
Abstract
Introduction:
Numerous studies have reported on regional or national trends of stone disease treatment. However, no article has yet examined the global trends of intervention for stone disease.
Methods and Materials:
A systematic review of articles from 1996 to September 2016 for all English language articles reporting on trends of surgical treatment of stone disease was performed. Authors were contacted in the case of data not being clear. If the authors did not reply, data were estimated from graphs or tables. Results were analyzed using SPSS version 21, and trends were analyzed using linear regression.
Results:
Our systematic review yielded 120 articles, of which 8 were included in the initial review. This reflected outcomes from six countries with available data: United Kingdom, United States, New Zealand, Australia, Canada, and Brazil. Overall ureteroscopy (URS) had a 251.8% increase in total number of treatments performed with the share of total treatments increasing by 17%. While the share of total treatments for percutaneous nephrolithotomy (PCNL) remained static, the share for extracorporeal shockwave lithotripsy and open surgery fell by 14.5% and 12%, respectively. There was significant linear regression between rising trends of total treatments year on year for URS (p < 0.001).
Conclusion:
In the last two decades, the share of total treatment for urolithiasis across the published literature has increased for URS, stable for PCNL, and decreased for lithotripsy and open surgery.
Introduction
U
Methods and Materials
Evidence acquisition: criteria for considering studies for this review
Inclusion criteria were as follows: (1) All articles written in the English language. (2) Studies reporting on national trends for urolithiasis treatment. (3) Patients of any age.
Exclusion criteria were as follows: (1) Studies reporting on regional trends for urolithiasis treatment where there were published national trend data. (2) Older studies using the same data as a more recent study. (3) Unsuitable or not available for analysis. (4) Studies examining treatment for nonurolithiasis conditions. (5) Studies with less than 100 patients.
Search strategy and study selection
The systematic review was performed according to the Cochrane Review and the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines. The search strategy was conducted to find relevant studies from Ovid Medline without revisions (1996–September 2016), Cochrane Library (2016), CINAHL (1996–September 2016),
Terms used included (but were not limited to): “temporal,” “trends,” “treatment,” “national,” “regional,” “calculi,” “stones,” and “urolithiasis.” Boolean operators (AND, OR) were used to refine the search.
The search was limited to English language articles between 1996 and September 2016. Authors of the included studies were contacted in the case of data not being available or clear. If the authors did not reply data were estimated from the graphs provided in the study; if the data could not be estimated then the study was excluded from analysis.
