
Abstract
Introduction:
Ureteral stenting is a common procedure in urology. The cystoscopic removal of Double-J stents (DJ) causes unpleasant side effects with a negative impact on patient's quality of life. The aim of our study was to evaluate this newly developed magnetic DJ and compare it with a standard DJ regarding quality of life with indwelling DJs as well as discomfort during the removal.
Material and Methods:
The magnetic DJ (Blackstar, Urotech [Achenmühle, Germany]) is a standard 7F ureteral stent with a small magnetic cube fixed through a string on the loop of the distal part of the stent. For DJ removal, a special catheter-like retrieval instrument with a magnetic tip is inserted, the two magnets connect and the retrieval instrument is removed with the DJ. We first tested this DJ in 20 cases. Afterward we evaluated 40 consecutive cases that required a DJ placement after ureterorenoscopy in a prospective randomized manner. The quality of life was assessed by the ureteral stent symptom questionnaire. A visual analogue scale was used to document the pain by DJ removal.
Results:
There was a significant difference regarding the pain location with the indwelling DJ (p = 0.038). The maximum pain was located in the lower abdomen and/or around the bladder (48%) with the magnetic DJ, whereas the standard DJ caused flank pain in 54% of the patients. The mean time for the magnetic DJ removal including preparation and cleaning as for a transurethral catheter insertion was 9.55 [7–14] minutes, whereas the mean time for the cystoscopic DJ removal was 21.35 [18–30] minutes. The pain caused by the removal of the magnetic DJ was significantly less than that caused by the cystoscopic DJ removal (p = 0.019).
Conclusion:
The discomfort caused by the indwelling magnetic DJ is comparable with that caused by the standard DJ. However, the magnetic DJ removal is less painful and faster.
Introduction
A
The idea to remove a DJ by using two magnets has been tried for implementation for more than 10 years. 6 No feasible product has been developed so far, which combines the idea of connecting magnets without additional discomfort to the patient. With the development of small magnets with enough power to remain together, the idea could be realized. The aim of our prospective, randomized study was to assess the functional efficacy of a newly developed DJ stent, which allows for removal without cystoscopy. The impact on patient's quality of life regarding stent- and stent-removal-related symptoms, as well as the DJ removal, was especially addressed.
Material and Methods
The magnetic DJ (Blackstar, Urotech [Achenmühle, Germany]) is a standard 7F ureteral polyurethane stent. A cylinder-shaped magnet is fixed through a string on the loop of the distal part of the stent. According to the length of the stent, the size of the magnet ranges between 7F and 9F (Fig. 1): • 9F: external diameter 3 mm, internal diameter 1.42 mm, length 4.5 mm, volume 31.8 mm3
• 7F: external diameter 2.33 mm, internal diameter 1.14 mm, length 3.5 mm, volume 14.9 mm3

Magnets on retrieval device and DJ (Blackstar, Urotech (Achenmühle, Germany)).
For removal, a specific catheter-like retrieval device made of soft polyurethane is used (Fig. 2). It consists of a Tiemann tip, 30° with a magnetic tip on the end. When the retrieval device is inserted, both indwelling magnets connect and the catheter can be removed together with the DJ.

Retrieval device and magnetic DJ (Blackstar, Urotech (Achenmühle, Germany)).
The removal of the magnetic DJ was performed in the out-patient clinic. The setting is comparable to a catheter insertion. The patient was laying straight on the back in a supine position. The procedure was first performed by a urologist in the pilot study and later by a nurse. A urologist was always present. The standard stent was removed in lithotomy position by a urologist in an endourologic intervention room.
The first case was performed under fluoroscopic control (Fig. 3). The other procedures were performed without fluoroscopy. You can either hear a slight “click” or feel, when the two magnets link to each other. Different DJ sizes from 4.8F to 7F with a length of 10 to 26 cm are available. Retrieval devices are available in 9F or 15F with a length of 40 cm.

First case: connecting magnets under fluoroscopic control.
According to the manufacturer of both stents (Urotech, Achenmühle, Germany), the costs of the regular stent are 20 Euro (€), including guidewire and pusher, whereas the magnetic DJ costs about € 80, including the retrieval device.
We first tested the DJ in 20 consecutive cases with an indication for a DJ placement after a URS for stone removal and removed it the first day after surgery. Afterward, we performed a prospective randomized trial with 40 consecutive patients from October 2013 to October 2014. All patients underwent a URS for stone removal. Either a standard or a magnetic DJ was inserted. Indication for a DJ insertion was made by surgeons' intraoperative decision.
