
Abstract
Objective:
To compare conventional videocystoscopy (CVC) with a novel and affordable (approximately $45) mobile cystoscopy system, the Endockscope (ES). We evaluated the ES system using both fluid (Endockscope-Fluid [ES-F]) and air (Endockscope-Air [ES-A]) to fill the bladder in an effort to expand the global range of flexible cystoscopy.
Methods:
The ES system comprised a portable 1000 lumen LED self-contained cordless light source and a three-dimensional printed adaptor that connects a mobile phone to a flexible fiber-optic cystoscope. Patients undergoing in-office cystoscopic evaluation for either stent removal or bladder cancer surveillance received three examinations: conventional, ES-F, and ES-A cystoscopy. Videos of each examination were recorded and analyzed by expert endoscopists for image quality/resolution, brightness, color quality, sharpness, overall quality, and whether or not they were acceptable for diagnostic purposes.
Results:
Six of the 10 patients for whom the conventional videos were 100% acceptable for diagnostic purposes were included in our analysis. The conventional videos scored higher on every metric relative to both the ES-F and ES-A videos (p < 0.05). There was no difference between ES-F and ES-A videos on any metric. Fifty-two percent and 44% of the ES-F and ES-A videos, respectively, were considered acceptable for diagnostic purposes (p = 0.384).
Conclusions:
The ES mobile cystoscopy system may be a reasonable option in settings where electricity, sterile fluid irrigant, or access to CVC equipment is unavailable.
Introduction
C
Advances in technology, however, are costly, which is prohibitive in making cystoscopy readily available on a global scale. Indeed, if one takes into consideration the costs of the high-powered light source, camera system, and the endoscope itself, along with the disposables for each cystoscopic procedure, the average cost of each in-office diagnostic cystoscopy rises to $300. 2
In addition to the high equipment costs of cystoscopy, those in the underdeveloped countries face additional barriers as access to electricity or disposable sterile fluid irrigant may be limited. Air cystoscopy is an alternative to fluid irrigant and is a technique that has been used since the 19th century, but is not readily utilized by urologists today given concerns of air embolism. 3,4 Although there have been reports of air embolism in other facets of urology, there have been none reported secondary to cystoscopic evaluations. 3,4 Some authors reported air expansion to be superior to a fluid irrigant for visualization of the bladder to determine the source of hematuria. 5,6
In an effort to reduce the cost burden of videocystoscopy and thereby make it more available on a global basis, we developed the Endockscope (ES) 7 (Fig. 1), a novel and affordable (<$50) videocystoscopy system which utilizes a mobile phone for image display and a solar rechargeable LED self-contained cordless light source. In this study, we sought to clinically compare the fluid-based endoscopic view with conventional videocystoscopy (CVC) to the air- and fluid-derived images using the ES.

Full Endockscope setup, including fiber-optic cystoscope, LED light source, and mobile phone.
Methods
ES system design
Commercially available and custom three-dimensional (3D) printed components were assembled to relay the image viewed through a flexible cystoscope to an Apple iPhone 6S™ (Apple, Inc., Cupertino, CA) operating in camera mode. An off-the-shelf 8 × optical zoom lens system with an attached iPhone case was used to produce a combined effective focal length of 18 mm. SolidWorks software (Dassault Systemes SolidWorks Corporation, Waltham, MA) was used to create a computer-aided design file for a custom coupling mechanism to securely attach the lens system to the outer diameter of the eyepiece of an endoscope. This file was then used to 3D print the coupling mechanism with acrylonitrile-butadiene-styrene (ABS) plastic using a uPrint SE Plus 3D printer (Stratasys Ltd., Rehovot, Israel). This configuration provided a centered image on the iPhone camera with an 8 × optical zoom with respect to the stock iPhone camera lens system (Fig. 2). This eliminated the need to use digital zoom to fill the iPhone screen, providing for maximal image quality.

Mobile phone case, 8 × optical zoom system, and three-dimensional printed coupling mechanism for attachment to fiber-optic cystoscope eyepiece.
An LED self-contained cordless light source was made using off-the-shelf materials. SolidWorks software was used to create a computer-aided design file for a custom-made adapter to connect the light source to the light port of a cystoscope. An SE Plus 3D printer was used to 3D print the adapter in ABS plastic. This resulted in a lightweight, wireless LED light source with an integrated rechargeable power source that can be attached directly onto the light post of the cystoscope, eliminating the need both for a high-powered halogen light source and its associated fiber-optic light cable (Fig. 3). The light source is 1000 lumens. The cost of the entire kit, not including the mobile phone and cystoscope, was approximately $45 (Fig. 1).