Two reviewers (R.G. and B.S.) identified all studies. Studies that appeared to fit the inclusion criteria were included for full review. Each reviewer independently selected studies for inclusion in the review (Fig. 1).
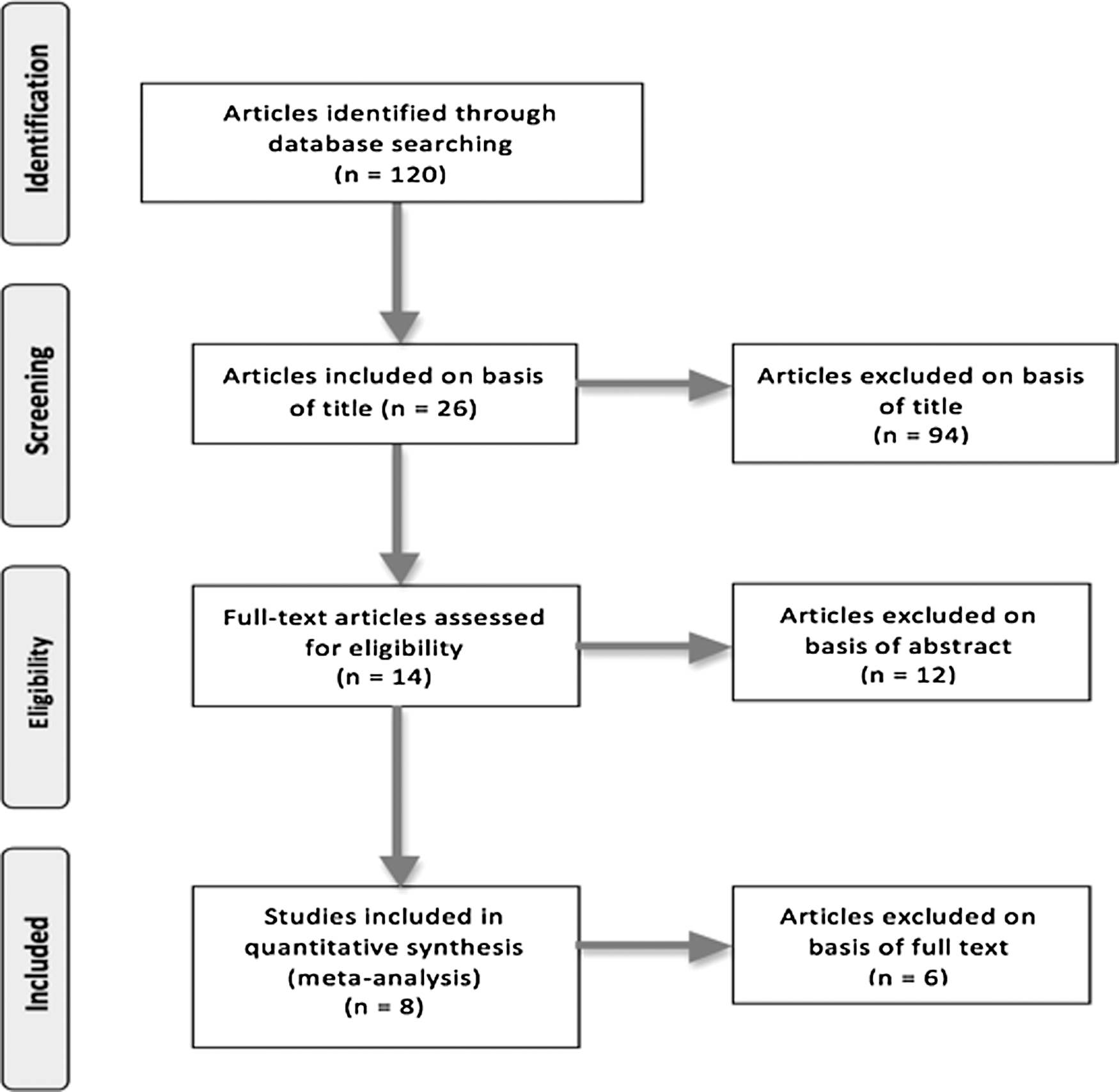
PRISMA flow diagram for article selection. PRISMA = preferred reporting items for systematic reviews and meta-analyses.
Data extraction and analysis
The following variables were extracted from each study: year of publication, country of study, type of dataset/database, study period, and treatment modality. Level of evidence was assessed using the recommendations set out by the Center for Evidence Based Medicine (CEBM). 10
Data were collated using Microsoft Excel (version 12.2.4) and analyzed using SPSS (version 21). Trends were analyzed using linear regression for the overall data and individual studies.
Results
Overall data and trends
Eight studies were identified and included for analysis (Fig. 1).
11
–18
Data were available in five studies
11,12,14,15,18
and had to be estimated in a further three studies.
13,16,17
Data were collected from various sources as follows (please see Appendix Tables A1–A9): • Australia: Medicare—includes all claimed procedures performed under a registered provider, which qualifies for a Medicare benefit. It does not include private patients.
11
• Brazil: Public Health System of Brazil (SUS) longitudinal hospital inpatient database—covers all inpatient procedures/admissions under the SUS. It does not include private patients.
12
• Canada: Ontario Health Insurance Plan, CIHI-DAD—a national database on all patient visits to acute care institutions, and NACRS—a national database on all patient visits to hospital and community based ambulatory care centers.
13
• New Zealand: The electronic surgical database at Auckland Central Hospital.
14
• United Kingdom: Health Episode Statistics—a national database covering all National Health Service (NHS) hospitals in England.
15
• United States: Nationwide Inpatient Sample (NIS)—covers roughly 20% of community hospital inpatient stays, collects data regardless of payer.
16
American Board of Urology (ABU) certifications—requires submission of 6 consecutive months of operative data before application submission.
17
Public Use Files from Centers for Medicare and Medicaid services—represents a 5% national random sample of patients using either Medicare or Medicaid.
18
Data were provided on URS, SWL, PCNL, and open stone surgery.
Ureteroscopy
Seven studies provided data on URS (Fig. 2 and Table 1). Overall URS had a 251.8% increase in total number of treatments performed from the start vs the end of the study periods (1996–2016). The share of total treatments also increased by 17%. Only the study by Ghani and colleagues 16 had a slight decrease in total number of URS procedures performed (loss of 9.4% from start to end of study); however, the share of total treatments treated with URS rose in all other studies. Linear regression analysis of individual studies demonstrated significant temporal trends in all studies. Only the study by Ghani and colleagues 16 had a negative temporal trend.

