
Abstract
Purpose:
To investigate the contemporary trends and perioperative outcomes of percutaneous nephrolithotomy (PCNL) by using a population-based cohort.
Materials and Methods:
Using the Premier Healthcare Database, we identified 225,321 patients in whom kidney/ureteral calculi were diagnosed and who underwent PCNL at 447 different hospitals across the United States from 2003 to 2014. Outcomes included 90-day postoperative complications (as classified by the Clavien-Dindo system), prolonged hospital length of stay, operating room time, blood transfusions, and direct hospital costs. Temporal trends were quantified by estimated annual percentage change (EAPC) by using least-squares linear regression analysis. Multivariable logistic regression was performed to identify predictors of outcomes.
Results:
PCNL utilization rates initially increased from 6.7% (2003) to 8.9% (2008) (EAPC: +5.60%, p = 0.02), before plateauing at 9.0% (2008–2011), and finally declining to 7.2% in 2014 (EAPC: −4.37%, p = 0.02). Overall (Clavien ≥1) and major complication (Clavien ≥3) rates rose significantly (EAPC: +12.2% and +16.4%, respectively, both p < 0.001). Overall/major complication and blood transfusion rates were 23.1%/4.8% and 3.3%, respectively. Median operating room time and 90-day costs were 221 minutes (interquartile range [IQR] 4) and $12,734 (IQR $9419), respectively. Significant predictors of overall complications include higher Charlson comorbidity index (CCI) (CCI ≥2: odds ratio [OR] 2.08, p < 0.001) and more recent year of surgery (2007–2010: OR 3.20, 2011–2014: OR 4.39, both p < 0.001). Higher surgeon volume was significantly associated with decreased overall (OR 0.992, p < 0.001) and major (OR 0.991, p = 0.01) complications.
Conclusions:
Our contemporary analysis shows a decrease in the utilization of PCNL in recent years, along with an increase in complication rates. Numerous patient, hospital, and surgical characteristics affect complication rates.
Introduction
T
A recent article using the United States Nationwide Inpatient Sample described PCNL use from 1999 to 2011, noting its increase in utilization from 1.7/100,000 to 3.1/100,000. 3 As for other modalities of stone treatment, a Canadian population-based study using administrative data found a rise in ureterorenoscopy (URS) and a reciprocal decrease in extracorporeal shockwave lithotripsy (SWL) for kidney stone treatment. 4
Contemporary data have demonstrated that flexible URS is increasingly challenging PCNL in the treatment for medium- to large-sized kidney stones. 5 –8 Despite this, PCNL remains the standard of care for kidney stones >2 cm, with continued improvements to techniques and approaches. 1,2 A recent meta-analysis also found that standard PCNL conferred higher stone-free rates, although at the expense of higher complication rates, more blood loss, and longer hospital stay, compared with RIRS. 9 Given that limited updated data exist on contemporary utilization rates and outcomes of PCNL as well as on costs associated with the procedure, we aimed at characterizing national utilization trends, perioperative outcomes, and costs by using a contemporary population-based cohort.
Patients and Methods
Data source
After obtaining an institutional review board waiver for the use of anonymized HIPAA-compliant data, we utilized the Premier Healthcare Database (Premier, Inc., Charlotte, NC), a nationally representative all-payer database capturing more than 75 million hospital inpatient discharges. It represents ∼20% of all hospitalizations at more than 700 hospitals in the United States and features detailed information on a patient's hospitalization, including demographics, hospital characteristics, and complete billing information. Apart from International Classification of Diseases, Ninth Revision (ICD-9), this claims-based database provides standardized billing items, including direct item costs for all hospitalizations (e.g., medications, laboratory services, room and board, etc.). This database has been featured in prior landmark studies. 10 Using validated projection methodology, the data represent weighted estimates of hospital admissions. All numbers reported here refer to the weighted estimates.
