
Abstract
Introduction and Objective:
Ten percent of patients undergoing prostatic urethral lift (PUL) require repeat surgical treatment within 3 years. We describe the feasibility and considerations of performing holmium laser enucleation of the prostate (HoLEP) as a salvage therapy after previous PUL.
Methods:
Men who had undergone HoLEP after PUL were retrospectively identified from three institutions with surgeons experienced in HoLEP. Subjects were characterized by age, time from PUL procedure (months) to HoLEP surgery, indication for retreatment, and pre-operative prostate volume by ultrasound. Outcomes of interest included enucleation time, morcellation time, morcellator type, weight of tissue resected, and Clavien complications. We also summarize findings related to the location of PUL device implants, and the effect of the implants on the enucleation and morcellation portions of the procedure.
Results:
From December 15, 2015 to October 31, 2016, seven men aged 51–78 years underwent HoLEP at a median of 8.6 months (range 3–18) after PUL. The median prostate volume by transrectal ultrasound was 80 cm3 (range 56–160 cm3). For the 7 patients, 6 out of the 22 device implants were found in aberrant locations. Auxiliary maneuvers were required in five cases. Morcellation devices tended to jam with each implant, requiring a pause for withdrawal of the morcellator and manual removal from the blade or requiring grasper retrieval of device components. There were no Clavien complications.
Conclusions:
HoLEP can be performed safely and effectively post-PUL; however, device implants may be found in areas other than the intended location, and morcellation of the adenoma tissue is complicated by metallic implants of the PUL device.
Introduction and Objective
B
The UroLift device (NeoTract, Inc., Pleasanton, CA) is the only FDA-approved device U.S. Food and Drug Administration the prostatic urethral lift (PUL) procedure. PUL entails deployment of permanent adjustable implants that retract the lateral lobes of the prostate and provide a patent anterior channel through the obstructing lateral lobes of the prostate. The implants are deployed transurethrally under direct visualization through a rigid cystoscope. The device implants consist of a nitinol tab that anchors the device anterolaterally outside the prostatic capsule, attached by a polyethylene terephthalate (PET) 0.4 mm monofilament self-adjusting suture to an inner stainless steel tab that compresses the lateral lobe of the prostate (Fig. 1). Two to six implants (typically four) are placed to create an open prostatic channel. PUL is for glands less than 100 cm3 and it is not recommended for treatment of an obstructing median lobe. PUL has gained popularity due to favorable patient outcomes, reduced complications compared with TURP, 4 and the reported lack of adverse effects on sexual function, namely antegrade ejaculation. 5 From a surgeon's perspective, PUL offers a short learning curve, can be performed in the office under local anesthetics, and can be performed on patients at a high risk for anesthesia.
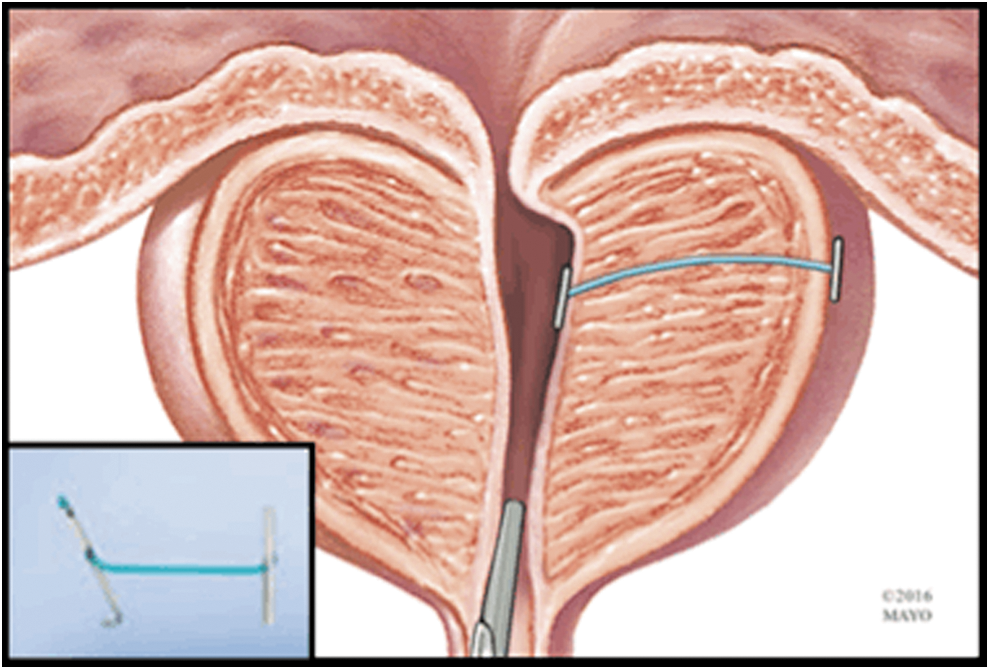
The UroLift PUL device consists of an 8 mm stainless steel urethral end-piece connected by PET monofilament to an 8 mm nitinol capsular tab that anchors the device outside the prostatic capsule. Proximal implants should be at least 1 cm distal to the bladder neck. 6 PET = polyethylene terephthalate; PUL = prostatic urethral lift.
