
Abstract
Introduction:
Immediate ureteroscopic treatment for patients presenting to the emergency room with symptomatic ureterolithiasis is more commonly being utilized. Recent reports demonstrate good efficacy for emergency ureteroscopy (URS); however, preoperative predictors of treatment success have not been described. In this study, we report our multicenter experience with emergency URS and identify predictors of successful treatment. We also describe the Emergency Ureteral Stone Treatment (EUST) score, which integrates these predictors and stratifies patients into those that are likely and unlikely to have successful treatment.
Materials and Methods:
Laboratory and radiographic data for all patients who underwent emergency URS for acute symptomatic ureterolithiasis from 2010 to 2015 were reviewed. Statistical difference among parameters for patients who were stone free (SF) and not SF was assessed with the Student's t-test. Cutoff values for significant predictors were determined using sensitivity and specificity analysis. The EUST score was determined based on the number of cutoffs a patient was below.
Results:
Two hundred two of 247 patients (81.8%) were SF. Two complications (ureteral perforation) occurred. Stone size, duration of symptoms before presentation, and serum white blood count at presentation did not affect SF rates. 95.5% of the treatment failures were attributed to a tight ureter preventing stone access. Patients who received alpha blockers before treatment were more likely to be SF (98.0% vs 55.5%, p < 0.01). Periureteral density (PUD) was lower in SF patients (2.8 HU vs 19.6 HU, p < 0.01), whereas the increase in serum creatinine from baseline (ΔCr) was greater in non-SF patients (0.44 mg/dL vs 0.20 mg/dL, p < 0.01). EUST score of 0, 1, and 2 correlated with SF rates of 20.6%, 81.9%, and 99.2%, respectively.
Conclusions:
Combined consideration of PUD and ΔCr with the EUST score can assist in selecting optimal candidates for immediate ureteroscopic management. Administration of alpha blockers before surgery may improve success rates by providing preoperative ureteral dilation.
Introduction
O
Patients with intractable renal colic and no clinical evidence of sepsis are usually admitted to the hospital and provided a trial of medical expulsive therapy. Failure to pass the stone prompts intervention, which is oftentimes ureteral stent placement without an attempt at stone treatment. Possible reasons for this practice pattern include concern for higher complication rates and diminished efficacy due to a presumed higher degree of acute ureteral inflammation. Interval stent placement allows passive ureteral dilation that may facilitate easier access to the calculus.
Over the last two decades, several factors have contributed to improved stone-free (SF) rates with ureteroscopic treatment of stones. These include miniaturization of ureteroscopes, improved fragmentation and basket devices, and improved surgeon familiarity with the procedure. 3,4 Contemporary reports have also described nearly equivalent SF and complication rates among patients treated urgently with ureteroscopy (URS) (commonly described as “emergency URS”). 5 –10 Benefits to this approach include eliminating the need for a second procedure, decreased indwelling stent time, and a subsequent improved patient quality of life.
Predictors for emergency URS have not been described. With the growing incidence of patients presenting to the Emergency Department with symptomatic ureterolithiasis and the expanding body of literature supporting efficacy of URS in this setting, more urologists are likely to consider performing emergency URS. Thus, it would be beneficial to be able to stratify patients into risk categories for being SF after emergency URS. In this study, we provide our multicenter report of emergency URS. We describe three preoperative predictors of treatment success as well as the Emergency Ureteral Stone Treatment (EUST) score, which incorporates two novel predictors—change in serum creatinine from baseline (ΔCr) and periureteral density (PUD).
Materials and Methods
After approval from the respective institutional review boards, our records were queried for all patients who underwent emergency URS from 2010 to 2015. Inclusion criteria were presentation to the emergency room with acute renal colic from ureterolithiasis, age >18, no clinical evidence of sepsis, and diagnosis made with CT scan. All patients were admitted directly from the emergency room and underwent surgery within a few hours of admission. No patient was electively scheduled.
Chart review was performed for all identified patients. Clinical parameters, including duration of colic before presentation, previous history of stones, previous stone surgery, and the number of presentations to the Emergency Room before admission, were obtained from the electronic medical record.
Laboratory data obtained at the time of presentation included urinalysis, basic serum chemistry panel, and complete blood count. Change in serum creatinine from baseline (ΔCr) was defined as the difference between the serum creatinine at the time of presentation and the baseline value.