Study population
Using ICD-9 codes, we identified individuals in whom kidney or ureteric calculi were diagnosed (592.0, 592.1, 592.9) and who underwent PCNL (55.04 or 55.03 combined with 55.21) between January 1, 2003 and December 31, 2014. Patients treated with PCNL were identified as previously described, by using ICD-9 procedural codes 55.04 for percutaneous nephrostomy with fragmentation and 55.03 for percutaneous nephrostomy combined with 55.21 for nephroscopy. 11
Study variables
We examined relevant patient, hospital, and surgical characteristics. Patient characteristics included age, gender (male vs female), race (White vs non-White), marital status (married vs non-married), insurance status (Medicare, Medicaid, private/commercial, other), and Charlson comorbidity index (CCI) (0, 1, ≥2). Hospital characteristics included teaching status (teaching vs non-teaching), size (<300, 300–499, ≥500 beds), urbanicity (urban vs rural), annual hospital PCNL volume, and U.S. geographic region (Midwest, Northeast, West, South). Surgical characteristics included annual surgeon PCNL volume and year of surgery (2003–2006, 2007–2010, 2011–2014). Hospital and surgeon volume was defined by the annual number of procedures undertaken by the hospital or surgeon during the year that the procedure was undertaken for that particular patient. This gives the most current status of a hospital or surgeon's volume status.
Outcomes
We determined the rates of 90-day complication defined according to the Clavien-Dindo classification (Clavien 1–5) by using ICD-9 codes as previously used. 12,13 Prolonged length of stay (LOS) was defined as >75th percentile of LOS (>4 days), as previously done. 11 We also evaluated operating room time (which referred to the total length of the procedure from the time that the patient is brought into the operating room till the time the patient leaves—“wheels in, wheels out”) and receipt of intra- or postoperative blood transfusion. Use of postoperative vasopressors and admission to the intensive care unit (ICU) were determined by using billing codes. Lastly, we calculated 90-day direct hospital costs, which included the cost of the entire procedure, inpatient stay, and any care for a maximum of 90 days postoperatively. All costs were adjusted to 2016 U.S. dollars by using the medical component of the Consumer Price Index.
Statistical analyses
For incidence of PCNL each year, we normalized this to population estimates from the latest 2014 U.S. Census Bureau (for years 2010–2014) and from intercensus estimates (for years 2003–2009). Temporal trends in rates were analyzed by estimated annual percentage change (EAPC), which uses the least-squares linear regression methodology. Next, we performed univariable analysis to evaluate outcomes. Categorical variables were summarized as proportions, whereas continuous variables were expressed as means (with standard errors) and medians (with interquartile ranges [IQRs]).
Finally, we assessed patient-, hospital- and surgical-related predictors of outcomes. We developed a multivariable logistic regression model controlling for all covariates to assess for independent predictors of outcomes, as listed earlier. Ninety-day direct hospital costs were found to have a gamma distribution, so we constructed generalized linear regression models. All statistical analyses were performed by using SAS 9.3 (SAS Institute, NC). All tests were two sided, and a p-value of <0.05 was considered statistically significant.
Results
Our final cohort consisted of a weighted sample of 225,321 patients who underwent PCNL by 3311 unique surgeons at 447 different hospitals across the United States from 2003 to 2014. Baseline characteristics are listed in Table 1. Temporal trends analysis showed a non-significant overall increase in the annual percentage of PCNL being performed (EAPC: +1.1%, 95% confidence interval [CI] −0.87%, +3.12%, p = 0.24), with an initial increase from 6.7% in 2003 to 8.9% in 2008 (EAPC: +5.60%, 95% CI 1.31%, 10.1%, p = 0.02), before plateauing between 2008 and 2011 at 8.9% to 9.0%, and finally significantly declining to 7.2% in 2014 (EAPC: −4.37%, 95% CI −7.27%, −1.37%, p = 0.02). The overall incidence of PCNL performed annualized to the U.S. population was 5.49/100,000 in 2003 and declined to 5.34/100,000 in 2014. Similar trends were noted when examining men and women separately (Fig. 1). There was an increasing trend in the age and proportion of patients with poorer CCI (Fig. 2).

Trend in incidence of PCNL hospitalization (from Premier Healthcare Database) in the United States from 2003 to 2014. PCNL = percutaneous nephrolithotomy.