PUL has been associated with retreatment rates of 1.5%–16% at 12 months, 5 7.5%–20% at 2 years, 6 –8 10% at 3 years, 9 and 14% at 4 years. Retreatment with TURP, photovaporization of the prostate (PVP), and repeat PUL have been documented without notable issue. 7 Holmium laser enucleation of the prostate (HoLEP) with morcellation of the resected adenoma is an established first-line therapy for BPH with an excellent durable response, and with particular benefit in patients with large glands. HoLEP has proved technically feasible and efficacious as a secondary procedure where previous BPH therapies have failed. 10 We describe the feasibility and considerations of performing HoLEP with intravesical morcellation of prostatic adenoma as a secondary procedure after previous PUL.
Materials and Methods
Men who had undergone HoLEP after PUL were retrospectively identified from three institutions: Mayo Clinic Arizona (MCA) (Phoenix, AZ), University of Arizona (Tuscon, AZ), and Baylor Scott and White Health (Temple, TX). Patients were evaluated by cystoscopy, uroflowmetry, transrectal ultrasound (TRUS) of the prostate, and urodynamics when indicated to define the etiology of their urinary symptoms and to determine appropriate therapy. Procedures were performed by a single surgeon from each institution, with considerable HoLEP experience. Subjects were characterized by age, time from PUL procedure to HoLEP surgery (months), indication for retreatment, and pre-operative prostate volume by ultrasound. Outcomes of interest included enucleation time, morcellation time, morcellator type, weight of tissue resected, 30-day Clavien complications, and surgical outcomes at 3 months follow-up. We also summarize findings related to the location of PUL device implants, and the effect of the implants on the enucleation and morcellation portions of the procedure. One patient at MCA underwent robotic exploration for removal of device implants, after HoLEP, as an attempt to alleviate pelvic pain, and this is detailed as well. Summary statistics were utilized when appropriate, namely median, mean, and range for continuous variables.
Surgical technique
Enucleation was performed as previously described, with slight variation by institution, utilizing a 100- or 120-W holmium:yttrium–aluminium–garnet (Ho:YAG) laser (Lumenis, Inc.) and a 550-μm end-fire laser fiber (SlimLine™ 550; Lumenis, Inc.) via a 26F continuous-flow resectoscope (Karl STORZ Endoscopy, Culver City, CA) with a 7F laser stabilizing catheter (Cook Urological, Inc., Spencer, IN).
Tissue morcellation was achieved under direct visualization by using either the reciprocating (VersaCut Lumenis, Inc., Santa Clara, CA) or oscillating morcellator (Piranha; Richard Wolf, Inc., Knittlingen, Germany) that was introduced through a 26F outer sheath and the offset nephroscope (Karl STORZ). Auxiliary procedures were defined as the need to use a grasper instrument or to perform additional work with the laser to remove pieces of the PUL device. A 22F three-way urethral catheter was placed for overnight continuous bladder irrigation as needed in all cases.
