
Abstract
Purpose:
To evaluate the feasibility and outcomes of retroperitoneal laparoscopic nephrotomy along the Brodel line and tumor enucleation (TE) for complete intraparenchymal renal tumors.
Patients and Methods:
We retrospectively analyzed the medical charts of patients with complete endophytic tumors and who underwent retroperitoneal laparoscopic nephrotomy along the Brodel line and TE between 2012 and 2015. Perioperative data, surgical technique, pathologic variables, complications, functional, and oncologic outcomes were reviewed.
Results:
Twenty-one patients (mean age of 50 years; mean body mass index of 25.8 kg/m2) were treated with retroperitoneal laparoscopic TE along the Brodel line incision. The mean tumor size was 2.0 cm, and the mean RENAL score was 9.4. The main surgical outcomes were mean operative time of 94 minutes, mean estimated blood loss of 63 mL, and mean warm ischemia time of 28.4 minutes. Pathology showed clear renal cell carcinoma (n = 16), papillary renal cell carcinoma (n = 4), and reninoma (n = 1). No positive margin was found, and no perioperative complication occurred. The mean glomerular filtration rate of the affected kidney was 31.5 mL/minute/1.73 m2 three months after the surgery. In a median follow-up of 20 months (range of 4–36 months), no evidence of tumor recurrence or metastasis was found.
Conclusion:
For patients with complete intraparenchymal renal tumors, retroperitoneal laparoscopic parenchyma incision along the Brodel line and TE can be safely and effectively performed in centers with significant laparoscopic expertise.
Introduction
F
Laparoscopic PN (LPN) is a technically challenging procedure that requires advanced laparoscopic skills. However, with increased confidence and technical refinements, authors have demonstrated that LPN and robot-assisted PN (RAPN) are feasible, safe, and effective approaches for complex masses, including hilar and complete endophytic lesions. 4 –7 TE is a nephron-sparing procedure for small renal masses, particularly when the tumor is cortical. Recent studies on highly complex renal tumors treated with TE obtained favorable results. 3,8
The current study focused on the feasibility and outcomes of retroperitoneal laparoscopic nephrotomy along the Brodel line and TE for complete endophytic tumors around the renal sinus in highly selected patients in our center.
Patients and Methods
Patients and perioperative assessment
The study was reviewed and approved by the Institutional Review Board of the Chinese PLA General Hospital. Written informed consent was obtained from all participants before the initiation of the study procedures. Patients who had undergone retroperitoneal laparoscopic nephrotomy along the Brodel line and TE for a complete endophytic renal mass at our center from 2012 to 2015 were identified. Patient charts were reviewed to obtain demographic data, pre- and postoperative glomerular filtration rate (GFR), warm ischemia time (WIT), operative time, estimated blood loss, complications, length of hospital stay, pathologic results for tumors and margins, and follow-up functional and oncologic outcomes.
Preoperative assessment included emission CT (ECT), contrast-enhanced CT and MRI with detailed reconstruction of the renal vasculature. The relationship between tumor and renal vessels was studied. The inclusion criterion was a mass located posteriorly in the renal hilum close to the renal sinus (≤5 mm) with a clear boundary of the pseudocapsule and not visible on the renal surface at all on preoperative imaging (Fig. 1). The anatomical characteristics of renal masses on CT/MRI were quantified with a standardized nephrometry scoring system (RENAL Nephrometry Score). 9

Preoperative image of one patient. The tumor could be identified by MRI scan. The white arrow indicates the location of the renal tumor.
Surgical procedure
The patient was placed in the lateral decubitus position with the affected side up. The table was flexed, and kidney rest was raised to maximize the distance between the costal margin and iliac crest. We preferred a three-trocar technique for the retroperitoneoscopic operations as previously described. 10 In brief, a 2-cm skin incision below the 12th rib in the posterior axillary line (PAL) was made, the peritoneum was pushed forward by the index finger, and balloon expansion was performed to create the retroperitoneal working space. Under the direction of the index finger, a 5 or 12 mm trocar was inserted under the subcostal margin in the anterior axillary line, and a 10 mm trocar was placed above the iliac crest in the midaxillary line for the laparoscope. The third trocar was placed in the 2-cm incision. In several cases, a fourth trocar was added near PAL at the level of umbilicus for the assistant.