Graph showing trends of share of ureteroscopy as a percentage of total treatments.
Statistical analysis relates to change in share of total treatment. Overall trend in terms of share of total treatment is significant (R 2 = 0.20, β = 0.45, p < 0.001).
The overall temporal trend analysis showed a significant rising trend of URS over the study period (R 2 = 0.20, β = 0.45, p < 0.001).
Extracorporeal shockwave lithotripsy
Seven studies provided data on SWL (Table 2). Overall, an increase in the total number of SWL treatments performed over the study period was witnessed. However, the share of total treatments decreased by 14.5%. Of the five studies that reported on SWL figures and with the exception of the Brazilian study, which showed an increase in the overall number of SWL treatments, 12 all other studies showed a modest change in SWL figures (both in terms of number and share of total treatment) over the study period (Fig. 3 and Table 2). However, even this study showed a nonsignificant trend with stable rates of SWL. 12 Four studies showed a temporal trend of significant decrease in SWL in terms of share of total treatments, while the remaining two studies had nonsignificant trends, and therefore, the temporal trend for those studies was stable (Fig. 3 and Table 2). 11,12,14,16

Graph showing trends of share of SWL as a percentage of total treatments. SWL = extracorporeal shockwave lithotripsy.
Statistical analysis relates to change in share of total treatment. Overall trend in terms of share of total treatment was not significant.
Although the overall trend showed that SWL had decreased as a share of total treatment, linear regression analysis was nonsignificant for this despite the change in absolute and relative measures (R 2 = 0.002, β = −0.046, p = 0.40).
Percutaneous nephrolithotomy
Eight studies provided data on PCNL. As a percentage of total treatments, the number of PCNL procedures performed fell in Australia (−1.7%) 11 and New Zealand (−3.9%), 14 but rose in Brazil (9.3%) 12 and United Kingdom (148.8%) 15 (Table 3). All studies, apart from Rukin and colleagues 15 and Seklehner and colleagues, 18 had significant linear regression analysis.
Statistical analysis relates to change in share of total treatment. Overall trend in terms of share of total treatment is not significant.
Overall, PCNL had an increase in total number of treatments performed over the study period, although the share of total treatments only marginally increased by 1.3%. Linear regression analysis was nonsignificant for share of total treatment against year, and thus, the overall temporal trend was stable despite the change in absolute and relative measures (R 2 = 0.009, β = −0.97, p = 0.40) (Table 3).
Open stone surgery
Four studies provided data on open stone surgery. As a share of total treatments, open surgery decreased by 12%. Total numbers of open stone surgery procedures performed fell in the United Kingdom (−39.5%) 15 and Australia (−80.6%), 11 but rose in Brazil (+50.5%) 12 and United States (+64.3%) 18 (Table 4). However, linear regression analyses of the share of total treatments for each study demonstrated that open surgery fell significantly in all studies, apart from United States, 18 where there was a nonsignificant trend. Overall, linear regression analysis demonstrated a weak nonsignificant negative trend between share of total treatment and year (R 2 = 0.017, β = −0.13, p = 0.41).
Statistical analysis relates to change in share of total treatment. Overall trend in terms of share of total treatment was not significant.
Discussion
This is the first study demonstrating the trends in the surgical treatment of urinary stone disease across the world. Eight studies were identified from the literature demonstrating data from six countries: Australia, 11 Brazil, 12 Canada, 13 New Zealand, 14 United Kingdom, 15 and United States. 16 –18 Four modalities of treatment were identified as follows: URS, SWL, PCNL, and open stone surgery. Trend analysis with linear regression highlighted a significant increase in the proportion of URS being performed (β = 0.45, R 2 = 0.20, p < 0.001). The proportion of the remaining modalities as a share of treatment per year had nonsignificant trends overall.
