
Abstract
Introduction:
Irreversible electroporation (IRE) is a non-thermal minimally invasive technique that is used to treat small renal masses (SRMs). Prior work has demonstrated greater narcotic requirements after radiofrequency ablation (RFA) for tumors that are closer to body-wall musculature. We hypothesized that pain after IRE is not dependent on tumor location due to the athermal mechanistic action.
Materials and Methods:
A retrospective review of 50 consecutive percutaneous IRE and RFA cases was performed from 2013 to 2014. Eight patients were excluded from analysis due to incomplete anesthesia record and/or multiple ablations per session, leaving 21 patients in each group. Data collected included patient age, sex, body mass index, nephrometry score, shortest distance to the closest body-wall muscle, perioperative narcotic use, and patient-reported pain score. Pearson correlation test and multivariable linear regression were used to identify predictors of postoperative pain, with significance set at p = 0.05.
Results:
There was no difference in the mean distance from tumor edge to the nearest body-wall muscle between IRE and RFA (2.6 cm vs 2.4 cm, p = 0.729, respectively). Total mean perioperative narcotic usage was 20.4 mg after IRE and 26.7 mg after RFA (p = 0.096). Mean postoperative pain score (scale 0–10) was slightly higher after RFA (4.3) compared with IRE (2.4), but this was not statistically significant (p = 0.088). Pearson correlation test identified tumor proximity to be significiantly associated with both pain score (p = 0.011) and postoperative narcotic use (p = 0.049) after RFA but not after IRE. On multivariable analysis, only tumor proximity to the body wall was significantly correlated to pain score (−1.4, p = 0.041) after RFA but was not found to be a factor for pain after IRE.
Conclusions:
Patients whose tumors lie close to their body-wall musculature do not have greater narcotic requirements or higher pain scores in the perioperative period after IRE. Percutaneous IRE may be preferred over RFA for SRMs that are close to the body wall to minimize pain.
Introduction
P
Transient lumbar plexus pain is a known morbidity of RFA for renal tumors. It is postulated to be caused by thermal injury to back musculature. A prior report demonstrated greater narcotic requirements after RFA if the kidney tumor was closer to the body-wall musculature. 7 The only prior study comparing clinical pain post-IRE vs RFA was on liver ablation and found no difference in pain scores or cumulative narcotic usage. 8 To our knowledge, whether or not proximity to the body wall causes more pain after IRE has not been previously reported. With its athermal mechanistic action, we hypothesized that pain is not dependent on tumor location after percutaneous IRE of SRM.
Materials and Methods
After Institutional Review Board approval, a retrospective review of 23 consecutive patients who had percutaneous IRE for SRM from 2013 to 2014 and 27 consecutive patients who had RFA in the same period was performed. Patients were offered both ablative modalities at their initial consultation and chose their preference for treatment based on risks/benefits discussed. Demographic data (patient age, gender, race, and body mass index [BMI]) and tumor characteristics (size, pathology, and nephrometry score) were recorded. The shortest distance of the tumor to the body-wall musculature was measured by two urologists independently after analyzing relevant cross-sectional axial imaging (Fig. 1). In most cases, this was the trajectory chosen for placement of the probes.
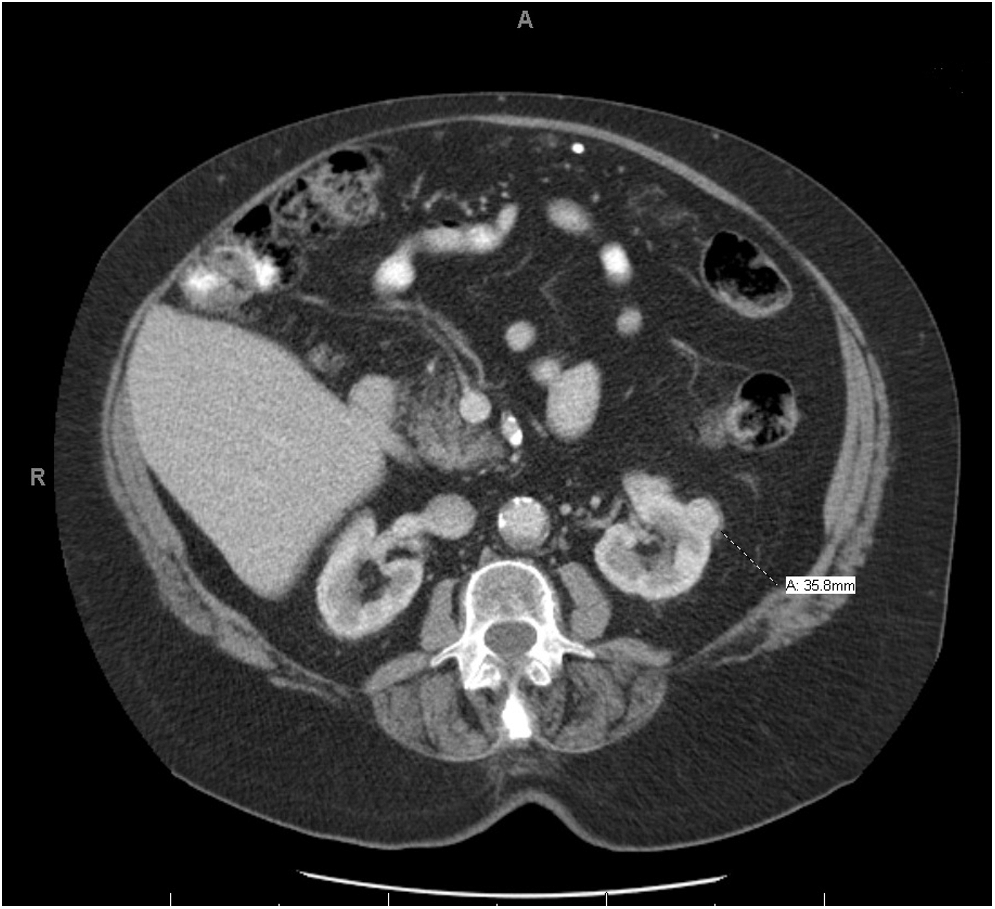
Measurement of distance between tumor and nearest body-wall musculature.