Results
From December 15, 2015 to October 31, 2016, seven men aged 51–78 years who had undergone HoLEP at the three institutions at a median of 8.6 months (range 3.2–18.8 months) after PUL were identified. In all cases, the PUL had been performed at an outside institution. Table 1 summarizes the preoperative evaluation for each patient. Persistent urinary symptoms were the operative indication in six out of seven cases, and chronic pelvic pain was the indication for the remaining patient. Five out of seven patients had urodynamic studies performed, with four demonstrating obstruction, and one being equivocal. All patients had a cystoscopy performed preoperatively and one patient was identified as having tri-lobar hypertrophy, which included an enlarged median lobe. The median prostate volume by TRUS was 80 cm3 (range 56–160 cm3).
HoLEP = holmium laser enucleation of the prostate; PUL = prostatic urethral lift; TRUS = transrectal ultrasound; UDS = urodynamic study.
Operative results are listed in Table 2. The median weight of resected tissue was 21 g (range 5–80 g). The median enucleation efficiency and morcellation efficiency were 0.9 (0.2–1.4 g/minutes) and 2.5 (0.7–4.7 g/minutes), respectively. The reciprocating morcellator was used in three cases, and the oscillating morcellator system was used in four cases. Auxiliary maneuvers were required in five out of seven cases, namely, utilization of a grasper instrument to remove device components. This was included in the morcellation time. There was one superficial bladder injury sustained during morcellation that required extended catheter drainage of 5 days, but there were no 30-day Clavien complications in any of the included cases. All patients were discharged on postoperative day 1. Three-month follow-up data were available for five out of the seven patients. The mean pre-operative International Prostate Symptom Score (IPSS) and bothersome scores were 21 (range 18–24) and 4.8 (range 4–6) compared with postoperative scores of 3.3 (range 2–4) and 1 (range 0–2), respectively. Median postvoid residual volume preoperatively was 300 mL (range 30–565 mL) compared with 45 mL (range 16–75 mL) postoperatively. Mean Qmax was 8.2 mL/second (range 5–12 mL/second) preoperatively compared with 15.8 mL/second (range 11–21 mL/second) postoperatively.
Operative findings
When separating the lateral attachments of each lobe from the prostatic capsule, we expected to transect the suture portions of each PUL implant. It should be recalled that this suture connects the inner stainless steel tab to the nitinol tab that is outside the prostatic capsule. We encountered implants between the 3 and 8 O'clock positions on the clock face rather than the manufacturer-recommended 10:30 to 1:30 location. When encountered, the suture was easily transected with the holmium laser. In several patients, we unexpectedly encountered one or more of the outer nitinol tabs in the plane between the adenoma and capsule, typically near the bladder neck (Fig. 2). This outer tab was expected to be outside the prostatic capsule. In one case, the tab was lodged partly in the capsule and was removed with the aid of a grasping instrument. The other tabs that were encountered were enucleated with a margin of tissue, avoiding direct application of energy to the tab itself to avoid fragmentation. The inner stainless steel tabs did not alter our enucleation technique. An inner stainless steel tab was visible on initial cystoscopy in only one out of the seven cases.