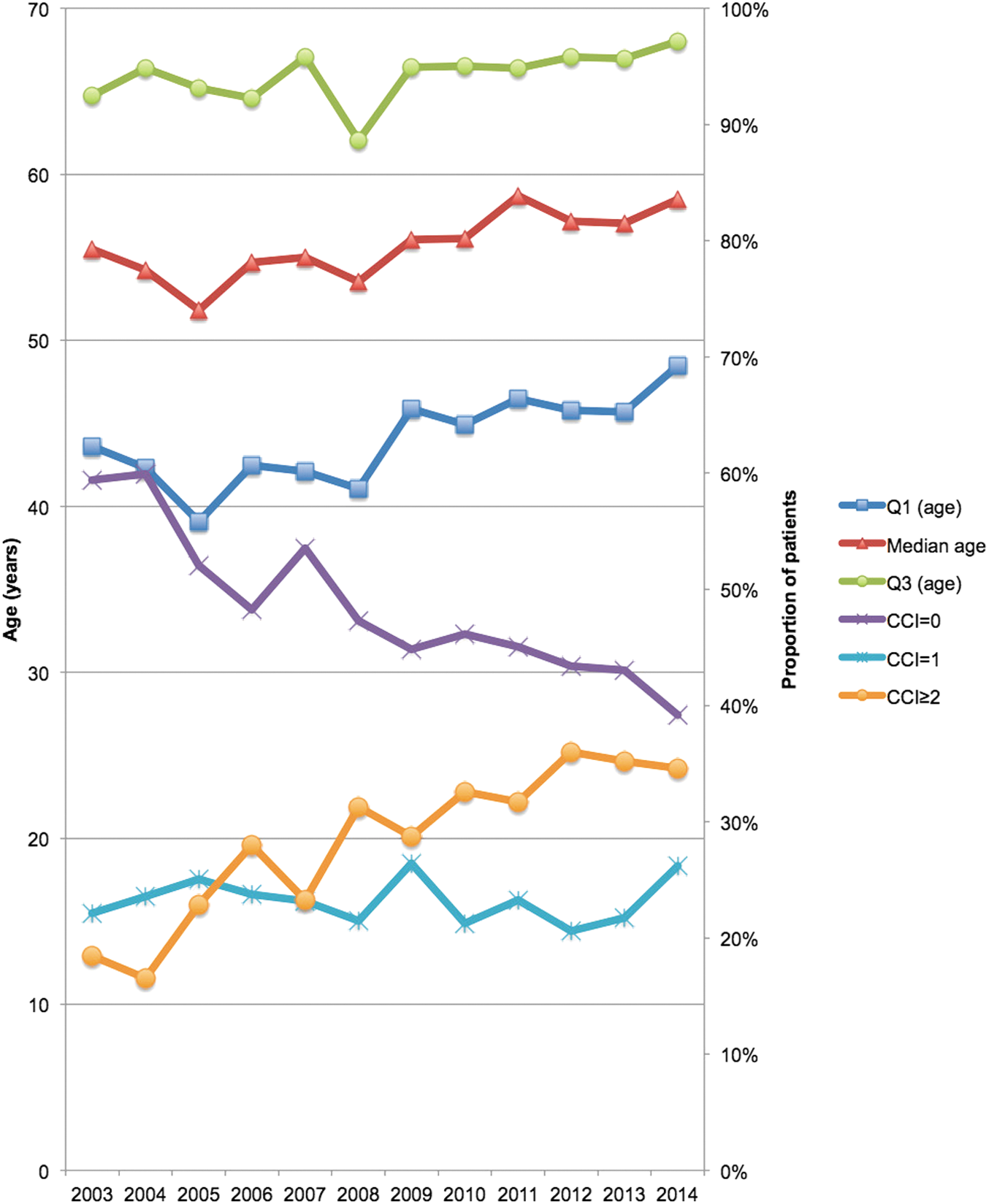
Trend of median age (interquartile range) and Charlson comorbidity index of patients who underwent PCNL from the Premier Healthcare Database in the United States from 2003 to 2014.
SE = standard error.