Two patients from the IRE cohort and five patients from the RFA cohort were excluded from analysis due to incomplete anesthesia record and/or multiple ablations per session. This left 21 patients in each arm to be included and compared in our analysis. Total perioperative narcotic usage was collected from anesthesia records, and it was then converted to morphine equivalents by using an opioid equianalgesic reference standard (
Both our percutaneous IRE and RFA techniques for kidney tumors were previously described. 2,9 Briefly, the procedures are performed with the patient under general anesthesia and neuromuscular blockade. A computed tomography scan is performed with contrast to localize the tumor. For RFA, we use a 15G RITA StarBurst™ probe (RITA Medical Systems, Mountain View, CA) to achieve near-perpendicular insertion of the probe on the mass. For IRE, the number of electrodes and configuration of electrode placement is determined by tumor size. For tumors <1.5 cm in diameter, 3 electrodes are placed in a triangular pattern around the tumor. For tumors 1.5–2.5 cm in diameter, 4 electrodes are placed in a rhomboid fashion around the tumor. To achieve adequate ablation, 30-40A of current must pass through the tumor between electrodes. The current output is determined by inherent tissue resistance, distance between electrodes, and the target voltage, which is set at 2000 V/cm. 10,11 A track ablation (within perinephric fat only) is not performed with IRE.
Statistical analysis was performed by using IBM® SPSS®, version 22. Continuous variables were compared by using Student's t-test. Categorical variables were analyzed by using either Pearson's chi-square or Fisher's exact test, where appropriate. Pearson product-moment correlation test and multivariable linear regression were used to determine which patient or tumor characteristics correlated to pain. Two-tailed hypothesis tests were used in each case, and a p-value of ≤0.05 was considered statistically significant.
Results
Patient demographics, tumor characteristics, and pain outcomes are compared in Table 1. All ablations were performed on cT1a lesions. There was no difference in the mean distance from tumor edge to the nearest body-wall muscle between IRE and RFA (2.6 cm vs 2.4 cm, p = 0.729, respectively). There were more men undergoing RFA compared with IRE (86% vs 52%, p = 0.043) and less opioid-naïve patients undergoing RFA compared with IRE (19% vs 76%, p < 0.001). Total mean perioperative narcotic equivalents usage was 20.4 mg after IRE and 26.7 mg after RFA (p = 0.096). Mean postoperative reported pain score was slightly higher after RFA (4.3) compared with IRE (2.4), but this was not statistically significant (p = 0.088). There was a higher percentage of patients without any reports of pain after IRE vs RFA (66.7% vs 33.3%, p = 0.031, respectively). There were no readmissions to the hospital for pain-related complications. Five patients (23.8%) were admitted for pain management after IRE compared with three patients (14.3%) who required admission for pain after RFA, but this was not statistically significant (p = 0.697).
BMI = body mass index; CCI = Charlson Comorbidity Index; IRE = irreversible electroporation; RFA = radiofrequency ablation; SD = standard deviation.
Correlation between patient and tumor characteristics and pain outcomes after IRE is shown in Table 2. There was no correlation between tumor proximity to body wall and postoperative narcotic use (r = −0.288, p = 0.206) or tumor proximity to body wall and patient reported pain score (r = −0.192, p = 0.405). Similar findings were noted, with BMI and nephrometry score as the dependent variables. Increasing age was found to be significantly correlated with lower perioperative narcotic equivalent use (r = −0.684, p = 0.001) and lower pain scores (r = −0.537, p = 0.012). Tumor proximity to the body wall was significantly correlated to patient-reported pain score (r = −0.545, p = 0.011) and postoperative narcotic use (r = −0.434, p = 0.049) after RFA, as shown in Table 3. On multivariable analysis, only tumor proximity to the body wall was significantly correlated to pain score (−1.4, p = 0.041) after RFA but was not found to be a factor for pain after IRE (Table 4). There were no significant predictors of narcotic usage after both RFA and IRE on multivariable linear regression (Table 5).
