
Abstract
Introduction:
Current treatment practices within the field of endourology require the routine use of radiation exposure to provide adequate imaging during urologic procedures. One such procedure requiring repeated radiation exposure during treatment is ureteroscopy. We set out to compare estimated fluoroscopic radiation exposures employing fixed table and portable C-arm fluoroscopy.
Materials and Methods:
A cross-sectional dosimetry phantom model was placed supine on both fixed fluoroscopy and standard operating room tables. The models were then exposed to three separate 5-minute runs of fluoroscopic exposure. Metal oxide semiconductor field effect transistor dosimeters were utilized in organ-specific locations to determine specific radiation exposure dosages. Absorbed radiation was determined for each organ location for both fluoroscopy units. Organ dose volumetric corrections were performed for skin and red bone marrow, to correct for the nonirradiated portion. Organ dose rate (ODR, mGy/s) and effective dose rate (EDR, mSv/s) were calculated, with values reported as mean ± standard deviation.
Results:
There were found to be statistically significant elevations for both total EDR and organ-specific dose rates with the use of fixed table fluoroscopy compared with C-arm fluoroscopy. EDR was found to be 0.0240 ± 0.0019 mSv/s for the fixed table unit and 0.0029 ± 0.0005 mSv/s for the C-arm unit (p = 0.0024). Internal organs exposed to the most radiation during fixed table fluoroscopy included the gall bladder and stomach in comparison to C-arm fluoroscopy, which found elevated exposure in the kidneys, pancreas, and spleen.
Conclusion:
The routine use of fixed table fluoroscopy results in significantly elevated estimated organ doses and EDR when directly compared with C-arm fluoroscopy in model trials. This difference should be taken into consideration by practicing urologists when patient treatment requires the use of fluoroscopy to maintain radiation exposure as low as reasonably achievable.
Introduction
P
