
Abstract
Introduction:
Several studies have examined the link between temperature or monthly seasonal variations and urolithiasis. The majority of these studies have demonstrated a link between higher ambient monthly temperatures and the incidence of renal colic and kidney stone disease (KSD). However, a worldwide trend on this association has not been explored and we perform a systematic review to examine the effect of seasonal variations on renal colic and KSD.
Materials and Methods:
A systematic review of the literature for a 26-year period (1990–2017) was conducted on all studies reporting on the effect of seasonal variations and its link to KSD. Two reviewers independently extracted the data from each study, which were analyzed using SPSS version 24.
Results:
A total of 59 studies were identified, and after screening, 13 were included in this review. The studies ranged in duration from 1 to 9 years (mean: 5.5 years) and included seasonal/monthly variations for proven stones or lithotripsy treatments or emergency department presentations with renal colic. Except for one study, there was a statistically significant association between higher monthly mean temperatures and the incidence of KSD-related events reported from the United Kingdom, South Korea, the United States, Saudi Arabia, Italy, Spain, Taiwan, Japan, and New Zealand.
Conclusions:
Worldwide trends on the incidence of renal colic and KSD seem be affected by seasonal variation favoring warmer months, with data suggesting that higher ambient temperature has an association with KSD.
Introduction
T
Although regional trends have shown a link between higher ambient monthly temperatures and the incidence of renal colic and KSD, a worldwide trend on this association has not been explored. We perform a systematic review to examine the effect of seasonal variations on renal colic and KSD.
Materials and Methods
Evidence acquisition: criteria for considering studies for review
Inclusion criteria: 1. Studies reporting on urolithiasis or renal colic or stone treatment, with recorded seasonal/monthly mean temperature. 2. Studies reporting in English language with no age restrictions.
Exclusion criteria: 1. Studies examining seasonal variation for nonurolithiasis conditions. 2. Studies with incomplete data or where a more updated study was available.
Search strategy and study selection
The systematic review was performed according to the Cochrane Review guidelines. The search strategy was conducted to find relevant studies from Ovid Medline without revisions (1990–January 2017), Cochrane Library (2017), CINAHL (1990–January 2017),
