
Abstract
Purpose:
To evaluate in vitro the maximum pressure generated in an artificial kidney model when people of different levels of strengths used various irrigation systems.
Materials and Methods:
Fifteen people were enrolled and divided into three groups based on their strengths. Individual strength was evaluated according to the maximum pressure each participant was able to achieve using an Encore™ Inflator. The irrigation systems evaluated were as follows: T-Flow™ Dual Port, Hiline™, continuous flow single action pumping system (SAPS™) with the system close and open, Irri-flo II™, a simple 60-mL syringe, and Peditrol™. Each irrigation system was connected to URF-V2 ureteroscope, which was inserted into an artificial kidney model. Each participant was asked to produce the maximum pressure possible with every irrigation device. Pressure was measured with the working channel (WC) empty, with a laser fiber, and a basket inside.
Results:
The highest pressure was achieved with the 60 mL-syringe system and the lowest with SAPS continuous version system (with continuous irrigation open), compared to the other irrigation devices (p < 0.0001). Irrespective of the irrigation system, there was a significant difference in the pressure between the WC empty and when occupied with the laser fiber or the basket inside it (p < 0.0001). The stratification between the groups showed that the most powerful group could produce the highest pressure in the kidney model with all the irrigation devices in almost any situation. The exception to this was the T-Flow system, which was the only device where no statistical differences were detected among these groups.
Conclusion:
The use of irrigation systems can often generate excessive pressure in an artificial kidney model, especially with an unoccupied WC of the ureteroscope. Depending on the strength of force applied, very high pressure can be generated by most irrigation devices irrespective of whether the scope is occupied or not.
Introduction
I
Unfortunately, better visibility achieved with higher irrigant inflow comes with the price of increased intra-pyelic pressure, potentially causing intrarenal, pyelo-venous, and pyelo-lymphatic backflow or even rupture of the collecting system, which has a potential to cause peri-renal hematoma or urosepsis. 2,3
Sparse data are present in the literature on comparison of maximum pressure achieved in the kidney by using the different irrigation systems. The aim of this in vitro study was to evaluate the maximum pressure obtained in an artificial kidney model when people of different levels of strengths used various irrigation systems.
Materials and Methods
Fifteen people were enrolled in the study and divided into three groups based on their strengths. Individual strength was evaluated according to the maximum pressure each participant was able to achieve using an Encore™ 26 Inflator (Boston Scientific, Massachusetts) with rated inflation pressure (ATM) gauge (Group 1: 0–8 ATM, Group 2: 9–15 ATM, and Group 3: 16–24 ATM), with the relative strengths increasing from group 1 to 3.
The evaluated irrigation systems were as follows: T-Flow™ Dual Port (Rocamed, Monaco), Hiline™ (Coloplast, Denmark), continuous flow single action pumping system (SAPS™) (Boston Scientific) with the system close and open, Irri-flo II™ (Olympus, Japan), a simple 60-mL syringe, and Peditrol™ (Wismed, South Africa).
Each irrigation system was connected to URF-V2 (Olympus, Japan) ureteroscope, which was inserted, through a 10/12 Fr ReTrace® (Coloplast) ureteral access sheath (UAS), into an Urovac Bladder Evacuator (Boston Scientific) filled with saline, used as an artificial kidney model.
The evacuator cap was reinforced with a nephroscope operator channel insertion cap (Karl Storz, Germany) and a rubber cap (Cook Medical, Indiana) to provide a closed system and to prevent any leakage around the UAS. The pressure inside the bench model was measured with a pressure fiber system (St. Jude Medical) introduced into the bladder evacuator alongside the UAS. The pressure was recorded in mm Hg and was later converted to cmH2O. The artificial kidney model was sealed but the irrigant outflow was permitted through the UAS alongside the flexible ureteroscope. 4 Each participant was asked to produce the maximum pressure possible with every irrigation device. Pressure was measured with the WC empty, with a 275 μm laser fiber, and a 1.9F basket inside it.
The experiment was repeated thrice for each participant and for each irrigant system, the mean pressure was then calculated and recorded. Statistical analysis was performed using one-way analysis of variance test (with repeated measures) and data were expressed as mean (standard deviation).
Results
In this in vitro study the highest pressure was achieved with simple 60 mL-syringe system and the lowest with SAPS continuous version system (with continuous irrigation open), compared to the other irrigation systems (p < 0.0001).