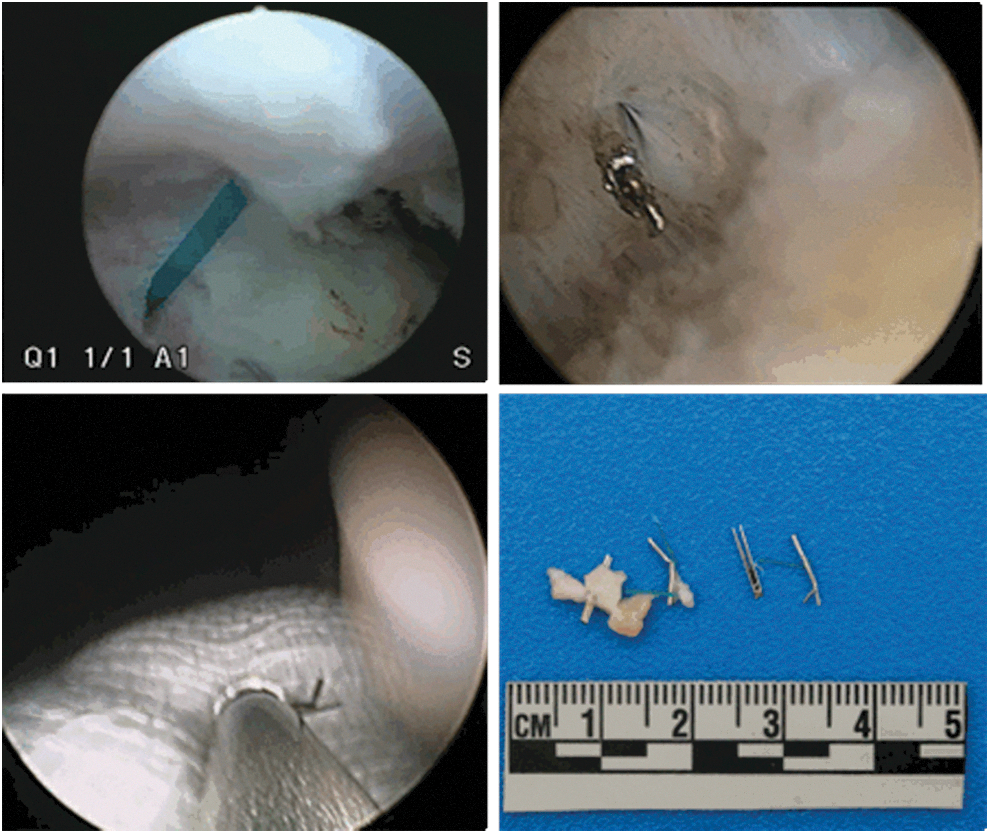
Clockwise from top left: PET suture before laser transection, capsular tab embedded in prostatic capsule, stainless steel urethral end-pieces removed during morcellation, and end-piece jamming the reciprocating morcellator.
Both morcellators became jammed when suture fragments or the stainless steel portions of the device were encountered. This resulted in temporary cessation of morcellation so that the instrument could be withdrawn and the foreign body manually removed from the blade. Removal of device components from the blades proved quick and easy in all cases, allowing morcellation to resume within a matter of seconds. We did note that with the oscillating morcellator, the stainless steel tabs were less likely to be entrapped in the blade, and they tended to bounce off. This allowed morcellation of the adenoma to continue without interruption, but it resulted in several minutes of chasing suture fragments and the steel tabs for removal by grasper after conclusion of morcellation. The difficulty of locating device components was dependent on the degree of hematuria present and also the severity of bladder trabeculations.
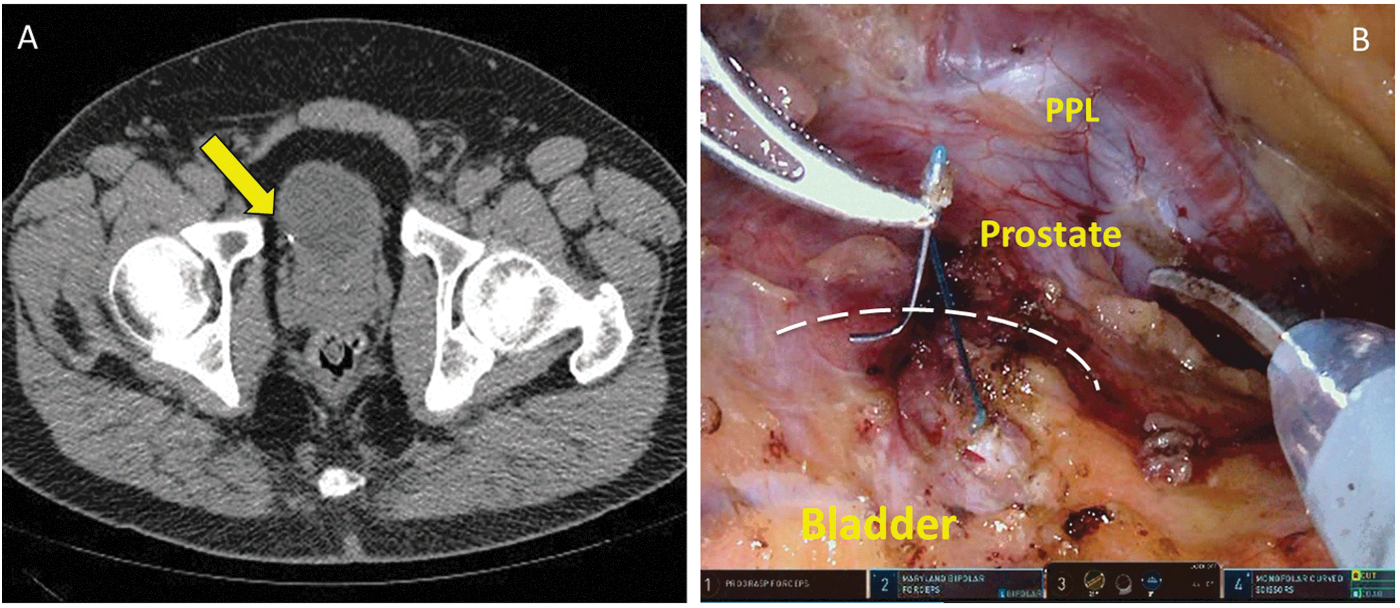
Severe pelvic pain was the operative indication for one patient (MCA4). This individual had significant pain after his PUL procedure at an outside hospital. Figure 3 illustrates the location of his device implants on CT after this procedure. A second urologist identified that the device components were improperly placed into the bladder neck and through the bladder wall, and performed a TURP for removal of the device components. One of the device components on the patient's right side was never encountered, but a CT scan revealed the presence of a tab outside the bladder near the junction of the prostate and bladder (Fig. 4A). He presented to us for persistent, debilitating pain, after conservative measures had failed. We first performed HoLEP of the residual tissue on the right side of his prostate and did not encounter any remnants of the device. As