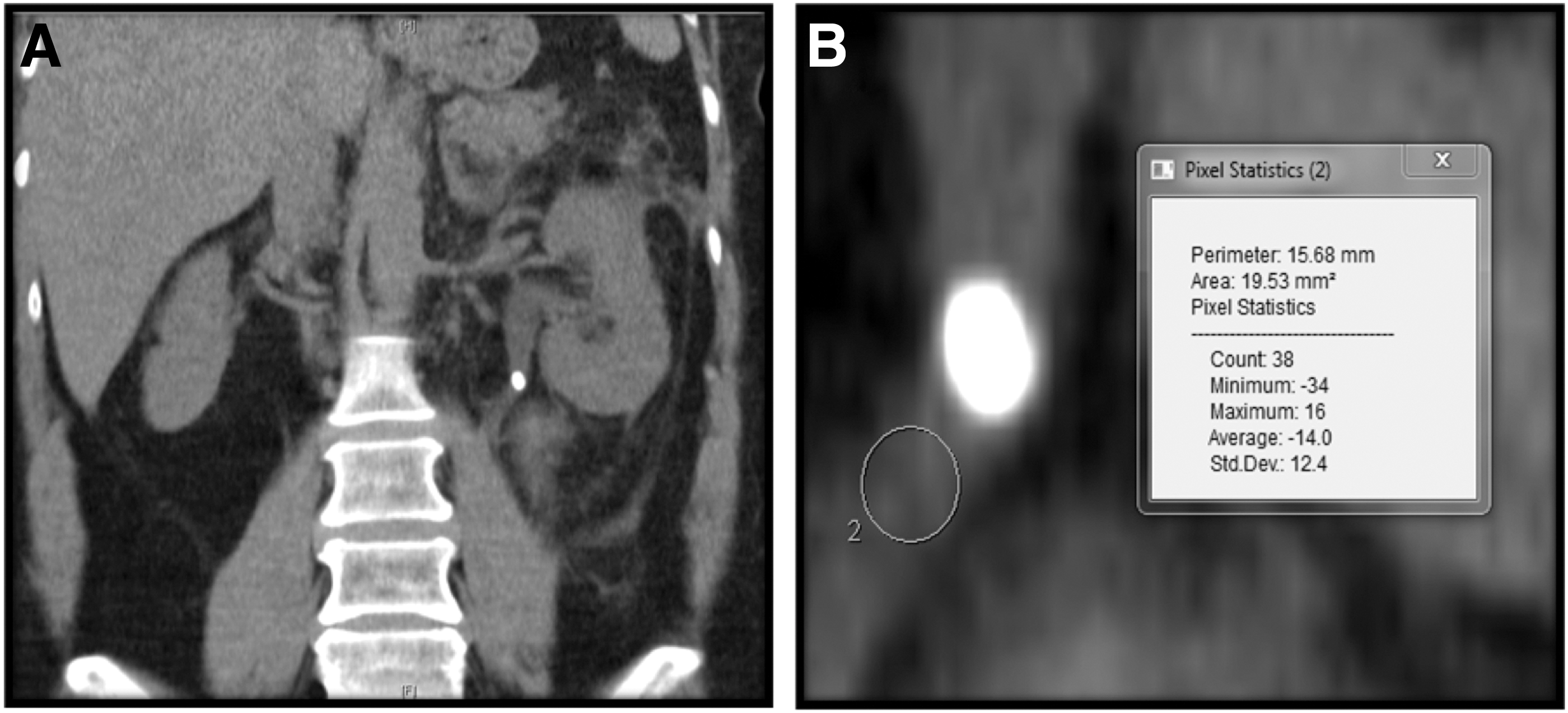
Noncontrast CT scan was used to ascertain stone location, size, and PUD. Stone size was independently measured as maximal stone diameter on either axial or coronal images. PUD was defined as the average Hounsfield units of the ureter immediately distal to the stone (technique described in Fig. 2).
All procedures were performed under general anesthesia. The use of muscle relaxation and/or endotracheal intubation was determined based upon surgeon preference. Unless warranted by an intraoperative complication (i.e., ureteral perforation), antibiotic prophylaxis was limited to a single perioperative dose of a fluoroquinolone or first-generation cephalosporin. Both 6.4F semirigid ureteroscopes and 5.3F flexible ureteroscopes were readily available for use. Intracorporeal lithotripsy was accomplished with holmium:YAG laser using 200 or 365 micron fibers.