Irrespective of the irrigation system, there was a statistically significant difference in the pressure between the WC empty and when occupied with the laser fiber or the basket inside it (p < 0.0001). Even when the measurements were stratified between groups, the statistical difference in the aforementioned three situations of the WC was confirmed (p < 0.05).
Moreover, the stratification between the groups with different strengths showed that the most powerful group could produce the highest pressure in the artificial kidney model with all the irrigation devices in almost any situation. The exception to this was the T-Flow system, which was the only device where no statistical differences were detected among groups (based on the physical strengths) with the WC empty or occupied with the laser fiber or basket inside it.
The overall maximum pressures and their stratification in three groups of power developed by using the different irrigation systems are reported in Tables 1 and 2 and Figures 1 and 2, respectively.
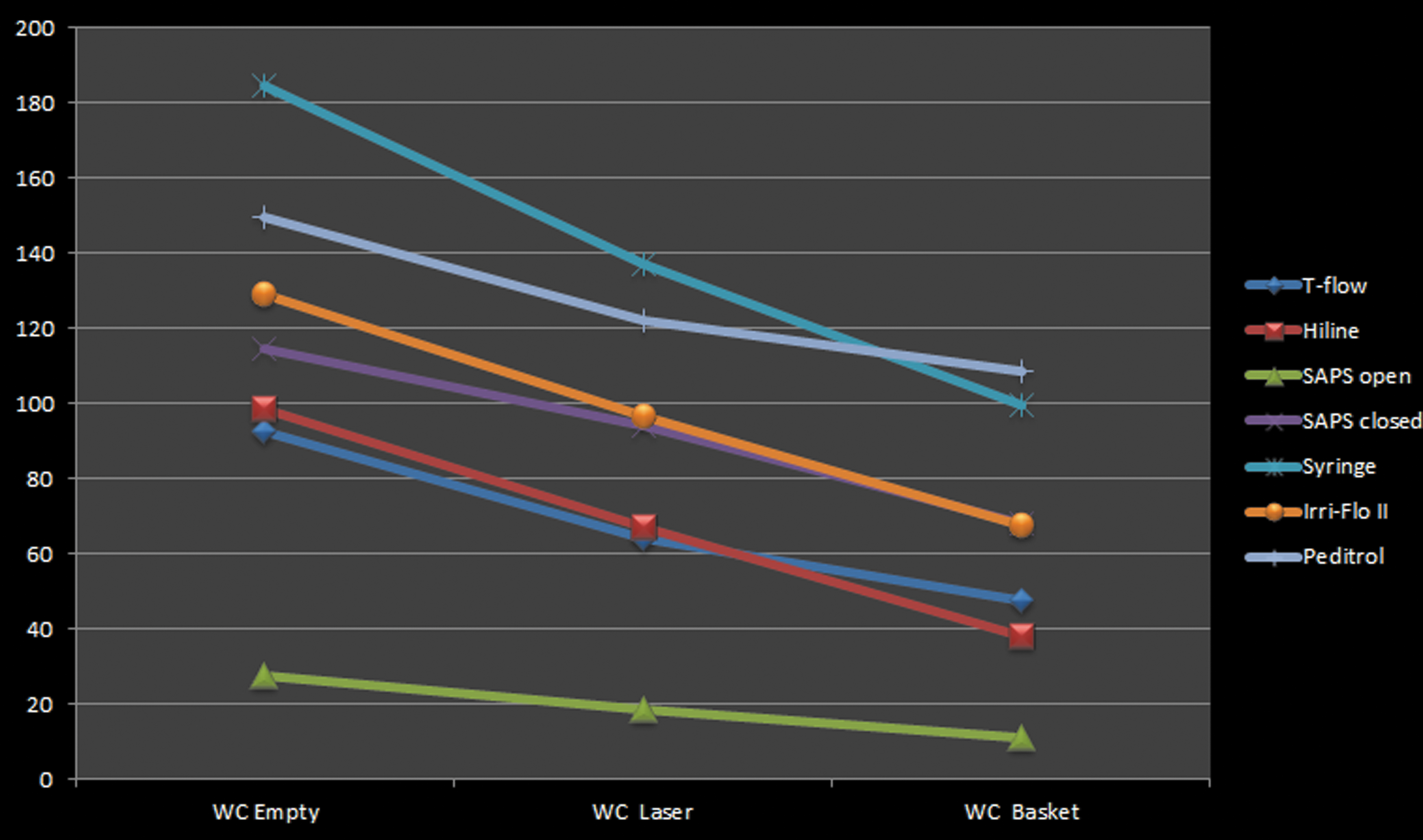
Overall maximum pressure (cmH2O) developed by using the different irrigation systems with WC empty, with laser in it, and with basket in it. WC = working channel.