The rise in urinary stone disease
The results of this study show an increase in total number of procedures performed over the past decade. This largely reflects increasing prevalence of urolithiasis. 4 –8 Furthermore, these changes are not confined to any race, gender, or age. 19 Certain key factors (and hypotheses) are associated with this evolving epidemiology. First, obesity is closely related to the risk of urinary stone formation. This positive correlation is supported by several large data series, including the NIS database, which gathered results from 20% of inpatient admissions in the United States. 20 Poor dietary patterns of industrialized countries rich in animal protein and minerals such as sodium and absence of adequate fluid intake all contribute to it. Diabetes and hypertension, also both rising in incidence, have been associated with uric acid and calcium oxalate stones, respectively. 21
The modern era of URS
While the total number of PCNL and SWL procedures has risen (+179% and +69%, respectively) over the past decade, the share of total treatment for PCNL has remained largely static (+1.3%), whereas for SWL, it has decreased (−14.5%). The findings in this review have therefore captured the modern evolution in URS. Owing to massive innovations in minimally invasive surgery, open techniques for stone disease has become almost completely obsolete in the developed world. These endourologic milestones include those related to technology, technique, and cost. The introduction of the holmium laser advanced this further and its predictability and potential soon superseded that of the lithotripter. Given these continued advancements, the therapeutic applications of URS have expanded. 22 –25 While previous EAU guidelines stated URS as a second line intervention after SWL for intrarenal stones <1.5 cm, it is now recommended as a possible first line treatment. 6 Arguably it is the intervention of choice for intrarenal stones of 1 to 2 cm. While PCNL is still accepted as the benchmark intervention for stones >2 cm, the justification for URS in this scenario has grown stronger. Previous meta-analysis by Aboumarzouk and colleagues recorded a stone-free rate of 95.7% in stones 2 to 3 cm with a major and minor complication rate of 0% and 14.3%, repectively. 26 The safety and efficacy of URS have supported for children and in pregnancy. 27,28 Bleeding diathesis does not preclude it either. It can be performed as a day case and is even feasible in patients with a solitary kidney. 29,30 In early practice, URS was limited to specialized centers, but the dissemination of this technique has allowed its wide uptake and has superseded other endourologic techniques. Development of educational courses, mentoring programs, and simulation models to enable a didactic platform to share experience and knowledge has played a key role in this. 31
Future trends
With these refinements in surgical technology set to continue, the forecast for URS is promising. Central to this will be further miniaturization of endoscopes and improvement in optics and training. 31,32 Evidence has already shown it to be cost efficient and its financial profile will improve further with reduced costs of ancillary equipment and repairs. The application of URS is likely to extend further to include more complex stones and nonindexed patients with multiple comorbidities. Increasing number of patients will undergo this as a day case procedure, and early results have supported bilateral simultaneous procedures for bilateral stone disease too. 33 Robotic URS as a nascent field, which enables control of instrument through console and joystick, has emerged as a novel adaption. Early results suggest improved ergonomics for the operator, but data on clinical outcomes are awaited. 34
Limitations and future research
With any systematic review, the overall strength or weakness relies on the included studies. Some of the studies in this review have examined robust national data that are representative of the true situation within that country. 12,15 Other studies, however, have been regional, 14 from national healthcare databases not inclusive of private patients 11,13,18 or provide a sample of the national population, 16 –18 and therefore may not reflect the true situation within the country. For example, Ghani and colleagues 16 demonstrate a proportional decrease in URS and increase in SWL, whereas Oberlin and colleagues 17 have demonstrated the opposite over a similar time period. Both of these studies utilized national samples within the United States. However, their respective datasets have been gathered from different sources. To therefore delineate which study more accurately represents the true practice in that country is extremely difficult.
With advances in imaging and newer imaging modalities, there is a higher incidence of picking up incidental stones, which is likely to have a role in these trends. 35 Similarly advances in training and better and lower cost of modern day technology have possibly influenced these trends of urinary stone disease treatment. The landscape of surgical trends will change further with the rise in minimally invasive PCNL techniques such as ultra-mini and mini PCNLs with some centers treating stones of 1 to 2 cm using this technique rather than URS. 36 Future studies should also examine national trends incorporating both public and private patient data. This is especially the case in countries where a state healthcare system (such as the United Kingdom which has NHS) is the main care provider and where majority of patients do not hold private health insurance.
Conclusion
The surgical paradigm for urinary stone disease has shifted. This study confirms the emerging role of URS, as well as the increased volume of endourologic procedures now being performed. Archived information from national databases gives invaluable insight into evolving practice patterns. Future epidemiologic studies should incorporate data from private healthcare, as well as look at the cost-effectiveness analysis of stone treatment.
Footnotes
Author Disclosure Statement
Bhaskar Somani is on the advisory board for ISIRIS. The other authors have no conflict of interest.