Terms used included “weather,” “temperature,” “seasonal,” “variation,” “trend,” “kidney,” “calculi,” “stones,” “renal,” and “urolithiasis.” Boolean operators (AND, OR) were used to refine the search.
The search was limited to English language articles between 1990 and January 2017. Authors of the included studies were contacted in the case of data not being available or if it was unclear. If the authors did not reply, data were estimated from the graphs provided in the study; and if the data could not be estimated, then the study was excluded from analysis.
Two reviewers (R.M.G. and B.K.S.) identified all studies, and those that appeared to fit the inclusion criteria were included for a full review. Each reviewer independently selected studies for inclusion in the review (Fig. 1).
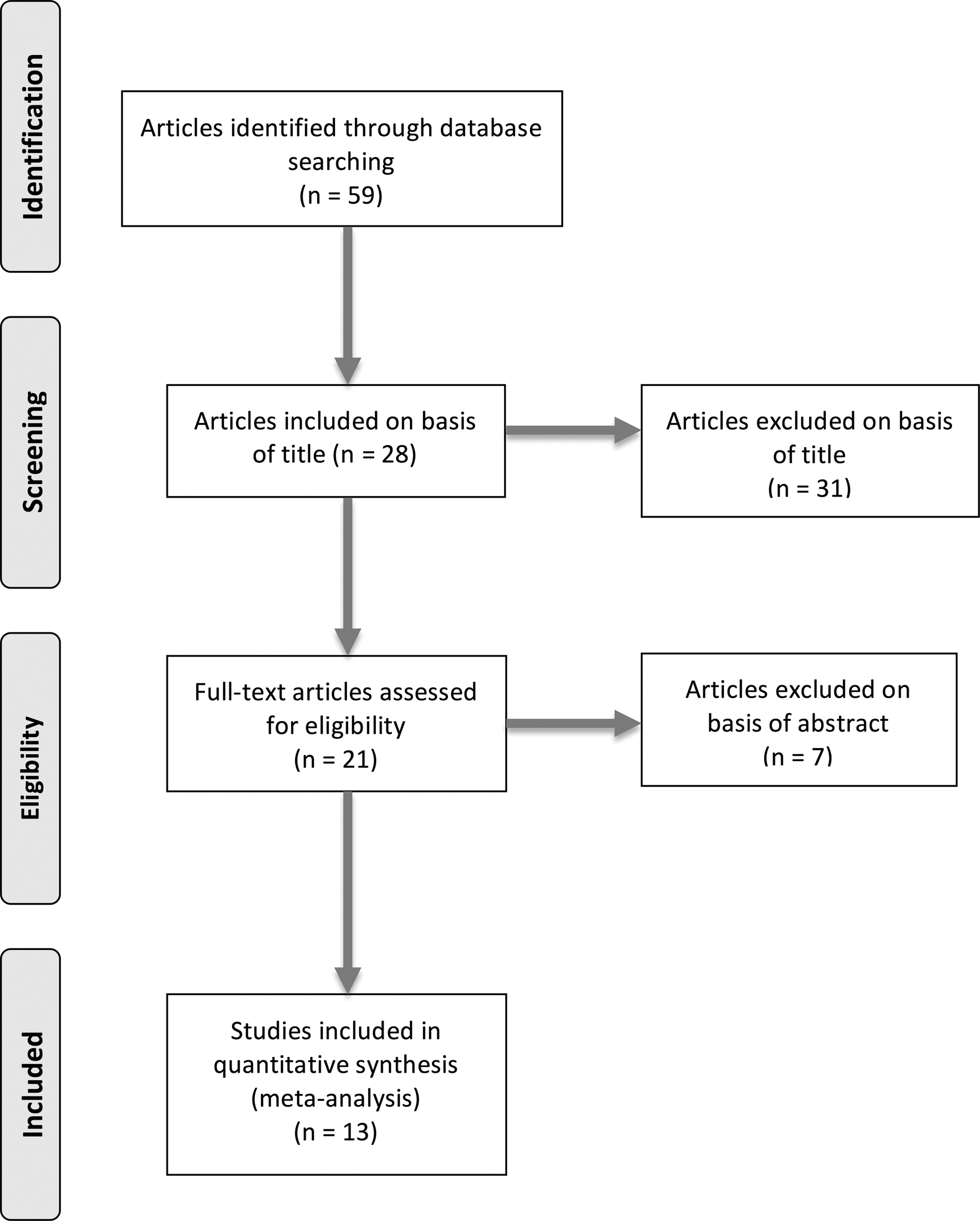
Preferred reporting items for systematic reviews and meta-analyses flow diagram for article selection.
Data extraction and analysis
The following variables were extracted from each study: year of publication, country of study, type of data set/database, mean monthly temperature, study period, and parameters observed as proxy for stone formation/presentation rate. Level of evidence was assessed using the recommendations set out by the Centre for Evidence-Based Medicine. 20 Data were collated using Microsoft Excel (version 12.2.4) and analyzed using SPSS (version 24). Associations between temperature and urolithiasis presentation were analyzed using linear regression.
Results
Overall, there were 13 studies identified, 4 –16 from a search yielding 59 articles with suitable titles (Fig. 1). The studies took place in the United Kingdom, 4 South Korea, 5,15 the United States, 6 Saudi Arabia, 7 Spain, 8,14 Italy, 9,11 Taiwan, 10,16 Japan, 12 and New Zealand. 13 Mean temperatures for January, April, July, and October were 7.3°C (range: −2.7 to 22.6), 15.4°C (range: 10.0 to 27.5), 25.6°C (range: 11.5 to 34.0), and 17.4°C, respectively (range: 12.0 to 29.8) (Table 1). Except for the study from New Zealand, 13 the mean temperature was higher in July for all reported studies, which correlated with an increased risk of renal colic and proven stones in 12 of the 13 studies. Of the 13 studies, 3 demonstrated data for proven stones 4 –6 and 9 used emergency department (ED) presentation for renal colic as a proxy for rate of stone formation. 7 –15 One study used number of extracorporeal shock wave lithotripsies performed per month as the proxy for rate of stone formation 16 (Table 2). Data were collated from studies reporting on national databases (n = 2), regional data (n = 1), multiple hospital data (n = 1), and solo hospital data (n = 9).
Higher seasonal temperature is shown in bold font.