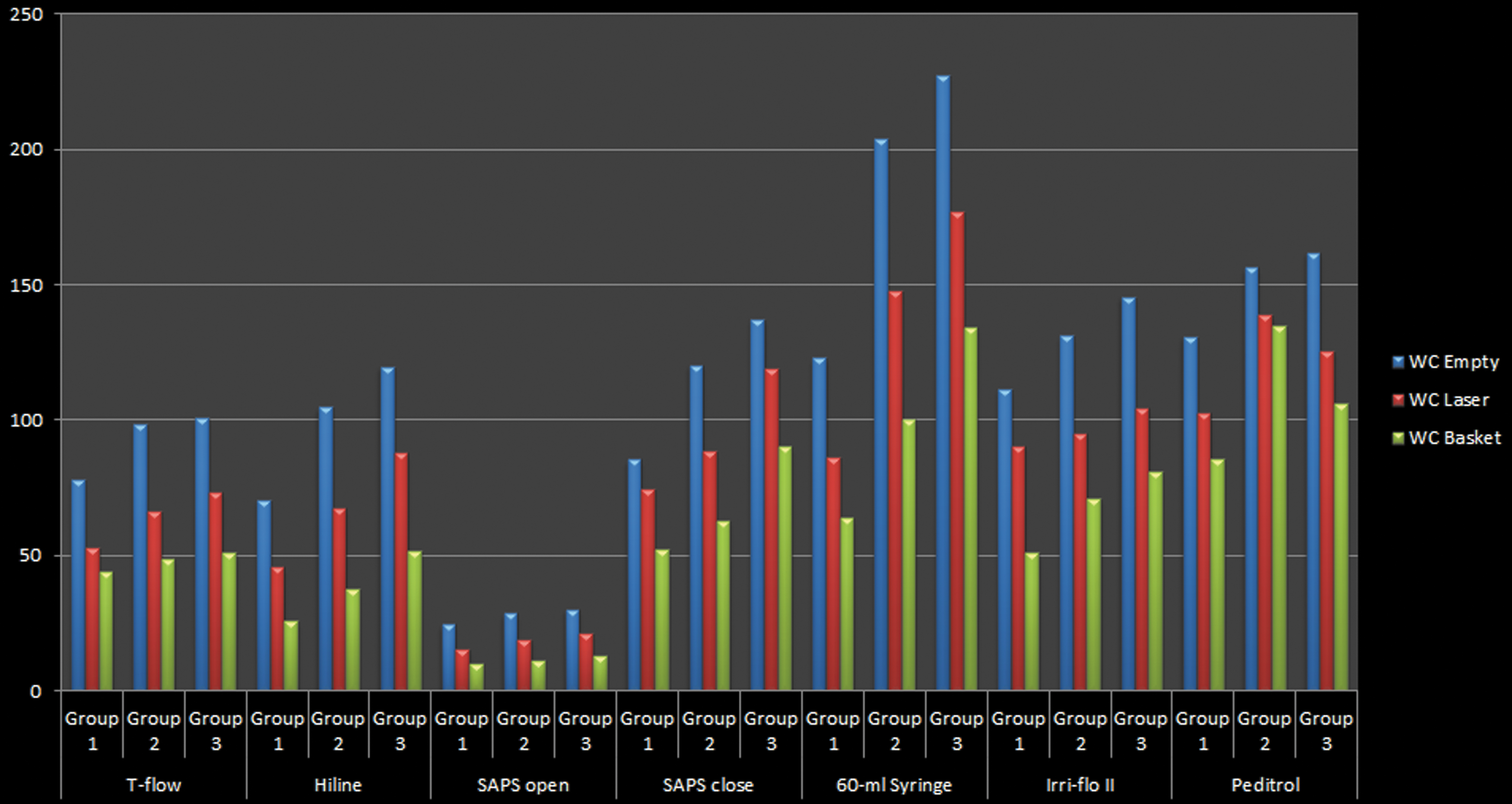
Group stratification of maximum pressure (cmH2O) developed by using the different irrigation systems with WC empty, with laser in it, and with basket in it.
Bold indicates statistical significance.
WC = working channel.
Bold indicates statistical significance.