The patients were randomized in a consecutive manner. Randomization was blinded for the patient. The surgeon knew up front which stent should be placed, if a DJ placement was necessary. The patients, who did not get any stent, were not enrolled in any study group.
The DJ removal was performed 7–14 days after surgery.
We measured the time of the DJ removal, which includes patient and table preparation. Cystoscope cleaning time was not measured in this setting.
Quality of life with the indwelling DJ was assessed by using the ureteral stent symptom questionnaire (USSQ). 8 –10 This questionnaire includes 6 sections with a total of 48 items, covering voiding symptoms, pain, overall general health status, work performance, sexual health, and additional problems. A German version was handed out to the patient after stent placement and collected at the day of DJ removal. 11 The questionnaire was filled out at least 5 days after the DJ placement to rule out the influence of the URS itself. After DJ removal, a visual analogue scale (VAS) was used to document the discomfort caused by the DJ removal. Exclusion criteria were patients less than 18 years, pregnant women, or sheltered patients. All patients gave their informed consent. The study was approved by the local ethics committee (No. 2014-414M-MA-§23b MPG).
In our first study phase, 20 patients were enrolled. In the second study phase, 40 patients were randomized into two groups. Twenty magnetic and 20 standard DJs were placed after a URS with stone removal. The DJ was removed within 7–14 days after the procedure. No transurethral catheter was placed after the URS.
The Pearson's chi-square test and the Cochran-Armitage Trend test were used for statistical analysis. The statistical analysis was performed by using the software SAS JMP (SAS Institute, Cary, NC).
Results
We placed 40 magnetic DJs and 20 standard DJs without any intra- or postinterventional complications. An early stent removal or replacement was not needed.
The mean age of the first study group (18 male, 2 female) was 48 [23–75] years with a mean body mass index (BMI) of 28.9 [22–38] kg/m2. In the second phase, the mean age of the magnetic DJ group (14 male, 6 female) was 47 [29–70] years with a BMI of 27.15 [16–38] kg/m2, and 48 [23–78] years with a BMI of 27.15 [19–42] kg/m2 in the standard DJ group (15 male, 5 female).
During the stent removal, no significant difference regarding pain between male and female was found (p = 0.695). The operative time was slightly different in both groups, with a mean time of 61.85 [17–160] minutes in the magnetic and 54.65 [13–95] minutes in the standard DJ group.
In the first group, we collected 16 USSQs and VASs. A total of 81.25% of this group did not complain about pain-related symptoms with the indwelling DJ. Urgency was reported in 43.75% of patients. The median pain score reported during DJ removal on the VAS was 2 [0–8].
In the second part of the study, 94.74% (n = 18) of the patients with the magnetic DJ and 85% (n = 17) of those with the standard DJ returned the USSQ and VAS questionnaire. There was a significant difference regarding the pain location with the indwelling DJ (p = 0.038). The magnetic DJ caused no pain in 16.67% (n = 3). A total of 48% patients (n = 13) complained about pain in the lower abdomen and/or around the bladder. A total of 18% patients (n = 5) described pain in the flank and 3.7% (n = 1) at the penis. The standard DJ caused no pain in 11.76% of patients (n = 2) and a maximum pain around the flank in 54% of patients (n = 15). A total of 14.29% of patients (n = 4) described pain in the groin and the penis/genitals. The detailed data are shown in Figures 4 and 5.