1000 lumen solar rechargeable LED light source with custom adaptor.
Endoscopic procedure
Institutional review board approval was obtained before the initiation of the study. Patients receiving in-office flexible cystoscopy, as indicated, for either bladder tumor surveillance or stent removal, were considered eligible for this study. Following informed consent, each patient received three consecutive endoscopic evaluations by one of two urologists (J.L. or R.V.C.). The Karl Storz (Karl Storz Endoskope, Tuttlingen, Germany) flexible fiber-optic cystoscope was first passed into the urethra at the outset of the procedure and was not removed until completion of the study. CVC was performed using sterile saline irrigant and a Karl Storz H3Z Image 1 HD camera (Karl Storz Endoskope), monitor, and light source (Karl Storz Xenon 300), as per the standard of care. While recording, the urologist performed a systematic bladder evaluation such that the right and left ureteral orifices, dome of the bladder, trigone, and bladder neck were seen. Next, the Karl Storz HD camera and light cable were detached and replaced by the ES system and the same systematic cystoscopy was performed using the video recording feature on the iPhone 6S and a sterile saline irrigant (Endockscope-Fluid [ES-F]). For the final evaluation, saline irrigant was drained and replaced with the same volume of air using a 60-mL sterile syringe (Endockscope-Air [ES-A]); cystoscopy was then repeated.
Video comparison
All three examinations were recorded and then sent to expert endourologists for a blinded evaluation on a variety of metrics: image quality/resolution, brightness, color quality, sharpness, and overall quality. Each video was graded on a Likert scale ranging from 1 (extremely poor) to 5 (excellent). In addition, each reviewer was asked whether the video was acceptable for diagnostic purposes (yes/no).
Results
Ten patients undergoing flexible videocystoscopy for bladder cancer surveillance or stent removal between December 2015 and March 2016 were included in the study. Among the 10 patients, 6 had CVC control videos that were deemed 100% acceptable for diagnostic purposes and were therefore included in our final analysis. Still images of each type of endoscopic evaluation, all taken from the same patient, are included in Figure 4. These 18 video segments (6 CVC, 6 ES-F, 6 ES-A) were sent for review to 11 expert endoscopists (see Acknowledgments section) (Table 1 and Fig. 5).

Video stills of the right ureteral orifice using conventional videocystoscopy (CVC), Endockscope-Fluid (ES-F), and Endockscope-Air (ES-A) cystoscopies. CVC video was captured using a Karl Storz Image 1 Hub (Karl Storz Endoskope, Tuttlingen, Germany) video box, and iPhone video was captured using an iPhone 6S.
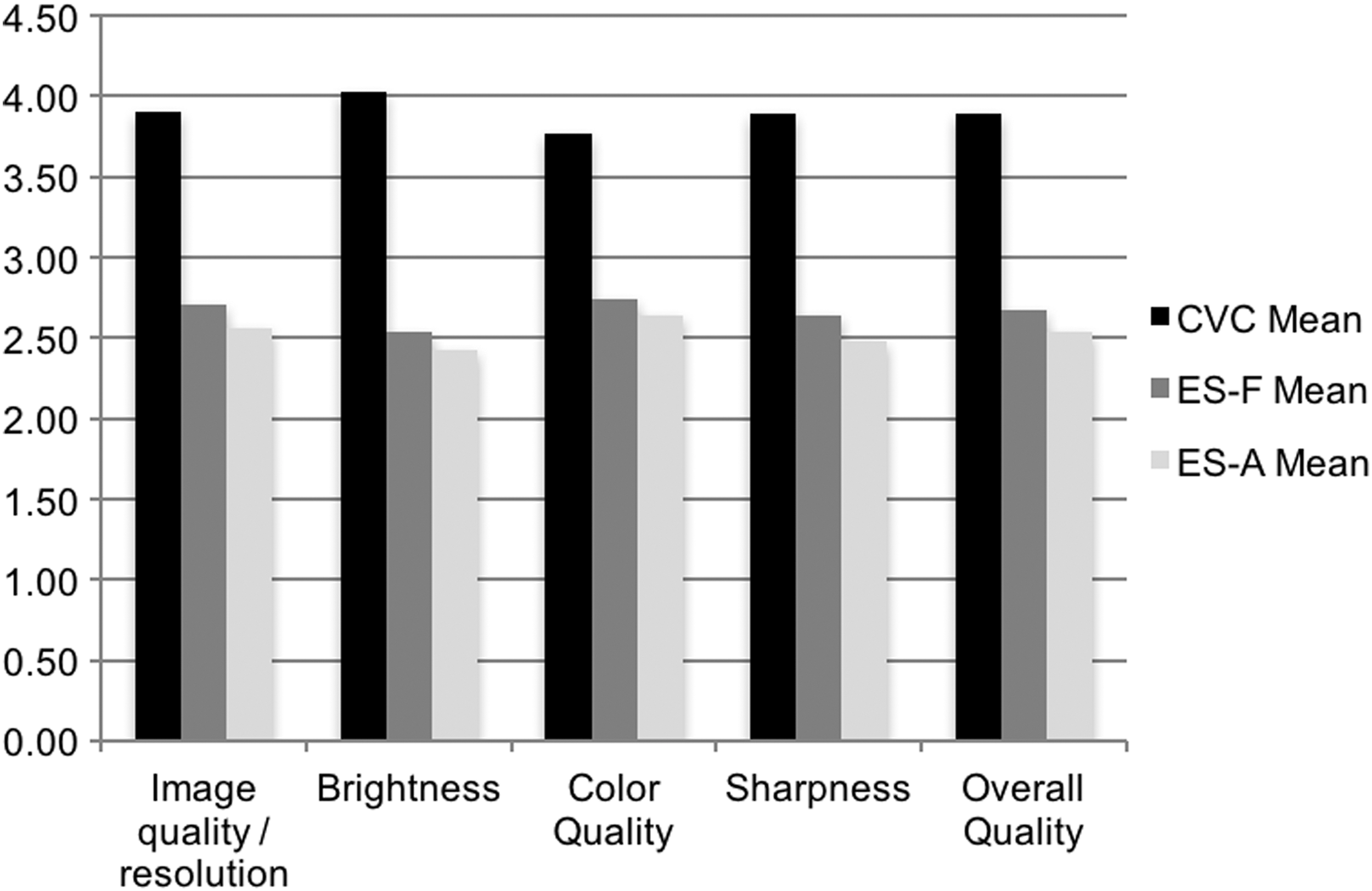
Video quality questionnaire results.