Intraoperative findings such as ureteral narrowing and surgeon interpretation of treatment success were determined from the operative report. Postoperative complications were assessed by review of the operative note, Emergency Department records, and follow-up notes from the urologist. Patients were considered SF if the following criteria were met: (1) no evidence of residual stones as documented by the operating surgeon, (2) no evidence of residual stones on postoperative KUB (kidney, ureter, and bladder radiograph) or no evidence of hydronephrosis/residual stones on ultrasound (typically performed 4–6 weeks after surgery), and (3) no clinical symptoms to suggest residual ureteral stones (i.e., persistent renal colic, which would prompt further imaging).
Statistical significance was determined using Student's t-test. Cutoff values for ΔCr and PUD were ascertained with sensitivity and specificity analysis. EUST score was based upon the number of cutoffs that a given patient was below (0, 1, or 2, see Fig. 1)
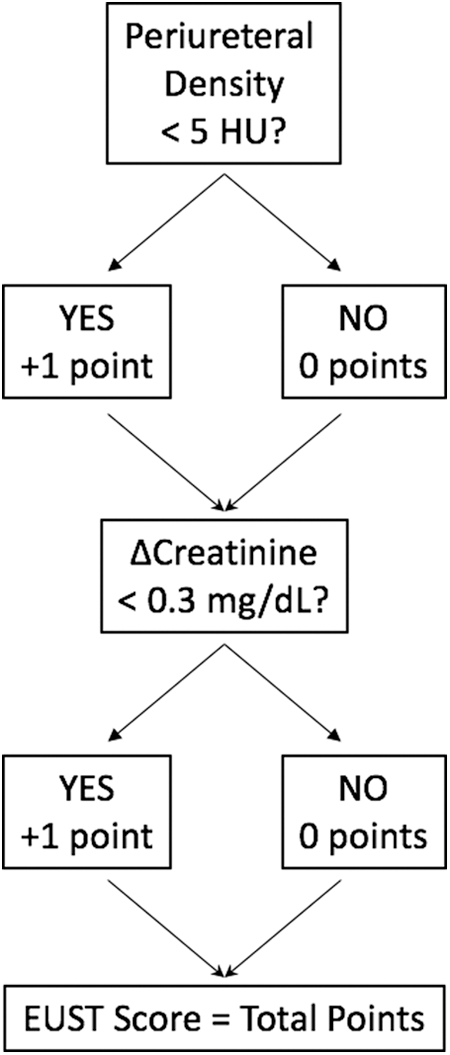
Flowchart for calculating the EUST score. EUST = Emergency Ureteral Stone Treatment.
Results
Two hundred forty-seven patients met inclusion criteria. Average age for this cohort was 52.7 years (range 22–90 years, Table 1). Fifty-two percent of the patients were male.
Where applicable, values reported as average (standard deviation, range).
Average stone size was significantly larger for proximal stones compared with distal stones (p = 0.02).
Both complications were contrast extravasation on retrograde pyelography after failed attempt to pass a wire.
ED = Emergency Department; WBC = white blood count.
Mean stone size for the study population was 5.8 mm. Among the treated stones, 116 were proximal, 24 were in the mid-ureter, and 107 were distal. Proximal ureteral stone size was significantly larger than the distal stones (6.3 mm vs 5.4 mm, p = 0.02). A flexible ureteroscope was used for 99 of 116 patients with proximal stones (85.3%), 14 of the 24 mid-ureteral stones (58.3%), and none of the distal stones.
Two hundred two of 247 patients were SF (81.8%). Ureteral narrowing preventing access of the ureteroscope to the calculus was the reason for treatment failure in 43 of 45 (95.5%) patients who were not SF. Five patients with mid-ureteral or proximal ureteral stones had balloon dilation of the distal ureter performed. For patients with narrowed areas just proximal to the stone, dilation was not performed due to the concern of pushing the stone into the ureteral wall. Of the five patients who had distal ureteral dilation, three ultimately failed (due to narrowing just proximal to the stone) and two were successfully treated.