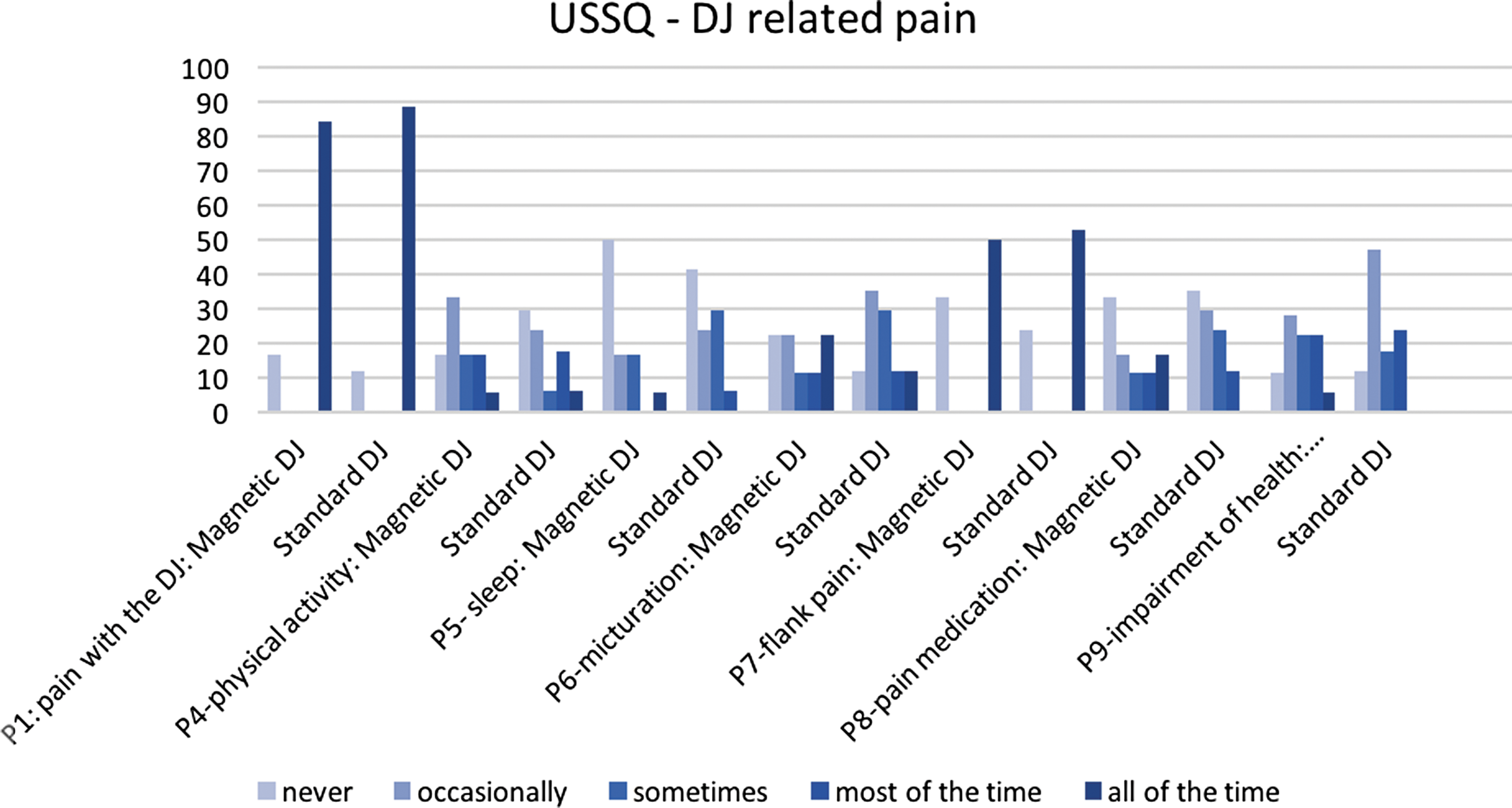
Detailed data of the USSQ different pain questions comparing the standard and magnetic DJ. The results are listed in percentage of each study group. P3 (pain scale) with the DJ is described in the result section. USSQ = ureteral stent symptom questionnaire.