CO2 was bubbled to maintain a pressure of 12 mm Hg. Gerota's fascia was incised. The kidney was mobilized, and the upper pole fat remained to prevent the kidney from moving downward. The renal hilum was fully exposed in a similar manner as that for LPN, and the renal artery and vein were clamped temporarily by bulldog vascular clamps. Subsequently, a 200 mL mixture of ice water was administered to the renal surface to cool down the kidney.
After ultrasonic scalpel marking along the Brodel line of the kidney, a vertical incision was carefully made with cold monopolar scissors through the renal parenchyma until the tumor pseudocapsule appeared. The monopolar scissors, controlled by the right hand, alternated the blunt (closed) and sharp dissection of the enucleation plane with gentle pressure on the capsulated tumor tissue. The dissecting forceps, controlled by the left hand, helped expose the surgical field. The suction, controlled by the assistant, guaranteed a clear vision of the plane between the tumor and renal parenchyma (Fig. 2A–D). After enucleation of the entire tumor, hemostasis in the resection bed was achieved with electric coagulation. For suspected surgical margins, intraoperative frozen-section pathologic examination was carried out. Again, a 200 mL mixture of ice water was administered to cool down the renal parenchyma.
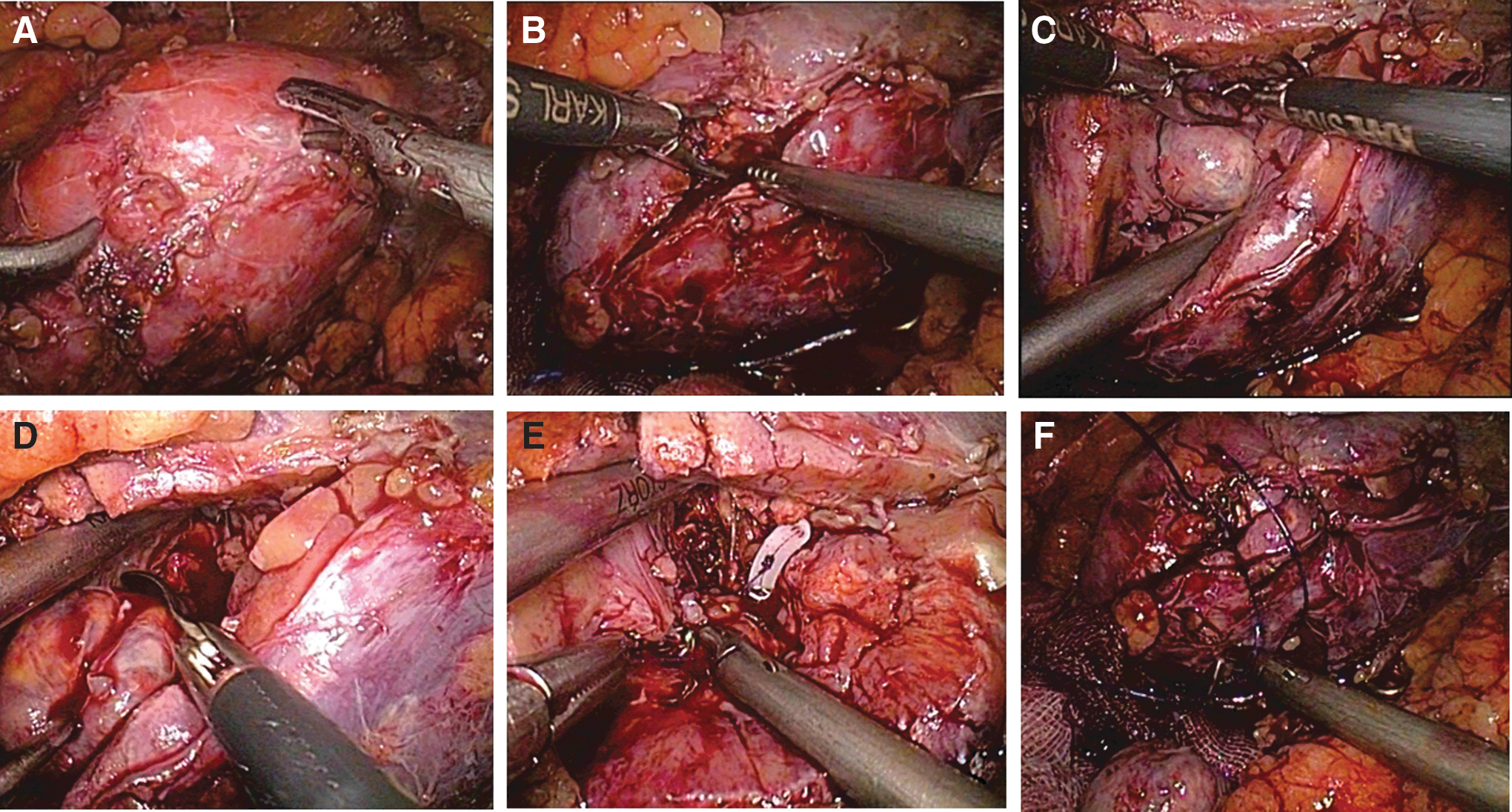
Retroperitoneal laparoscopic nephrotomy along the Brodel line and tumor enucleation.