SF rates were lower for proximal (72.4%) and mid-ureteral stones (75.0%) in comparison to distal stones (93.5%, p < 0.001 and p < 0.01, respectively; Table 2). Intraoperative complications were limited to two patients for whom extravasation was noted on retrograde pyelography after lithotripsy of proximal calculi. No postoperative readmissions were noted, although four patients (1.6%) were treated for urinary tract infection. All, but one patient (98.7%) received a stent postoperatively; this patient had minimal ureteral edema and an uncomplicated procedure, obviating the need for stent placement.
Meta-analysis of six studies from 2007 to 2011 that considered emergency ureteroscopy.
p Values in comparison of stone-free rates: proximal vs distal, p < 0.001; mid vs distal, p < 0.01; proximal vs mid, p = 0.79.
Intraoperative complications, including six false passages and three mucosal injuries.
Postoperative complications, 76% for sent pain and 14% for infection.
No difference was noted in patient age and gender, and incidence of a previous ureterolithiasis (including ipsilateral calculi) between patients who were SF and not (Table 3). Similarly, the duration of symptoms before the Emergency Department visit and previous presentations to the Emergency Department during the same episode of acute colic were not different between the two groups. Interestingly, the incidence of previous ipsilateral URS was higher among SF patients than those who failed treatment, although this difference did not achieve statistical significance (21.2% vs 11.1%, p = 0.08).
Factors associated with significant difference highlighted in bold.
No difference was observed in stone size between the SF and non-SF groups. Among SF patients, the increase in both creatinine from baseline to presentation (ΔCr) as well as PUD measured on CT scan (PUD, Fig. 2) was significantly different in comparison to non-SF patients (2.8 HU vs 19.6 HU, p < 0.01 and 0.20 mg/dL vs 0.44 mg/dL, p < 0.01, respectively). The difference was even more notable when considering only proximal and mid-ureteral stones (−0.85 HU vs 12.9 HU, p < 0.01 and 0.22 mg/dL vs 0.55 mg/dL, p < 0.01). No difference in the serum leukocytosis or left shift was observed between the SF and non-SF patients.
98.0% of patients who were SF received an alpha-blocker before surgery, in comparison to only 55.5% of patients who were not SF (p < 0.01). Patients who did not receive an alpha-blocker before emergency URS had an SF rate of 16.6%, whereas those who received an alpha-blocker had an SF rate of 88.7% (p < 0.01). No difference in SF rates was noted between patients who received an alpha blocker within 24 hours of surgery and patients who had been started on an alpha-blocker at a previous emergency visit (88.1% vs 90.0%, p = 0.863). No difference in SF rates was noted between patients treated by urologists who had completed an Endourology fellowship and those who had not.
Receiver operator characteristic curves were used to generate cutoff values for ΔCr and PUD. Using cutoffs of 0.3 mg/dL and 5.0 HU, respectively, an EUST score of 0, 1, or 2 was assigned to each patient based upon the number of cutoffs their ΔCr and PUD were below. EUST score of 0, 1, and 2 correlated with SF rates of 20.6%, 81.9%, and 99.2%, respectively (Table 4). Thirty-four patients had EUST score of 0, 94 had a score of 1, and 119 had a score of 2. The difference in SF rates was statistically significant between all EUST scores.
comparison of stone-free rate for EUST score of 0 & 1 and 0 & 2.
Comparison of stone-free rate for EUST score of 1 and 2.
EUST = Emergency Ureteral Stone Treatment.
Discussion
Mirroring the rise in the incidence of kidney stone disease is the rate of Emergency Department visits for symptomatic ureterolithiasis. 1,2 It has been demonstrated in several series that URS can be safe and effective in the setting of emergent presentations with colic and no infection. 5,6,10 We sought to assess whether there were accurate predictors of successful URS in this setting.
Our data demonstrated an SF rate of 81.8% among 247 patients treated with emergency URS. The observed SF rate appears to be lower than some modern series studying the efficacy of emergency URS. A closer examination of these studies and our data reveals that the overall success rate in our series is influenced by the higher proportion of patients with proximal stones (47% overall), in whom the SF rate was 64.7%. In reports by Guercio et al. and Al-Ghazo et al., only 19% and 20% of patients had proximal stones in their series. Lower SF rates were noted for these patients in comparison to those with stones in more distal locations. 5,6 In the most recent series, Zargar-Shoshtari and colleagues performed emergency URS on 394 patients and reported SF rates of 60% for patients with proximal stones. 10 Thus, after a critical analysis of the data, the overall SF rates by location in our study closely align with those noted in other studies.