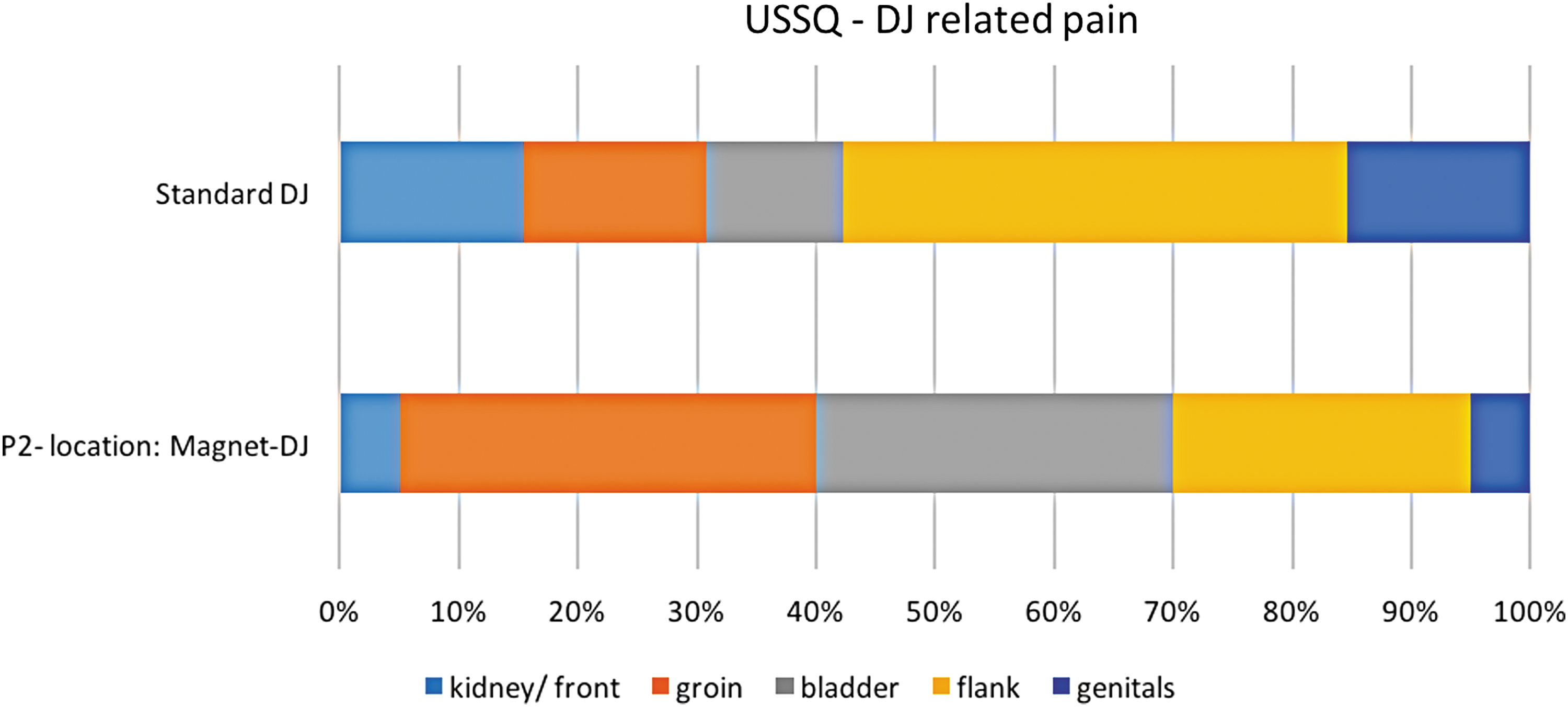
Detailed data of the USSQ pain section according to the pain location comparing the standard and magnetic DJ.
On the pain scale (Question P3) from 0 to 10, although 0 means no pain and 10 a maximum of pain, no significant difference could be shown (p = 0.156). With the magnetic DJ, the mean pain was stated at 3 [0–9], with the standard DJ at 5 [0–8], respectively.
The magnetic DJ showed no effect on the sexual life, although we must mention that 61.11% (n = 11) did not have an active sexual life before implantation of the magnetic DJ. A total of 16.67% did not have sex because of the implantation of the magnetic DJ. There was no significant difference (p = 0.486) compared with the standard DJ, whereas 58.82% (n = 10) did not have an active sexual life and 35.29% stopped having sex because of the DJ.
The mean time for the magnetic DJ removal including preparation and cleaning as for a transurethral catheter insertion was 9.55 [7–14] minutes, whereas the mean time for the cystoscopic DJ removal was 21.35 [18–30] minutes.
There was a significant difference (p = 0.019) regarding the pain caused by the DJ removal. The median number on the VAS for the magnetic DJ removal was 3 [0–6], whereas the median number for the cystoscopic DJ removal was 4 [1–8].
In 19 out of 20 cases, the removal was effective. In one patient with a magnetic DJ, a cystoscopy was needed. The retrieval instrument could not be inserted into the bladder because of a big median lobe of the prostate. Every other removal was without complications and could be performed by our trained urologic nurses.
A cost analysis at our institution calculated a reduction of € 101.41 using the magnetic DJ. As there was no need for a urologist, an operating room, a cystoscope and, therefore, no sterilization, this reduction is feasible. DJ removal with a cystoscope including sterilization costs € 193.75, whereas the cost of a magnetic DJ removal is € 92.34.