Overall complication rates saw an increasing trend from 6.6% in 2003 to 33.1% in 2014 (EAPC: +12.2%, 95% CI 6.63%, 18.07%); this was similar for major complication rates, from 0.4% in 2003 to 8.6% in 2014 (EAPC: +16.4%, 95% CI 6.94%, 26.60%; both p < 0.001) (Fig. 3). Overall and major complication rates were 23.1% and 4.8% during the study period. Median hospital LOS was 2.47 (IQR 3.09) days, with 28.0% of patients having a prolonged LOS (>4 days). A minority (3.2%) of patients required postoperative ICU admission, with use of vasopressors postoperatively at 5.3%. Trends in selected outcomes are graphed in Figure 3. Median operating room time was 159 (IQR 90) minutes. Median 90-day direct hospital costs were $12,734 (IQR: $9419) (Table 2).
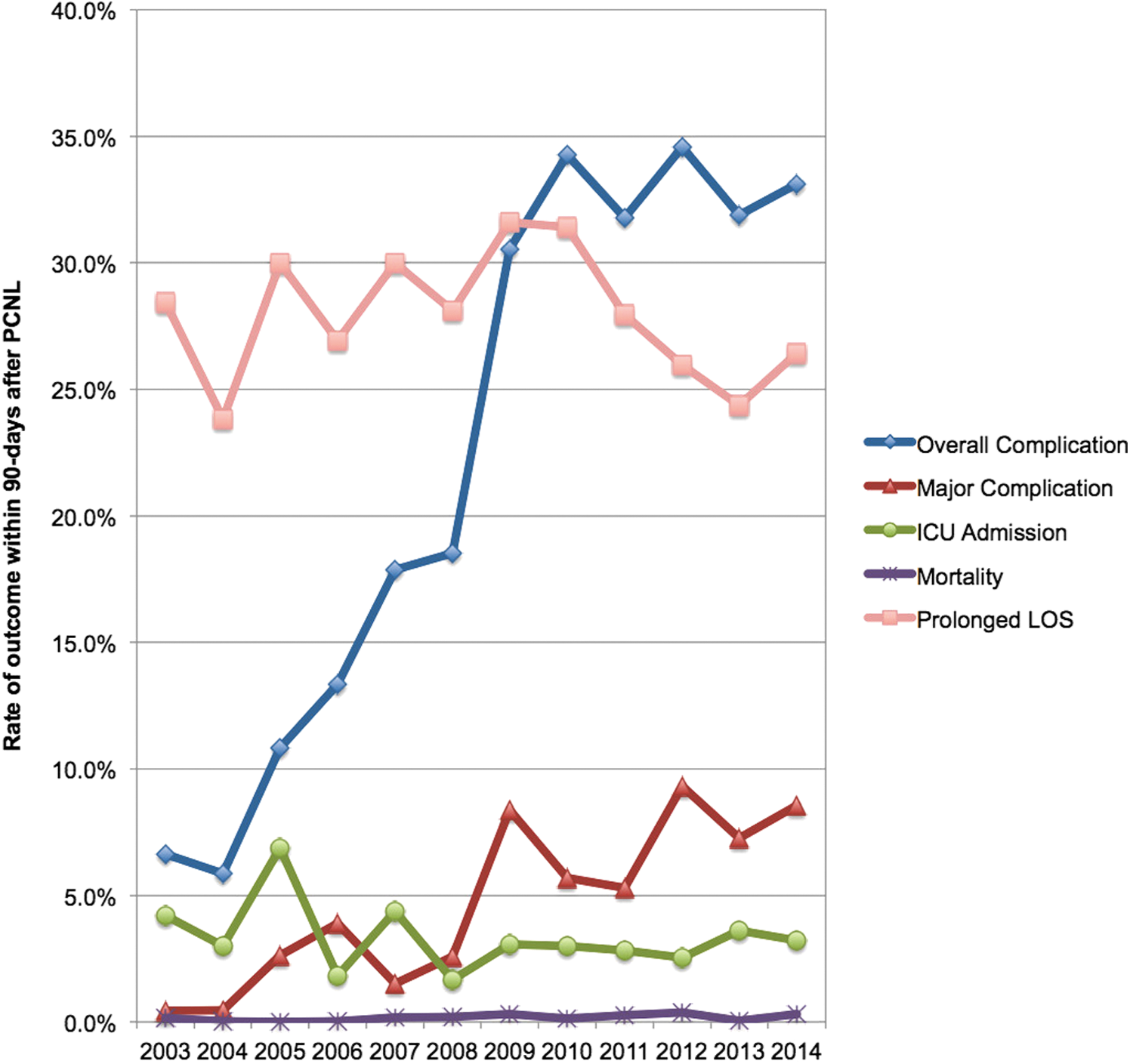
Trend of 90-day postoperative outcomes (rates of overall complication, major complication, ICU admission, mortality, prolonged length of stay) among patients who underwent PCNL from the Premier Healthcare Database in the United States from 2003 to 2014. ICU = intensive care unit.