CVC = conventional videocystoscopy; ES-A = Endockscope-Air; ES-F = Endockscope-Fluid; SD = standard deviation.
The CVC videos scored higher than ES-F or ES-A videos on all of the metrics (p < 0.0001). The largest difference was in the brightness score, which was 4.03, 2.54, and 2.43 for the CVC, ES-F, and ES-A videos, respectively (p < 0.0001). In a subset analysis comparing ES-F with ES-A videos, ES-F videos scored higher on all of the metrics, although none of these differences reached statistical significance. Overall, 52% and 44% of ES-F and ES-A videos, respectively, were considered acceptable for diagnostic purposes.
Discussion
The ancestor to the modern endoscope dates to 1805 when Philip Bozzini, a German army surgeon, created the “Lichtleiter,” a speculum-like device that enabled him to peer into the female urethra and bladder using a beeswax candle light source and a series of small silver reflecting mirrors. 8 A century and a half later, the first flexible fiber-optic endoscope was used by Basil Hirschowitz, a gastroenterology fellow, to visualize the upper alimentary canal. 8 Tsuchida and Sagawara were the first to describe the use of a flexible fiber-optic cystoscope in 1973; a decade later, the first digital endoscope became available. 8
State of the art CVC requires several components: sterile fluid irrigant, a high-power external light source, a fiber-optic or digital cystoscope, and a video monitor/camera system. The cystoscope itself usually costs between $2000 and $4000 and is equally as expensive to repair. 1 The cost of the endoscopic tower system, including the tower, monitor, light box, camera box, and cables reaches approximately $45,000 depending on the manufacturer. 7 As such, Lotan and Roehrborn estimated the cost of a single in-office cystoscopic evaluation to be approximately $300, well out of reach of most low-income countries. 2
The first iteration of the ES in 2013 showed feasibility of the coupling mechanism, although without any clinical data. 7 This study, completed in 2016 after obtaining institutional review board approval for human application and improvement of the system with addition of a self-contained rechargeable light source, aimed to test the ES system's utility in a real clinical setting. Our results show that the video quality from the ES is inferior to CVC in the setting of an in-office cystoscopy for bladder cancer surveillance or ureteral stent removal. We did not expect the ES to be equal in its clinical utility to CVC; however, we do believe that the ES has immense clinical potential because of its reduced cost, portability, video recording ability, compatibility with widely available mobile phone technology, and wireless connectivity. Additionally, almost half of the expert reviewers deemed that the video quality was acceptable for diagnostic purposes.