the patient was convinced that his pelvic pain was secondary to the foreign body, we agreed to perform a robotic exploration for removal of the device remnant. At MCA, we had experience performing robotic prostatectomy in two patients with previous PUL. In both cases, the outer nitinol tabs were visualized outside the prostatic capsule during the surgery and the surgery was not complicated by the PUL implants. In this particular case, the outer nitinol tab was encountered outside the bladder wall rather than outside the prostatic capsule (Fig. 4B). Excision resulted in a small cystotomy that required catheter drainage of his bladder for 7 days. At 2 months, the patient felt that his pain had improved significantly.
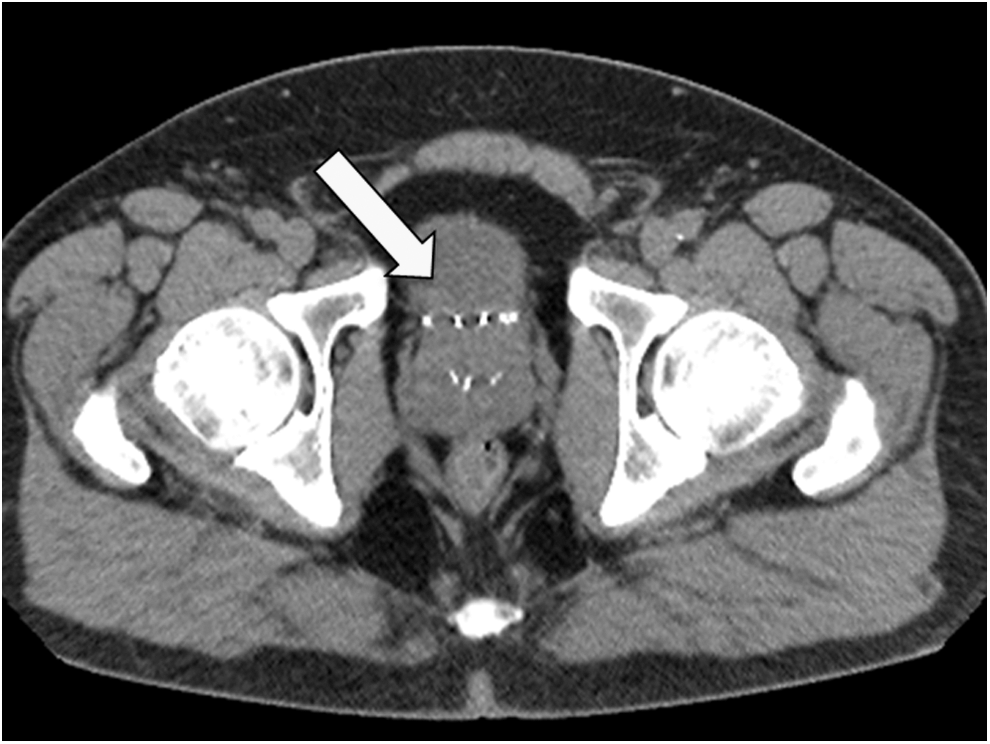
CT scan of pelvis demonstrating four PUL device implants located aberrantly at the bladder neck.
Discussion
The purpose of this article is to highlight the findings of three experienced HoLEP surgeons in performing HoLEP as a secondary procedure to PUL. PUL is conservatively associated with a 10% reoperative rate at 3 years. 9 With the increasing popularity of the PUL procedure, urologists should be prepared to perform secondary procedures after PUL failure. Whether the secondary procedure is TURP, PVP, HoLEP, or other procedures, understanding the PUL device design, intended function, and familiarity with the possibility of aberrantly placed PUL device implants is critical. In the present series, we found that HoLEP can safely be performed as a secondary procedure to PUL. Morcellation for retrieval of the adenoma is complicated by the device components, and auxiliary maneuvers are commonly required to remove all device components. These findings are likely transferrable to other treatment modalities, namely TURP and PVP as secondary procedures. Reports of TURP and PVP after PUL indicate that both energy modalities easily transect the PET suture, but retrieval of the metallic components is not specifically discussed. 7,11,12