Discussion
Meaning of our study
The importance of this study lies in the fact that during fURS, we have to be aware of which irrigation system we are using and the potential intrarenal pressure that may be developed by applying excessive force. We should therefore take into consideration the physical strength of the assistant or user who is helping or assisting with these devices. Our study shows that the simple innocuous and “so-called” safe syringe device can generate the highest pressure in all situations. Also, based on the individual strengths, a high pressure can be produced with most irrigation devices with the exception of T-Flow system. This shows that unless clinical acumen and awareness is applied, a high pressure can be achieved and applied in most situations by majority of these devices whether the WC is empty or occupied.
While a high pressure can be helpful to improve visual clarity when the WC is occupied, this elevated pressure on an empty WC can have a theoretical risk of increasing the complication rates associated with fURS. 2,3
To our best knowledge, this is the most comprehensive in vitro study that evaluates (in the same bench model) the maximum pressure developed by numerous irrigation systems using different levels of strengths achieved by the assistants, where the maximal potential force was preliminarily assessed with a device that was able to differentiate the pressure applied on it.
Clinical relevance of intrarenal pressure and comparison with other studies
Technological advances have been successful in providing flexible ureteroscopes with increasingly smaller diameters, thereby facilitating the access to the upper urinary tract with respect to the ureteral and pyelocalyceal anatomy. One of the drawbacks is a common WC for irrigation and instruments, which impacts on the overall irrigant flow. Good irrigation is vital for proper visibility and dilatation of the collecting system during fURS. Frequently, the simple gravity irrigation is not sufficient for good visualization during fURS 5 and irrigation enhancement is often required to improve the visibility of the operative field. Several irrigant systems with this purpose are currently available, but they frequently lead to an increased intrapelvic/intrarenal pressure, 6,7 that is significantly reduced when the UAS is used. With little clinical data on the effect of different enhanced irrigation system on intrarenal pressure, the safety of these devices is not well outlined.
In a previous study Wilson and Preminger described (in six patients) different intraureteral and intrarenal pressures reached with three forms of irrigation: gravity irrigation, gentle and forceful manual irrigation with a 60-mL syringe, and the roller-pump mechanical irrigation device. 7 The highest intrarenal pressure obtained was by using the 60-mL syringe. With gentle irrigation on the plunger, measurements of 85 and 115 mm Hg were reached via 3.6F and 4.0F WC respectively. With significant manual force, intrarenal pressures of 345 and 410 mm Hg were obtained via 3.6F and 4.0F WC, respectively. 7 It has to be underlined that in the aforementioned study the authors did not objectify the meaning of gentle and forceful manual pressure and they fail to mention whether the same assistant performed the manual pressure tests. Another ex vivo study evaluated the intrarenal pressure reached by using gravity drainage at 100 cmH2O, pressurized irrigant bag at 300 cmH2O, handheld 60-mL syringe and Peditrol. 6 The highest and similar intrarenal pressures were measured by using Peditrol and 60-mL syringe, but no evaluation or stratification of the pressure applied on these irrigation devices was mentioned. In the aforementioned study 6 and in another study by Auge and colleagues, 8 it was demonstrated that using an UAS significantly decreases the intrapelvic pressure during fURS.
According to our in vitro results, in this bench model the highest pressure was reached by using the handheld 60-mL syringe. We believe that, among the syringe-based systems, the large 60 mL volume of the handheld syringe is responsible for the highest pressure. The volume is six-time greater than the others syringe-based systems, which contains just 10 mL of saline solution. The lowest pressure measured was obtained by using the SAPS continuous version with continuous irrigation left open. Irrespective of the irrigation system, there was a statistically significant difference in the pressure between the WC empty and when occupied with the laser fiber or the basket inside it (p < 0.0001). Our results correlate with previously published data. Bach and colleagues showed that the use of laser fiber leads to a decrease in irrigation volume of 53.7%; moreover, loss of irrigation volume varies from 62.24% to 99.1% by using basket from 1.5F to 3.0F, respectively. 9 Similarly, group 3 produced the highest pressure with all types of irrigant devices whether the WC was empty or occupied, with the exception of the T-Flow device. No significant differences were detected among groups with the WC empty and with the fiber laser and basket inside when T-Flow device was used.