Numerous fluoroscopy devices are used during endourologic procedures, including fixed fluoroscopy tables and C-arm portable units. Some fixed table units employ an over-the-table radiation source; meanwhile, the energy source on most C-arm units is placed under the table. Absorbed radiation dose tends to be the highest near the X-ray emitter, 2 so the distribution of organs affected by the radiation beam will be affected by the location of the radiation source. Also, organs exposed to fluoroscopy have different radiosensitivities and we believe that the over-the-table approach results in more radiation exposure to anteriorly located, radiosensitive organs compared with the under-the-table radiation source. The consequence would be increased overall radiation absorption during ureteroscopy with an over-the-table radiation source. Our objective was to estimate patient radiation exposure during fluoroscopy with either an over-the-table radiation generator (fixed table) or an under-the-table radiation generator (portable C-arm) using a validated anthropomorphic adult male model.
Materials and Methods
Anthropormophic phantom, MOSFET dosimeters, and fluoroscopy units
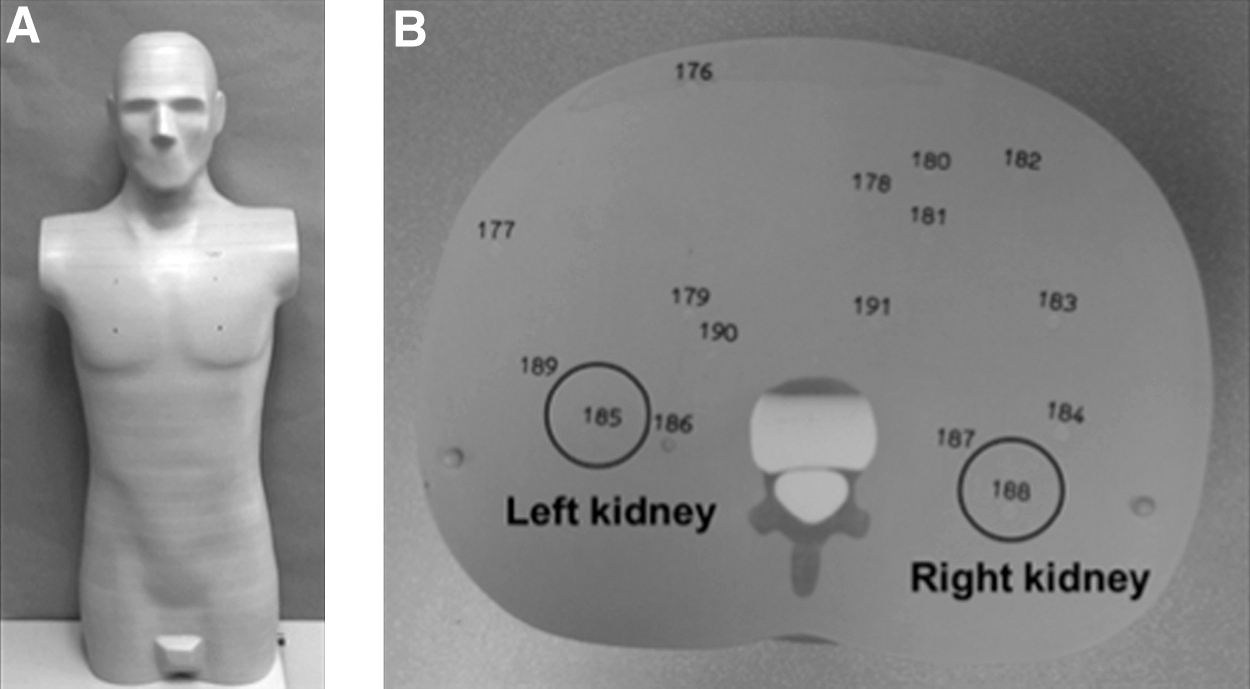
An anthropomorphic male phantom (Model 701-D CIRS, Norfolk, VA) validated for organ dosimetry was used (Fig. 1A). The phantom model is 173 cm tall, 73 kg and composed of 39 adjacent axial slices, each of which is 25 mm thick. Internal organs are represented in each slice and have specific numbered locations, which are optimized for organ dosimetry (Fig. 1B). Specialized high-sensitivity TN-1002RD MOSFET dosimeters (Best Medical, Ottawa, Ontario, Canada) were used to measure organ dosages (Fig. 2).
Nonobese adult male phantom

Specialized high-sensitivity TN-1002RD MOSFET dosimeters (Best Medical, Ottawa, Ontario, Canada) placed at specific organ sites to measure organ dosages.
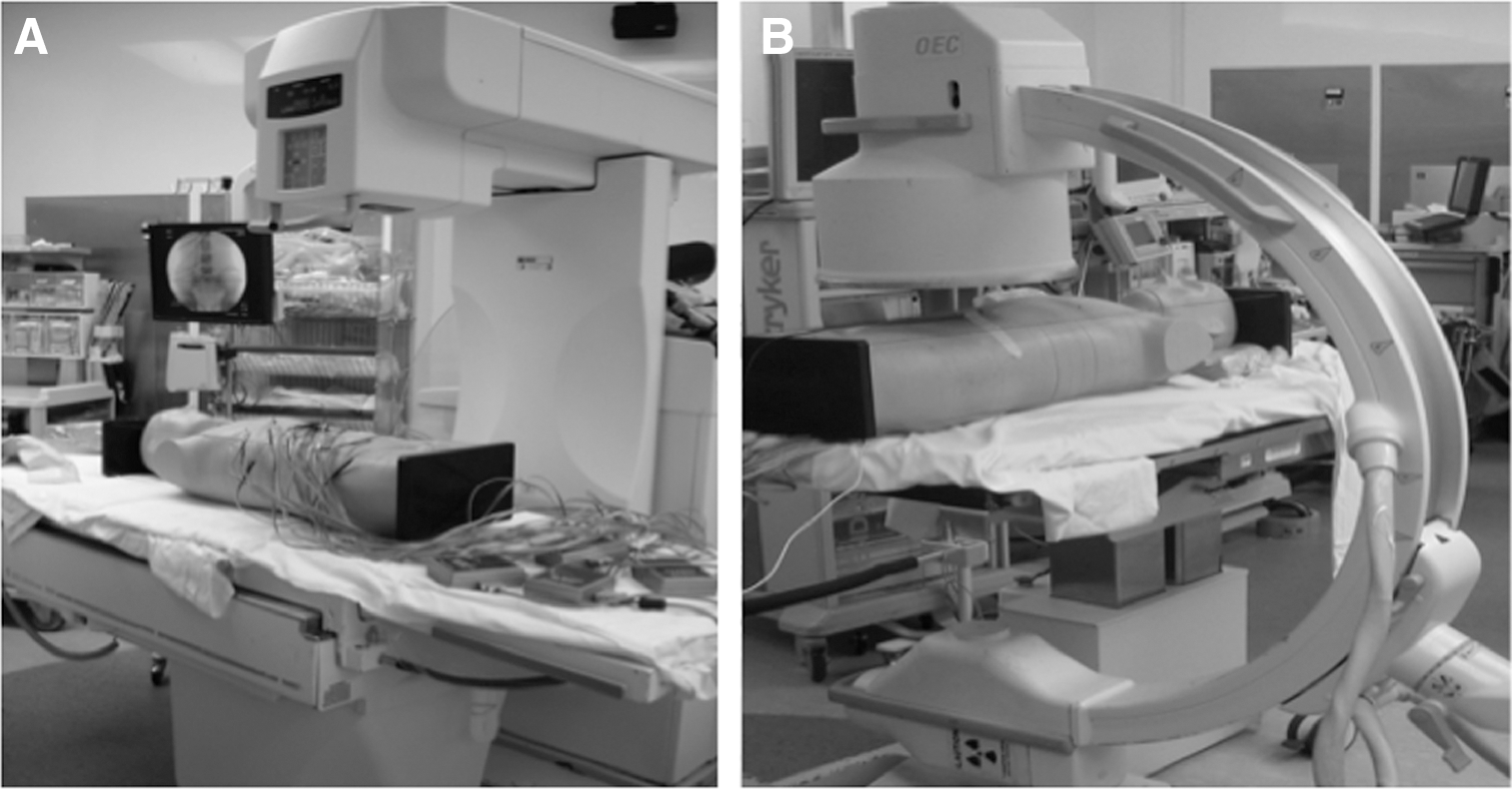
An OEC Uroview 2800 fixed fluoroscopy unit with 36 cm intensifier (GE, Little Chalfont, United Kingdom) and an OEC 9800 Plus C-arm with 30 cm intensifier (GE) were used to perform fluoroscopy. The UroView 2800 (Fig. 3A) is a fixed fluoroscopic X-ray system, including a patient-support table with overhead X-ray tube assembly. The OED 9800 C-arm (Fig. 3B) is a portable unit with its X-ray emitter arising below the table.
Positioning of phantom and fluoroscopic units
Simulated ureteroscopy and dosimetry
Twenty MOSFET dosimeters were placed at specific organ sites in the phantom (Fig. 4). Fluoroscopy was performed in the straight anterior to posterior (AP) orientation with the phantom in supine position. For both fluoroscopy units, fluoroscopy settings were determined by the fluoroscopy unit's automatic brightness control and provided with an ideal image that would allow ureteroscopy. The image was collimated to include the renal units, with the ureters and the bladder.