The UroLift PUL device is not designed to treat median lobe enlargement or glands greater than 100 g. 12 In the current series, one patient had a gland that was 160 g on TRUS, and one patient had an enlarged median lobe. These patients were arguably poorly selected for PUL as an initial treatment. The UroLift system is designed to (1) deliver the implant to the desired anatomical location by using cystoscopic guidance, (2) ensure delivery and attachment of the capsular tab onto the capsular surface, (3) customize the implant to the compressed lobe thickness at the point of delivery, and (4) allow the urethral end-piece to invaginate into the urothelium, thereby “hiding” the implant from exposure to the urine stream and promoting rapid covering and epithelialization over the end-piece. 12 For the 7 patients in the current cohort, 6 of the 22 device implants were found in aberrant locations. We do not know whether the outer nitinol tab was initially placed between the adenoma and the capsule, having never passed beyond the prostatic capsule, or whether it was placed beyond the capsule and then migrated into the prostate, such as by pressure necrosis. Additional studies would be needed to determine the mechanism that results in this device location, and whether the final location of the nitinol tab affects device functionality and patient outcomes. PUL was performed at outside institutions in all seven patients; thus, the experience level of the surgeons performing the PUL use of anesthetic is unknown. The common finding of implants at the bladder neck may be attributed to the angle of deployment for the device (Fig. 5), or possibly to migration. In the L.I.F.T. study for the UroLift device, routine cystoscopy was performed at 12 months. In 131 patients with 642 implants, 27 implants (4%) were identified as exposed to the bladder, and 14 experienced encrustation. Endoscopic removal of the encrusted device implants was performed in two patients who were symptomatic. 13 We expect enucleation to be without incidence in cases of properly placed PUL device implants, though foreign bodies within the adenoma will always complicate morcellation.