SWL = extracorporeal shock wave lithotripsy.
ED = emergency department; SWL = extracorporeal shock wave lithotripsy.
Trend analysis
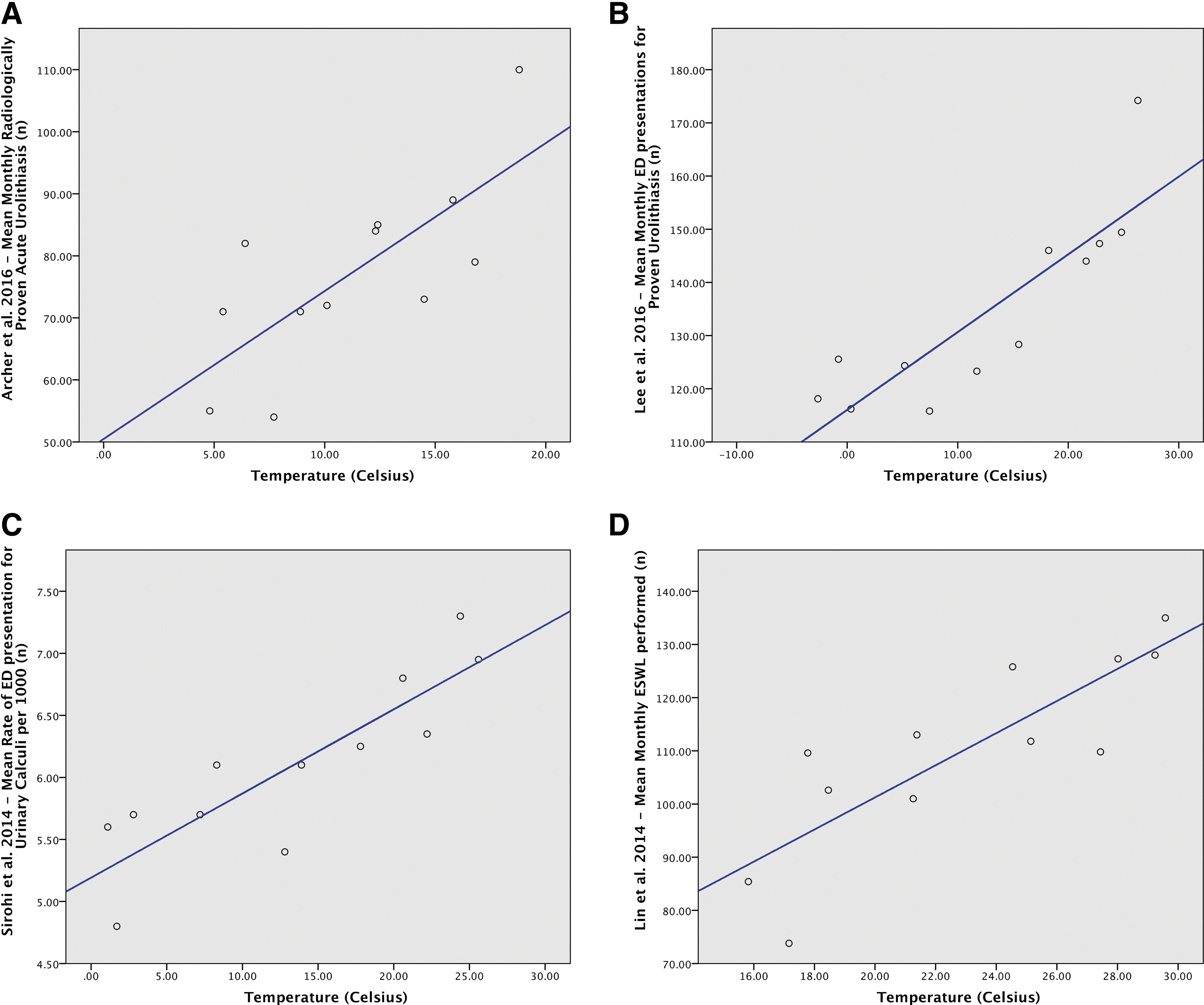
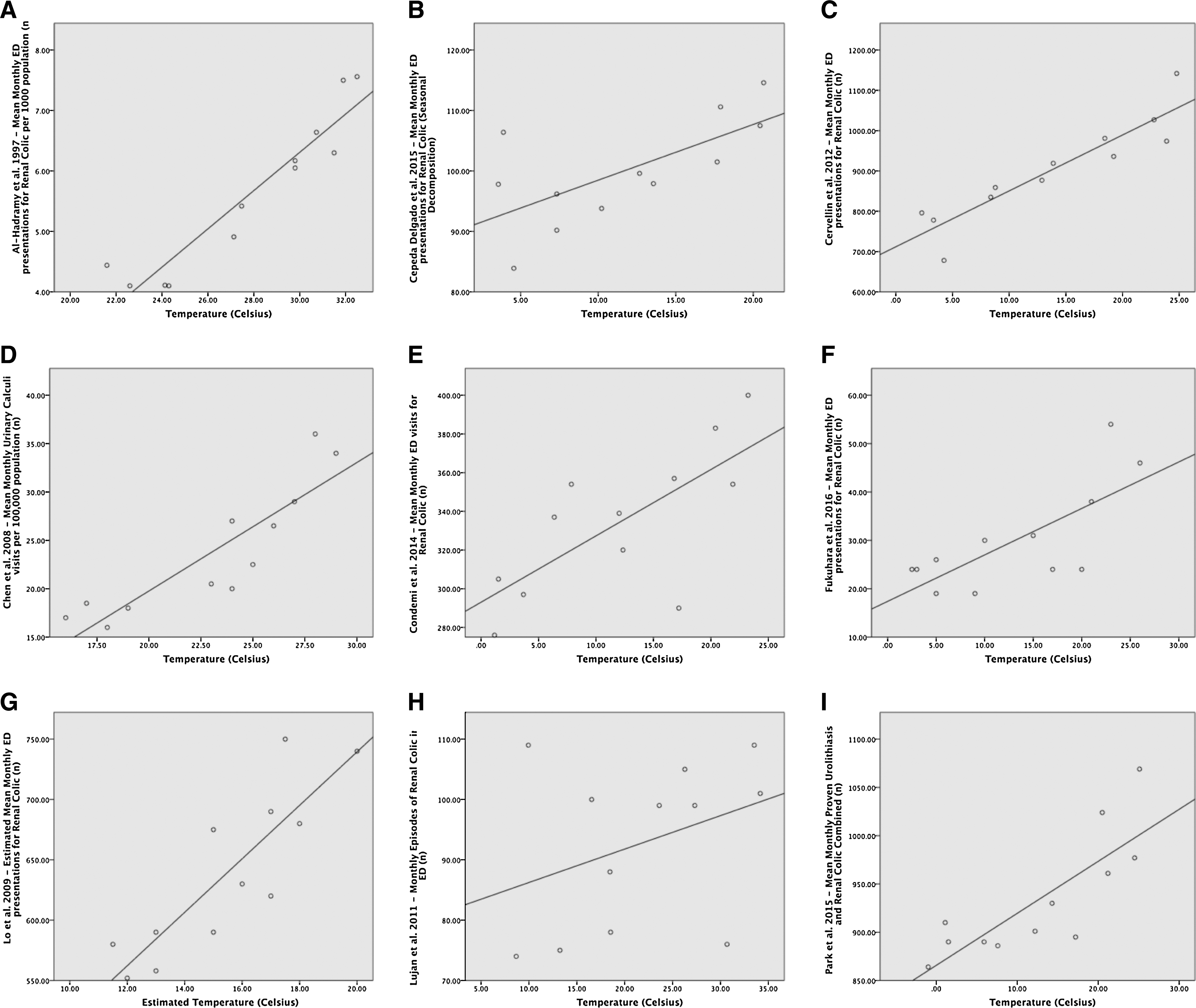
A total of 2,033,157 patients were reported in the study period (mean: 5.5 years, range: 1–9 years) and a male:female ratio of 3:1. Trend analysis using linear regression analysis was performed on individual studies; however, no overall analysis was performed given the heterogeneity of the data. Except one study, there was a statistically significant association between higher monthly mean temperatures and the incidence of KSD-related events reported from the United Kingdom, South Korea, the United States, Saudi Arabia, Italy, Spain, Taiwan, Japan, and New Zealand (Table 3; Figs. 2 and 3).
Bold text indicates significant linear association.
ND = not documented.
