Using two fluorophores (FLUO, HAL) and CVII we have demonstrated, for the first time, the possibility of real-time cytodetection. This new technique provides information on tissue architecture, cell cytoplasm, and nuclei volume, as well as the NCR of suspicious lesions under blue light cystoscopy. An improved system is needed to limit fluorescence overlap and increase the reception of PPXI fluorescence. New studies should be conducted with an improved system to confirm these preliminary interesting results and increase the specificity. This technique provides a key for effective carcinoma diagnosis, in association with PDD.
Footnotes
Author Disclosure Statement
No competing financial interests exist.