Mean ICU LOS was calculated from only among those who were admitted to the ICU. Patients who did not require an ICU stay (i.e., ICU LOS = 0 days) were excluded from this calculation. bSimilarly, mean number of days of using vasopressors was calculated from only among those who required postoperative use of vasopressors. Those who did not have any postoperative use of vasopressors were excluded.
ICU = intensive care unit; IQR = interquartile range; LOS = length of stay.
Predictors of overall complications
Multivariable logistic regression identified the following significant predictors of overall complications: poorer CCI (vs CCI 0, CCI 2: odds ratio [OR] 2.08, 95% CI 1.94, 2.24, p < 0.001) and recent year of surgery (vs 2003–2006, 2007–2010: OR 3.20, 95% CI 2.92, 3.50; 2011–2014: OR 4.39, 95% CI 4.01, 4.80, both p < 0.001). Higher surgeon volume was significantly associated with lower overall complications (OR 0.992, 95% CI 0.988, 0.997, p < 0.001). Other predictors are listed in Table 3.
Predictors of major complications
On multivariable logistic regression, we found that increasing age was a significant predictor of major complications (OR 1.004, 95% CI 1.001, 1.008, p = 0.02) (Table 3). Other significant predictors of major complications include female gender (vs male, OR 1.46, 95% CI 1.31, 1.62, p < 0.001), non-married status (vs married, OR 1.26, 95% CI 1.13, 1.42, p < 0.001), Medicaid insurance status (vs Medicare, OR 1.79, 95% CI 1.50, 2.13, p < 0.001), higher CCI (vs CCI 0, CCI 1: OR 1.66, 95% CI 1.41, 1.95; CCI 2: OR 3.10, 95% CI 2.67, 3.60, both p < 0.001), and more recent year of surgery (vs 2003–2006, 2007–2010: OR 2.29, 95% CI 1.95, 2.70; 2011–2014: OR 3.32, 95% CI 2.83, 3.89, both p < 0.001). Higher hospital volume was also associated with major complications (OR 1.008, 95% CI 1.005, 1.012, p < 0.001), whereas higher surgeon volume was associated with decreased major complications (OR 0.991, 95% CI 0.984, 0.998, p = 0.01).
Predictors of prolonged LOS and 90-day direct hospital costs are listed in Table 3.
Discussion
We utilized a large population-based all-payer discharge database to evaluate the trends and outcomes of patients who underwent PCNL in the United States from 2003 to 2014. To the best of our knowledge, this study is the largest cohort of PCNL patients (N = 225,321), providing contemporary trends in its utilization and outcomes. During the study period, we found that the utilization of PCNL had initially increased to a peak of 6.97/100,000 in 2008, before decreasing gradually to 3.63/100,000 in 2014. The rise in incidence was congruent with findings from Stern and colleagues, who used the Nationwide Inpatient Sample from 1999 to 2011 (N = 105,180). 3 However, our findings of the subsequent decrease in the incidence of PCNL from 2008 to 2014 are new and noteworthy. Recent data had demonstrated an important increase in the use of URS over the past 10 years with a similar decrease in the use of SWL. 4,14,15 Over this same time frame, PCNL utilization remained stable. Contemporary data are now demonstrating that URS is not only having an impact on the utilization of SWL but may also affect the utilization of PCNL. It would appear that RIRS is beginning to selectively decrease the number of PCNL cases that are being performed in the United States.