The ES was primarily developed as a mechanism to bring flexible cystoscopy to environments and locations where it is currently not viable from a cost perspective. As such, our comparison to CVC was primarily an effort to establish the relative efficacy of the ES technology. Indeed, the evaluation of air cystoscopy in the current article was another mechanism by which we had hoped to minimize the cost and resources of cystoscopy, thus making the procedure viable where it is currently unavailable. Additionally, the portability of the ES makes it of great value to these same regions where it may not be feasible to keep a CVC tower in one location or in places where electricity is not available.
Digital flexible cystoscopy is today's preferred method of CVC in the developed world; as such, there are a large number of flexible fiber-optic cystoscopes that are not being utilized or have been traded in. We believe that gathering these cystoscopes and pairing them with the inexpensive (<$50.00) complete ES kit (i.e., LED solar chargeable flashlight and 3D printed mobile phone attachments) may be extremely useful for low-income or remote areas where mobile phone technology has penetrated. While specific sales data in third world countries are not publicly disclosed, according to the Pew Research Center, smartphone ownership rates in emerging and developing nations are rising, climbing from a median of 21% in 2013 to 37% in 2015. 9 In 2015 alone, there were a total of 1.4 billion smartphones sold worldwide. 9 Access to smartphones is emerging in third world countries and by giving healthcare providers the ability to pair their devices with the ES, there lies a potential to dramatically improve detection rates of bladder pathology. Images can be easily uploaded for viewing at a remote site either at the time of the cystoscopy or stored and forwarded at a later date. We believe that this same technology can be applied to all fiber-optic endoscopy whether it be of the urinary tract or other organ system.
A distinct advantage of pairing mobile phone technology with cystoscopy is wireless Internet connectivity. A trained urologist is required to interpret the findings of a cystoscopic evaluation; often times the difference between a healthy and unhealthy bladder is subtle and requires years of experience to recognize. However, it is far simpler to train an individual to meticulously perform a thorough cystoscopic evaluation of the bladder and urethra than it is to train a urologist. With the ability to record and share the video digitally, it is possible to have an individual trained in performing cystoscopy upload a video of the examination to the “cloud,” where it can be interpreted by an expert, although remote, urologist. Indeed, future iterations could rely on artificial intelligence algorithms to assist in diagnosis.
Although our study is limited by a small sample size, we believe there is immense global clinical potential with the ES system. In places where there are few or no urologists and scant, if any, cystoscopy resources, whether they be CVC video towers or sterile fluid irrigant, the ES system may be utilized as long as a fiber-optic eyepiece enabled cystoscope and an iPhone are available. We found no difference in video quality between ES-F and ES-A evaluations; although there was a small sample size, we do believe that air cystoscopy is a reasonable alternative to cystoscopy with fluid irrigant if sterile fluid is unavailable. Some studies have suggested that an air medium may even be superior to fluid, especially in diagnosing the etiology of macroscopic hematuria. 5
Only about half of the ES videos were considered adequate for diagnostic purposes; however, this is only the first iteration and we believe that the ES system can be greatly improved. For example, the brightness, which was the biggest disadvantage according to reviewers, can be improved by using a more powerful LED light source (>1000 lm). In addition, the new iPhone has nearly 4 million more pixels than the iPhone 6 and the recent PIXEL from Google provides even more resolution and better color definition. While the ES presently cannot compete with the digital cystoscope or the typical fiber-optic arrangement with its sophisticated camera technology and high-powered light source, it is a first step in bringing flexible endoscopy to many places where cystoscopy either does not exist or is obtainable only in a rigid, and more morbid, format. To that end, at the 2016 World Congress of Endourology, 26 Units were distributed at no cost to urologists working in remote areas of the world. Their experience will test the worth of this approach in flexible endoscopy.
Conclusions
The ES mobile cystoscopy system brings flexible cystoscopic capability to areas where electricity, sterile fluid irrigant, or access to CVC equipment is unavailable. In its current iteration, it was found to provide images sufficient for diagnostic purposes in half of the cases in which it was used.
Footnotes
Acknowledgments
We are indebted to our expert reviewers who kindly provided their expertise and time to this study: Richard Babayan (Boston University, Boston, MA), James Borin (New York University, New York City, NY), Jeffrey Caddedu (University of Texas Southwestern Medical School, Dallas, TX), Judy Choi (University of California–Irvine, Orange, CA), Brian Eisner (Harvard Medical School, Boston, MA), Manoj Monga (Cleveland Clinic, Cleveland, OH), Margaret Pearle (University of Texas Southwestern Medical School, Dallas, TX), Stephen Nakada (University of Wisconsin, Madison, WI), Chandru Sundaram (Indiana University, Indianapolis, IN), Roger Sur (University of California–San Diego, San Diego, CA), and Stuart Wolf (University of Texas–Austin, Austin, TX).
Author Disclosure Statement
No competing financial interests exist.