SE = standard error.
Discussion
Minimally invasive ablative technologies employed to treat SRM include RFA and CA, both of which have achieved durable long-term oncologic outcomes. 12 –15 An advantage to utilizing ablative technologies to treat SRM is the low rate of complications. 16 However, both of these ablative technologies rely on temperature extremes to cause cell death. As such, these treatments have side effects that are unique to thermal injury. Urothelial injuries can occur if the collecting system is involved in the zone of ablation, which may result in urine leakage, hematuria, and strictures. 17,18 In CA of kidney tumors, ice ball cracking of the tumor during the procedure can cause clinically significant hemorrhage. 18 Nerve damage leading to pain, paresthesia, and numbness has been described in both RFA and CA. 18,19
IRE is a nonthermal ablative technology with Food and Drug Administration approval for surgical ablation of soft tissue. Prior work has demonstrated its safety, with good clinical success in the short term with predominant applications in liver and kidney tumors. 1,2,20 IRE delivers high-voltage and high-current electrical pulses of a microsecond duration, thereby creating nanoscale pores within cellular membranes and leading to cell death. 21 It has been tested in vivo in animal studies to cause permanent cell death, whereas supporting structures such as collagen, blood vessels, and nerves have been shown to be spared during ablation. 6,22,23 A sciatic nerve study in rats demonstrated intact endoneurium and perineurium after IRE, with axonal regeneration demonstrated at 7 weeks. 24 Neurovascular tissue around the dog's prostate was also spared after bilateral transperineal IRE ablation. 25
The only prior study comparing clinical pain post-IRE vs RFA was on liver ablation and found no difference in pain scores or cumulative narcotic usage. 8 In our retrospective review of percutaneous IRE vs RFA cases, we found no correlation between tumor proximity to body-wall musculature and postoperative narcotic usage or numerical pain score after IRE. This finding is in contrast to our experience with RFA showing an increase in perioperative narcotic usage 7 and an increase in pain score when the tumor is in close proximity to the body wall.
Stimulation of the nociceptive receptors within the body-wall and diaphragmatic musculature from RFA-related heat likely leads to the discomfort. As IRE is a nonthermal ablative modality, the nociceptive receptors within the body wall may not be triggered in a dose-dependent mechanism as with RFA. Track ablation is also not performed during IRE; whereas in RFA, a track ablation is often done to prevent tumor seeding. This maneuver involves extending the ablation only 1 cm beyond the tumor capsule and stopping short of the body-wall musculature. Although it is performed under direct vision, unrecognized ablation to the body wall damaging sensory nerves could potentially occur and may account for the pain discrepancy between RFA and IRE.
In our study, only increasing age was correlated significantly with postoperative narcotic usage and pain scores on univariable analysis after IRE. Prior work has demonstrated that age is the best predictor of postoperative morphine requirements. 26,27 Age-related pharmacokinetic and pharmacodynamic factors may explain the decrease in postoperative opioid requirements as patient age increases. 26 However, this relationship between IRE and pain scores is likely more complex than just age alone, as shown in our multivariable analysis. Unlike IRE, no correlation between age and pain score or between age and postoperative narcotic use after RFA was seen. This may be attributed to the fact that there was a substantially greater number of opioid-naïve patients (76%) in the IRE group vs 19% in the RFA group who were affected by narcotics differently.
To our knowledge, this is the first study examining postoperative pain after percutaneous IRE vs RFA for kidney tumors. There are several limitations to this study. This is a small retrospective study with a small sample size, and data are limited to the immediate postoperative time period with no information on narcotic usage at home. Additional information, including time to return to work and normal activities, would be useful to assess ease of convalescence from the procedure. Nevertheless, we did not find any correlation between tumor proximity to body-wall musculature and pain scores or postoperative narcotic usage after IRE. If IRE proves to be equally effective as current thermal ablation modalities in the long term, anticipatory postprocedure pain may be an important factor to consider in decision making for the treatment of SRM.
Conclusions
Patients whose renal tumors lay close to their body-wall musculature did not have greater narcotic requirements or higher pain scores in the perioperative period after percutaneous IRE. On the other hand, patients with tumors that were in close proximity to the body-wall musculature did have higher pain scores with an increase in postoperative narcotic requirements after RFA. With increased experience and longer-term outcomes, IRE may be preferred over RFA and perhaps other thermal technologies for small renal tumors that are close to the body wall to minimize postprocedure pain.
Footnotes
Acknowledgment
This abstract was previously presented at the 33rd World Congress of Endourology meeting in London, United Kingdom, in 2015.
Author Disclosure Statement
No competing financial interests exist.