Renorrhaphy was performed in two layers. First, the visible, opened collecting system and bleeding sites of the resection bed were carefully repaired with running sutures (Knotless Tissue-Closure Device, Quill, 4-0) with a Hem-o-lok clip applied to the free end. Second, the renal cortical defect was closed with running sutures (Knotless Tissue-Closure Device, Quill, 1-0) after placing hemostatic agents (Fig. 2E, F). The bulldog vascular clamp was removed, and hemostasis and global kidney perfusion were confirmed. The tumor was extracted in an endocatch bag for final pathologic analysis. A rubber drainage tube was routinely placed and removed when postoperative output was <50 mL/day. Positive surgical margin (PSM) was defined as tumor cells reaching the inked surface (Supplementary Video S1; Supplementary Data are available online at
Results
Overall, 21 patients were treated with retroperitoneal laparoscopic TE along the Brodel line incision. All procedures were completed laparoscopically with no need for open conversion. The patient demographics and tumor characteristics are summarized in Table 1.
BMI = body mass index; GFR = glomerular filtration rate; SD = standard deviation; WIT = warm ischemia time.
All tumors were centrally located (defined as abutting the central renal sinus or pelvicalyceal system during preoperative imaging). The mean tumor size on preoperative CT or MRI was 2.0 cm (range of 1.2–2.5 cm). According to the RENAL Nephrometry Scoring System, the mean score was 9.4 (range of 9–10). All the masses were located posteriorly to the kidney midline plane in the axial images, in contact with the renal sinus (two or three points for the “N” domain) and not visible on the renal surface (three points for the “E” domain) at all on preoperative imaging.
The mean WIT was 28.4 minutes (range of 24–40 minutes). The mean operative time was 94 minutes (range of 60–150 minutes). The mean estimated blood loss was 63 mL (range of 20–200 mL), and the mean postoperative hospital stay was 5.5 days (range of 5–6 days). All the patients had the drainage removed on postoperative day 3 with the output of <50 mL during the last 24 hours. No serious complications occurred during the perioperative period.
Histopathology confirmed clear renal cell carcinoma (n = 16), papillary renal cell carcinoma (n = 4), and reninoma (n = 1). All patients had negative surgical margins. In the 3-month follow-up, no patients experienced a significant change in GFR of the affected kidney with a mean of 31.5 mL/minute/1.73 m2 (range of 24–38 mL/minute/1.73 m2) compared with preoperative levels with a mean of 36.2 mL/minute/1.73 m2 (range of 30–43 mL/minute/1.73 m2). In the median follow-up of 20 months (range of 4–36 months), no evidence of tumor recurrence or metastasis was found (Fig. 3).

Postoperative follow-up of the patient. The operative site could be identified by CT scan. The black arrow indicates the operative site after tumor enucleation.
Comments
This report presents a single center's retroperitoneal laparoscopic experience in managing complete endophytic tumors. The results show that TE after parenchyma incision along the Brodel line is a safe and feasible method for highly selected patients.
For patient groups with challenging tumors, studies on technique modifications and the outcomes of LPN or RAPN have already been published. 4 –7 Gill and colleagues 4 reported that 55 of their 800 patients with a complete intraparenchymal tumor were treated by LPN. Under intracorporeal ultrasound (US) guidance, the tumor margins and the extent of parenchymal involvement were accurately delineated. The mean WIT was 29.9 minutes without PSM. The robotic series carried out by Autorino and colleagues 5 also obtained a favorable result. Intracorporeal US was used to guide tumor resection with an adequate margin of normal parenchyma, and PSMs occurred in 3 of the 48 patients.