Our data indicate that preoperative administration of alpha-blockers was associated with a significant improvement in SF rates. Given that the administration of an alpha-blocker was the only factor in this study that can be controlled preoperatively by the provider, it appears reasonable to suggest that all patients under consideration for emergency URS receive an alpha-blocker before surgery. Animal studies have demonstrated that alpha-blockers relax ureteral spasm. 11 Given that nearly all treatment failures in this study (95.5%) were secondary to ureteral narrowing that could not be bypassed, it is possible that the beneficial effect observed with alpha-blockers is related to pharmacologic ureteral relaxation that allows ureteroscopic access to the calculus. Interestingly, whether patients had received an alpha-blocker a few hours before their procedure or if they had been taking the medication for several days, SF rates were similar (90% vs 88%, respectively). This similarity in success rates suggests that the duration of administration may not have as strong an effect on its efficacy in promoting treatment success. Although steady-state concentrations for tamsulosin are achieved after 5 days, peak serum concentrations of this drug are achieved relatively quickly (4–5 hours).
In this study, we describe a new metric, PUD. PUD is determined by measuring the density (in Hounsfield Units) of the ureter distal to the obstructing calculus (Fig. 2). PUD was significantly higher among patients that failed treatment. A higher PUD may represent a more inflammatory environment distal to the stone, with resultant ureteral spasm and narrowing, which may preclude endoscopic access to the stone. A lower PUD may represent more urine being present in the ureter distal to the stone, suggesting a wider passage for the ureteroscope to the stone.
ΔCr is another novel predictor of treatment success described in our report. Although contralateral hyperfiltration assists in maintaining renal function during unilateral ureteral obstruction, patients with higher grade obstruction have a greater decline in renal function. 12 Thus, a greater ΔCr may indicate a tighter and therefore more challenging ureter to traverse with a ureteroscope and may explain its association with treatment failure.
Interestingly, stone size was not a significant predictor of treatment outcome in this study. Other studies have also noted high emergency URS SF rates in patients with large stone burdens. Yang and colleagues described an SF rate of 91.8% for a cohort of 49 patients where the mean stone size was 14.8 mm. 9 In contrast, however, a multicenter study of 9681 patients undergoing URS showed a significant difference in SF rates between patients with stones ≤10 mm and those with stones >10 mm, regardless of stone location. 13 The absence of predictive power for stone size in our cohort may be attributed to the fact that the average stone size was smaller (5.6 mm) and there were only a few stones larger than 10 mm. Thus, it is less surprising that ureteral narrowing becomes the top reason for treatment failure in our series, as once the stone is accessed, treatment is relatively straightforward.
Also of interest from this study is the rate of postoperative stenting. In our study, 244 of 247 patients (98.7%) received had a Double-J stent placed after URS. The rationale for stent placement was the higher likelihood of ureteral colic secondary to ureteral inflammation. Stent rates from other studies were lower and there was not an increase in colic-related complications. The rationale for not placing a stent was that treatment shortly after the onset of acute colic allows removal of calculus before the development of significant inflammation. These results are interesting and suggest another area of further evaluation for emergency URS.
As a predictive score, the EUST score demonstrates stronger predictive value than either PUD or ΔCr alone (Fig. 3). In evaluating the best use of the EUST score, it appears that it may be most useful for patients with mid- or proximal ureteral stones. First, these patients demonstrate the greatest difference in ΔCr and PUD. Second, the SF rate for patients with distal stones was effectively high (93.5%) and distal URS is less technically challenging, which suggests that emergency URS may be worthwhile for most patients with distal stones. Finally, for patients with distal stones, there is a greater challenge in drawing a region of interest of the ureter below a distal stone that does not include the bladder, which may limit accurate application of the EUST score. Thus, consideration of these factors suggests that the greatest utility for this score would be in determining whether to stent or proceed with emergency URS in the patient with a mid-ureteral or proximal stone.