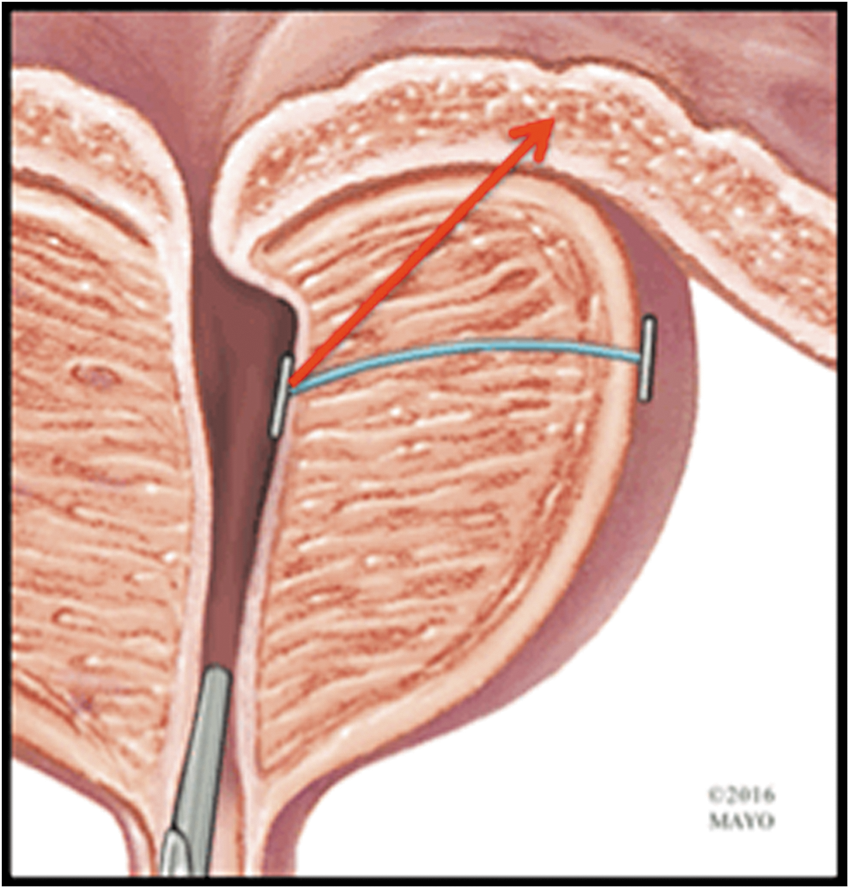
The trajectory of the red arrow is a possible mechanism of device placement into the bladder neck.
Morcellation was somewhat disadvantaged by the PUL device implants. All inner stainless steel portions of the implants became lodged in the morcellator, jamming the system and requiring a pause from morcellation. It is generally unfavorable to remove the morcellator instrument as this results in the cessation of continuous flow of fluid into the bladder and provides an opportunity for blood clot formation and decreased visualization. In each of the included index cases, there was relatively excellent hemostasis so this did not prove to be significant. We maintain a second morcellator instrument in all cases in the event that there is a mechanical failure. Awareness of this potential issue could change a surgeon's threshold to perform a cystotomy after HoLEP for removal of the enucleated tissue, a common practice for extremely large glands or glands that do not efficiently respond to morcellation.
Limitations of the current series include its retrospective nature and small sample size. The experience of the surgeons performing PUL is unknown. Our follow-up data are limited, but the purpose of this series was to detail the operative feasibility of HoLEP after PUL. Also, we cannot quantify the impact on the functionality of the morcellator blades resulting from entrapment of the PUL device components, but this could be of concern, particularly for multiuse morcellator blades.
Conclusion
Surgeons performing HoLEP or other transurethral procedures as secondary treatment after PUL may find device implants in areas other than the intended location, particularly for implants placed near the bladder neck. HoLEP can be performed safely and effectively post-PUL; however, morcellation of the adenoma tissue is complicated by metallic implants of the PUL device.
Footnotes
Author Disclosure Statement
No competing financial interests exist.