In the present study, we exposed the tumor without the guidance of US by incising the renal parenchyma along the Brodel line because of the special tumor location. With blunt and sharp dissection of the tumor pseudocapsule, TE was performed without PSM. The Brodel line is a relatively avascular plane near the midline (5 mm posterior) of the convex border of the kidney, through which the collecting system of the kidney could be entered. Nephrotomy along the Brodel line and dissection through the collecting system were performed in previous studies for patients with complex staghorn calculi through laparoscopic and robot-assisted procedures. 11,12 We adopted this method to treat patients with complete endophytic and posteriorly located renal tumors. A big incision along the Brodel line was made to better expose the tumor. The tumor might be located more accurately with smaller incision under the guidance of intracorporeal ultrasound, thus, the WIT could also be reduced. However, intraoperative US was not used in the present patient series.
Opinions on performing standard PN or TE are varied. 13 Advocates of TE refer to comparative studies on reduced PSMs for TE compared with standard PN. No consensus has been reached with regard to the management of PSM after PN. Upon positive margins, options include observation, repeat PN, ablation of the surgical bed, and RN. 14 Permpongkosol and colleagues 15 presented their midterm outcomes of seven patients with PSMs with surveillance. One patient with von Hippel–Lindau disease died of metastatic renal cell carcinoma in the pancreas 10 months after LPN. The remaining patients were disease-free in the median follow-up of 32 months. Meanwhile, studies have shown that for high-risk (e.g., pT2-pT3a or Fuhrman grade III–IV) renal tumors, PSM is significantly associated with a high risk of recurrence (HR 7.48, p < 0.001). 16
Numerous studies have demonstrated that TE provides oncologic outcomes comparable to those of wedge resection, with the benefit of maximal preservation of renal parenchyma and optimized function. 3,8 Mir and colleagues 17 observed in their study that the ultimate renal function after PN is primarily driven by parenchymal preservation, with ischemia playing a secondary role as long as it is within a limited period. In his study, Simmons conducted multivariate analysis and claimed that percent functional volume preservation and WIT are associated with nadir GFR, whereas only percent functional volume preservation is associated with late GFR. 18 Laying ice slush around the kidney is the most common technique used in open PN for surface cooling. Methods of surface cooling have also been developed for LPN and are recommended when WIT is expected to exceed 20 minutes. After exposure to ice slush, a safe ischemia time of 35 minutes at the maximum has been described. 19
In the current study, TE was performed with a mean WIT of 28.4 minutes (range of 24–40 minutes). In our previous study on robot-assisted and laparoscopic PN for complex renal tumors with a RENAL Nephrometry Score of ≥7, the mean WIT were 20.5 and 22.3 in each group, respectively. 20 The WIT in the TE group was relatively longer than that in the robot-assisted and laparoscopic PN groups, a result that may be explained by the more complex anatomy of the current group (e.g., close to the collecting system). In the 3-month follow-up, the mean GFR of the affected kidney was 31.5 mL/minute/1.73 m2 (range of 24–38 mL/minute/1.73 m2), which is comparable to preoperative levels with a mean of 36.2 mL/minute/1.73 m2 (range of 30–43 mL/minute/1.73 m2). Kidney ECT was not routinely applied in the latest follow-up of all the patients; however, the serum creatinine levels of the patients recovered to the preoperative level, which indicates good functional recovery after surgery to a certain extent.
The limitations of the present study include limited patient series, short follow-up period, and retrospective nature. Nevertheless, to our knowledge, this article presents the first case series performing laparoscopic parenchyma incision along the Brodel line and TE defined by the RENAL Nephrometry Score, and it strengthens the growing evidence that laparoscopic TE is safe and effective for patients with challenging renal tumors. The strengths of this study include randomized trial, relatively large number of patients and long follow-up time. Further study with the application of intraoperative US for this kind of specially localized renal tumors should also be carried out.
Conclusion
In conclusion, we described our technique, illustrated with Supplementary Video S1, of retroperitoneal laparoscopic parenchyma incision along the Brodel line, and TE for complete intraparenchymal renal tumors. This laparoscopic procedure can be safely and effectively performed in centers with significant laparoscopic expertise.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.