Strengths and weakness of our study
In this study, we evaluated the maximum pressure developed by various irrigation systems, using different levels of strengths achieved by the assistants, where the maximal potential force was preliminarily assessed with a device that was able to standardize the pressure applied on it. Compared to previous studies, our study standardized the user-force strength used for the measuring the irrigation pressure generated by various systems. 6,7
In our study, it was interesting to observe that the other device similar to the T-Flow, the Hiline system (both basing their concept on bulb compression for providing an extraflow), showed statistical differences in all situations analyzed among the three groups (p < 0.05). These conflicting results may be addressed to the different shape and material of the compression chamber between these two devices. Nevertheless, our study outcomes cannot be completely translated in real life efficiency of the devices, especially regarding the optimal visualization of the operative field. Hendlin and colleagues showed that, among different irrigation systems, SAPS required the fewest number of pumps per second to maintain a clear endoscopic field while the Peditrol device required the most. 10 Our study did not attempt to assess the impact of different irrigation devices on visualization of the operative field into the kidney mode. Accordingly to this limitation of the study, we cannot comment on the visibility enhancement issues related to fURS. Similarly, we did not objectively measure the flow rates in this study and perhaps future studies in this area should be done in conjunction with this parameter in the study design. 11
A weakness of this study is that our results are not in line with those previously reported in the literature. Despite the use of UAS in our bench model, higher pressures were obtained in our study when compared to previously reported studies. 6 –8 These findings could be explained due to the intrarenal pressure measurements in different situations (artificial models, cadavers, and humans). Perhaps, the characteristics of our bench model (elasticity/rigidity, size, and shape) could explain higher pressures in the artificial kidney, even with the UAS in place; consequently the pressures measured are only applicable to our model.
Moreover, another interesting issue that emerges from this study is that using Peditrol device in two out of three different situations of the WC analyzed (with the laser fiber and the basket inside the WC), group 3 did not develop the highest pressure into the artificial kidney model that was achieved by the group 2. This finding could be addressed to the fact that we stratified the groups according to the force achieved by using their hands and foot pressure measurements were not standardized.
Despite this, in the aforementioned situations of WC, statistical significant differences in pressures were detected among groups, underlining the concept that the surgeon or the assistant should pay attention to the force applied when they are using the foot-pedal irrigation device.
Areas of future research
The normal intrarenal pressure is ∼10 mm Hg 12 and the threshold for pyelovenous and pyelosinous backflow is around 30–45 mm Hg. 13 Moreover, it has been shown that during forced irrigation and laser fragmentation pressure peaks can reach up to 300 mm Hg, 14 exponentially increasing potential complications. Particularly infective risks are associated with this high intrarenal pressure during fURS. In the CROES (Clinical Research Office of the Endourological Society) study the use of UAS was shown to decrease the infective complications since it helps to decrease the intrarenal pressure, although this has been refuted in other studies. 15,16 Perhaps future prospective potentially randomized clinical studies would help to clarify this issue.
Further in vivo studies are needed to better establish the real difference among the irrigation devices regarding the intrarenal pressure, impact of the experience and physical strength of the assistant, and correlation with the devices efficiency in maintaining optimal operative field visualization. Nevertheless, it is essential to be gentle during the irrigation without exerting excess force on irrigation enhancement devices. This is especially important because another member of the team who is potentially less experienced and who could involuntarily apply too much force on the irrigation device, leading to extremely high intrarenal pressure during fURS, often assist endourologists. Consequently, it is of utmost importance for the surgeon to be aware of the irrigation enhancement device properties in conjunction with the experience and physical strength of their assistant. Training, education, and awareness can lead to better coordination, teamwork, and improved patient-related clinical outcomes.
Conclusion
The use of common irrigation systems can often generate excessive pressure especially with an unoccupied WC of the ureteroscope. Depending on the strength of force applied, very high pressure can be generated by most irrigation devices irrespective of whether the scope is occupied or not.
Footnotes
Acknowledgments
The authors thank Mr. Lorenzo Proietti for his iconographic support. Petra Group: O.T., B.S., S.P., L.D., Guido Kampius, Julien Letendre, Jonathan Cloutier, Emre Sener, Achilles Ploumidis, Steeve Doizi, Tzevat Tefik, Saeed Al-Quahtani, Luca Villa, Alexander Thomas, Salvatore Butticè.
Author Disclosure Statement
S.P., L.D., S.B., M.T., E.E.: nothing to disclose. O.T.: consultant for Coloplast, Rocamed, Olympus, Lumenis, Boston Scientific, Biohealth, EMS. G.G.: consultant for Coloplast, Rocamed, Olympus, Lumenis, Boston Scientific, Karl Storz, Cook Medical. B.S.: consultant for Isiris system (Coloplast).