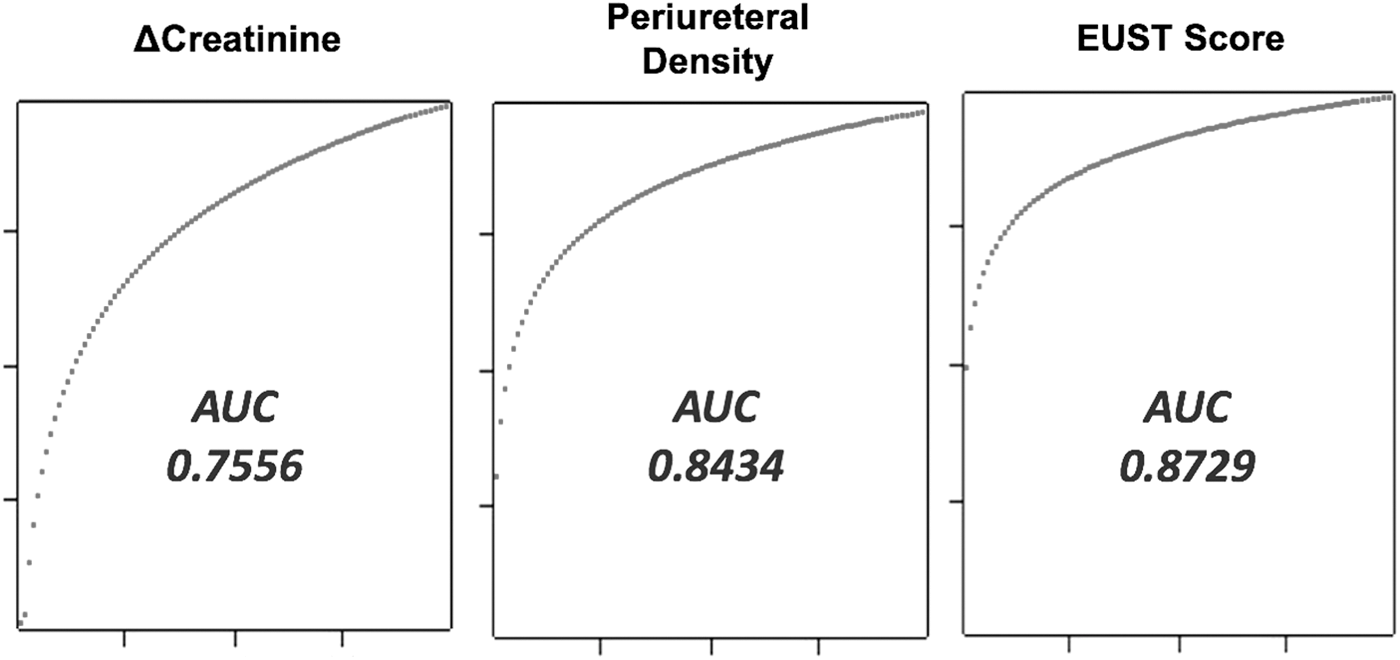
Comparison of receiver operator characteristic curves for predictors of success in emergency ureteroscopy. AUC = area under the curve.
The main benefit of this study is the identification of three predictors of treatment success in emergency URS. One is easily modifiable (administration of alpha-blockers preoperatively) and two are variables that can be considered preoperatively in nearly all patients eligible for this procedure. The EUST score allows a provider to consider both PUD and ΔCr in tandem to facilitate optimal patient selection for emergency URS vs only stent placement.
Selection bias is a limitation to this study. Surgeon judgment was used to determine whether a patient would undergo URS instead of only ureteral stent placement. It is possible that a patient had previously tolerated a stent poorly in the past or they were known to have had a previously successful URS, which could then prompt the surgeon to proceed with an emergency URS. In addition, although our definition of SF was fairly strict (as it relied upon a combination of operative findings, postoperative ultrasound and/or KUB, as well as an absence of clinical symptoms such as renal colic), it may still slightly overestimate SF rates as noncontrast CT scans were not routinely performed.
Conclusions
Administration of an alpha-blocker before an emergency URS should be considered as it appears to facilitate access of the ureteroscope to the obstructing stone. Combined consideration of PUD and ΔCr with the EUST score stratifies patients into those who are likely to have successful treatment vs those who may benefit from prestenting before definitive treatment.
Footnotes
Author Disclosure Statement
No competing financial interests exist.