Discussion
Main findings
This is the first systematic review to demonstrate the association between higher ambient temperature and urolithiasis. Twelve of the 13 studies demonstrated statistically significant associations between temperature and the study proxy for rate of stone formation, with trends of renal colic and KSD favoring higher mean monthly temperature 4 –13,15,16 The study by Luján and colleagues failed to demonstrate a significant association, possibly because of the short study period and a small number of patients, which is reflected in the low R2 value. 14
Although studies in most countries had higher mean temperature in July with trends favoring a higher incidence of KSD-related events during summer, the study from New Zealand showed a higher temperature from January to April (warmest months there) with a proportionate rise in trends of KSD events during these months. 13
Meaning of the study in relation to other published studies
The association of increased monthly temperature with worldwide trends of urolithiasis is clearly shown from this study. This has important implications for healthcare planning, primary care prevention strategies, and allocation of available resources. 17 The mechanisms proposed for this association include increased sunlight exposure, relative humidity, inadequate fluid intake, and increased sweating, leading to dehydration and concentrated urine. 6,13,21,22
The exact mechanism for the effect of increased temperature on stone formation has not been demonstrated. Eisner et al. 21 demonstrated that urinary calcium excretion increased with increase in temperature, independent of humidity. Tasian and colleagues 18 demonstrated that the time lag between a rise in temperature and a rise in patient's presenting to ED was ≤3 days, suggesting that stone formation is relatively fast. However, to truly assess this link, the hydration status of the patients would have to be known throughout the study period, which in not feasible. Similarly, there seems to be a link between serum vitamin D and urinary markers of bone turnover, which seems to be higher during the summer months. 6,13,23
Strengths and weakness of our study
Our systematic review is based on worldwide data on all regional or national trends on association of KSD with climatic variations. This includes data from Europe, Asia, Middle East, New Zealand, and America, representing a sample population and weather map from most continents and geographical regions. The data detail not only renal colic patients but also treatment variations and proven kidney/ureteral stones, which shows a significant association with warmer climate consistently across multiple studies. To quantify this risk factor, we can use the R2 values, which range from 0.24 to 0.78 for statistically significant analyses. This demonstrates that temperature increase accounts for between 24% and 84% of increase in stone presentation.
The major limitation of this study is the heterogeneity of the data collected, whereby 9 of the 13 studies use renal colic as a surrogate for urolithiasis. However, a previous systematic review on the use of noncontrast CT scan for renal colic has shown a stone pick-up rate of 36%–73% with additional pathologies in 12%–15%, suggesting that renal colic is an acceptable surrogate for identifying patients with KSD. 24
Different hospitals may say serve variable population numbers and the reported incidence of KSD may also differ based on dietary factors, fluid intake, and provision and accessibility to healthcare. Similarly, hydration status of patients was not monitored or reported although there is an inference of higher ambient temperature, leading to dehydration. Similarly, different geographical areas might have influx of tourists during summer months, which has not been reported or accounted for in these studies, although this does not seem to be a case in most studies. Although we have not studied the impact of global warming, it has been proposed that global warming will lead to an increase of 1.6–2.2 million lifetime cases of urolithiasis by 2050 in the United States, which might be as high as 30% in some climate divisions. 17
Future studies
There is no standardized imaging and reporting of renal colic and KSD worldwide, and most data are obtained from small regional registries or local hospital databases. Similarly, stone composition that can give more insight into stone disease is not universally analyzed or reported in these studies. An important aspect to consider would be the effect of artificial environment such as air-conditioned buildings negating the effect of a heat wave, and studies also ought to assess this, in addition to the environment itself.
The real benefit would come from long-term studies, which looks into the effect of primary care intervention and public education on the preventive aspects of stone formation. The role of increased fluid intake, regulated protein consumption, and healthier lifestyle might need to be explored further. 6,21 Similarly, cost implication and budgeting allocation for kidney stone services may have to be based on the seasonal variation of stone disease, which might be different in different parts of the world.
Conclusions
Worldwide trends of renal colic and KSD seem to be affected by seasonal variation favoring warmer months, with data suggesting that higher ambient temperature has an association with KSD. This might have an impact on resource allocation for management of these patients during the warmer months.
Footnotes
Author Disclosure Statement
No competing financial interests exist.