Similarly, we found an overall increase in overall and major complication rates across the study period. This may be due to the medium-sized stones being increasingly managed with flexible URS, 9,16,17 leaving the larger and/or more complex staghorn cases to be managed with PCNL. Another possibility that can account for the higher rates of complications is the increasing age and proportion of patients with more medical problems (as indicated by higher CCI) across the study period. As such, it was not unexpected to find that poorer CCI was a significant predictor of overall and major complications. Patients with CCI ≥2 had more than twice the odds of developing postoperative complications and more than three times the odds of developing major complications after PCNL. This suggests the importance of careful patient selection for PCNL. It remains to be seen whether patients with poor CCI might benefit from a staged, flexible URS procedure instead of a more morbid PCNL procedure. 18 Interestingly, at the beginning of our study period, complication rates (6%–11%) were quite low. During this early time frame, it is plausible that flexible URS had not been widely adopted by most urologists, and, consequently, simple and smaller stones were still being managed by PCNL. A recent review of nephrolithometric scoring systems found that patients with Grade I–II Guy's stone score treated by PCNL had complication rates that were a maximum of 10%. 19
Through the use of billing codes, for the first time, we were also able to determine a population-based rate of 3.2% at postoperative ICU admission. This was similar to the 3% to 4% rate found in a 2002 to 2006 study using the Truven Health's MarketScan Database, which was limited to working-age adults and their dependents with employer-sponsored benefit plans. 20
Another interesting finding relates to that of surgical volume. We were able to evaluate both annual hospital and surgeon volume. Higher hospital volume was significantly associated with more overall and major complications. Although counterintuitive, this may be secondary to more complex cases being referred to higher-volume hospitals. 21 A study using the Nationwide Inpatient Sample found that complication and transfusion rates varied by case volume in a non-linear fashion, wherein rates were highest at the lowest and highest volume centers. 22
In contrast, we found that higher surgeon volume was significantly associated with decreased overall and major complications, as well as with decreased prolonged LOS. Notably, we were able to determine complications according to the recommended Clavien-Dindo classification system. 23 A 2012 Clinical Research Office of the Endourological Society (CROES) PCNL study found higher stone-free rates and lower complication rates at high-volume centers, among 3933 patients, even after adjusting for important clinical variables such as stone burden, urine culture status, American Society of Anesthesiologists (ASA) score, and the presence of staghorn stones. 24 Another nationwide study in Taiwan found that higher surgeon volume was associated with lower medical costs and shorter LOS after PCNL, but surgeon volume did not predict complications or mortality. 25 Our study did not find a significant decrease in direct hospital costs with higher hospital (p = 0.99) or surgeon volume (p = 0.10).
Our study is not devoid of limitations. First, this was a retrospective study using an administrative discharge database; therefore, it can be subject to misclassification bias. Second, we lacked important clinical information such as the location or size of the kidney stones, stone complexity grading systems (e.g., CROES nomogram 26,27 ), preoperative urine culture status, ASA score, or postoperative stone-free rates. From a list of 15 recommended outcomes to report for PCNL studies, 28 our study was able to report 5 outcomes (LOS, overall complication rate, operating time, blood transfusion, and cost). Third, we were not able to determine what type of PCNLs was actually performed, that is, supine vs prone, 29 standard vs mini vs ultra-mini vs micro. 30 In addition, we could not evaluate patients who underwent flexible URS, RIRS, or SWL, as these are usually day surgery cases that would not require overnight hospitalization; hence, we cannot draw any firm conclusions about trends in their use in comparison to PCNL. Lastly, this study was primarily based on clinical practice and costs in the United States and may not reflect those in other parts of the world.
Conclusions
This large contemporary population-based study provides new insight into the trends of utilization and outcomes of PCNL in the United States. We found an initial increase in the utilization of PCNL during the earlier study period, with a subsequent decrease in the more recent era. The contemporary decrease in the utilization of PCNL may be due to an increase in the use of flexible URS. In addition, increasing age, poorer comorbidity status, and possibly increasing complex cases that are being managed with PCNL may contribute to the rise in complication rates. Surgeon volume is an important factor in decreasing overall and major complications, as well as prolonged LOS. A variety of patient-, hospital-, and surgical-related characteristics have been found to affect outcomes and may have implications on referral patterns and patient selection.
Footnotes
Author Disclosure Statement
Q.D.T. is supported by an unrestricted educational grant from the Vattikuti Urology Institute, a Clay Hamlin Young Investigator Award from the Prostate Cancer Foundation, and a Genentech BioOncology Career Development Award from the Conquer Cancer Foundation of the American Society of Clinical Oncology. The remaining authors have no competing financial interests.