Discussion
Different material and design of ureteral stents have been developed in the past. Mainly two different study groups have been working with the idea of a magnetic DJ removal. One Chinese group describes a spiral elastic wire at the bladder coil end of the stent and a retrieval catheter with a magnetic tip and several small hooks to snag the metal elastic spiral wire for blind removal. 12 The stent was tested in a bench model for removal and biocompatibility in a rat model. In vivo studies need to show how the material acts in patients and how they cope with the stent. Altarac and Vrazic describe a similar stent with a permanent magnet on the distal part. The retrieval device is a Nelaton catheter with a magnet at the tip. The two magnets should connect in the bladder to extract the stent. However, removal was not always effective because of lack of mobility of the catheter and decoupling of the magnets. Only female patients were described so far and no randomized controlled study was described to date. 13 Other nonendoscopic techniques for DJ removal include the use of a string attached on the distal part of the DJ, hanging out of the urethra. By pulling the string the DJ can be removed without any further transurethral manipulation. This method is a convenient way for DJ removal when the DJ persists for few days, but if the DJ is needed to stay longer, the risk of a urinary infection increases and patients do not cope with the string by complaining of urinary leakage.
Different studies show the advantage regarding patient comfort of DJ removal by leaving the string on the stent for approximately 1 week compared with a cystoscopy. But no differences occurred regarding stent-related quality of life or urinary symptoms using the USSQ score. 14,15 One study showed a significant difference referring to pain during stent removal 14 compared with the removal with a flexible cystoscope, whereas another study showed different findings. 15 One concern of leaving the string is accidently removing the stent before the prescribed time. This could be crucial if the patient has an infection, perforation, or a ureteral stricture. Althaus et al. found in a three-center study with 512 cases that 5.3% of men and 24.4% of women accidently dislodged the string. According to their study, 15% of all patients with strings will have inadvertent stent dislodgement, whereas women have a fourfold higher risk. 16 Otherwise most people with the string did not have sexual intercourse, which might affect quality of life. A total of 16.67% of patients with the indwelling magnetic DJ did not have sex because of the DJ, whereas 35.29% with the standard DJ stopped having sex because of discomfort caused by the DJ. The number of patients seems to be quite low, but there is still an effect on sexual activity caused by the implantation of a DJ, either magnetic or standard.
Other new innovations such as biodegradable stents might yield to no DJ removal at all. 17,18 Barros and colleagues describe a stent made of polysaccharides, which degrade within 2 weeks in artificial urine in an in vitro study. 18 Another study showed stents that were covered with ketoprofen to treat renal colic. Fifty percent of drug release could be seen in the first 10 hours, the other 50% released within 60 hours. In vivo clinical trials are not performed to date with any biodegradable stent, but this might be a promising future development. 19
In our study, almost half of the patients with the magnetic DJ (48%) experienced pain in the lower abdomen or around the bladder, whereas most patients in the standard DJ group (54%) described pain around the flank. This difference could be related to the small magnet, which might cause discomfort in the bladder and abdomen. Just 18% of the patients with the magnetic DJ complained about flank pain.
A limitation of the magnetic DJ is the fact that magnetic resonance tomography is contraindicated with the indwelling stent, because the small magnet might heat up and can damage the bladder wall.
We could show in our study that the DJ removal was easy and less painful. If a magnetic DJ removal was not effective, a cystoscopy can be easily performed. One ineffective DJ removal was caused by a big prostatic middle lobe.
Further studies might be useful to show whether there is a threshold to avoid the magnetic DJ in patients with enlarged prostates and a big middle lobe. Owing to our relatively young patient cohort, we cannot give a recommendation whether to use the magnetic DJ in men with large prostate.
One limitation of our study is the low number of patients. However, the study was performed in a prospective randomized manner to reduce selection bias.
By reducing operating room time, expendable materials, and presence of a urologist, as well as the working hours of nursing staff, a cost reduction could be obtained. There might be a difference regarding the reimbursement depending on the national medical insurance system.
Conclusion
The magnetic DJ can be removed fast with less unpleasant side effects compared with the standard cystoscopic removal. There is hardly no difference regarding the comfort with the indwelling stents. The magnetic DJ seems to improve patient's quality of life for DJ removal.
Footnotes
Author Disclosure Statement
Urotech (Achenmühle, Germany) has supported this trial by providing the ureteral stents cost free for all patients within this study. M.R. and M.C.R. have received funding for conference attendance. None of these sources had any input whatsoever into this article. The remaining authors have no competing financial interests.