Phantom fluoroscopic image.
Initial testing was performed with the OEC UroView 2800 fluoroscopy table. Three 5-minute runs of fluoroscopy were performed at a setting of 80 kVp and 3.0 mA. The phantom was then placed on a ureteroscopy table (IDI 100UC; Image Diagnostics, Fitchburg, MA), and the C-arm was centered over the location of the phantom. Three 5-minute runs at the setting of 80 kVp and 1.0 mA were performed. Machine-specific pulse exposure settings were determined by utilizing their respective automatic rate control abilities on a low-dose setting. The distance from the image intensifier to the model with the C-arm model was minimized as we do in standard practice to minimize radiation distance traveled while still providing an adequate picture. This distance was kept standard for each C-arm run. The length of radiation time was chosen to be 5 minutes as required for dosimetry equipment to properly register exposure within the phantom model.
Specific absorbed radiation in mGy was determined for each organ location during each 5-minute run for both fluoroscopy units. Organ dose volumetric corrections were performed for skin and red bone marrow, to correct for the nonirradiated portion. Estimated exposed area corresponded to 18% and 20% pf the total skin and bone marrow area, per previous studies. Organ dose rate (ODR) in mGy per second were calculated by dividing by organ dose by fluoroscopy time. Effective dose per fluoroscopy unit was calculated with the ODR of all organs by using the International Commission on Radiological Protection Publication (ICRP) 103 formula and tissue weighing factors (Wt). Equivalent dose rate presented in mSv per second was calculated for both fluoroscopy units.
We compared ODR and EDR between the C-arm and fixed table and performed an unpaired t test for statistical analysis. Type I error was set as alpha = 0.05, and the analysis was performed with JMP (SAS Institute, Cary, NC). Mean and standard deviations are reported. Values are reported as mean ± standard deviation (SD) unless otherwise specified. A Holm-Bonferroni method was applied for multiple comparisons in the EDR data.
Results
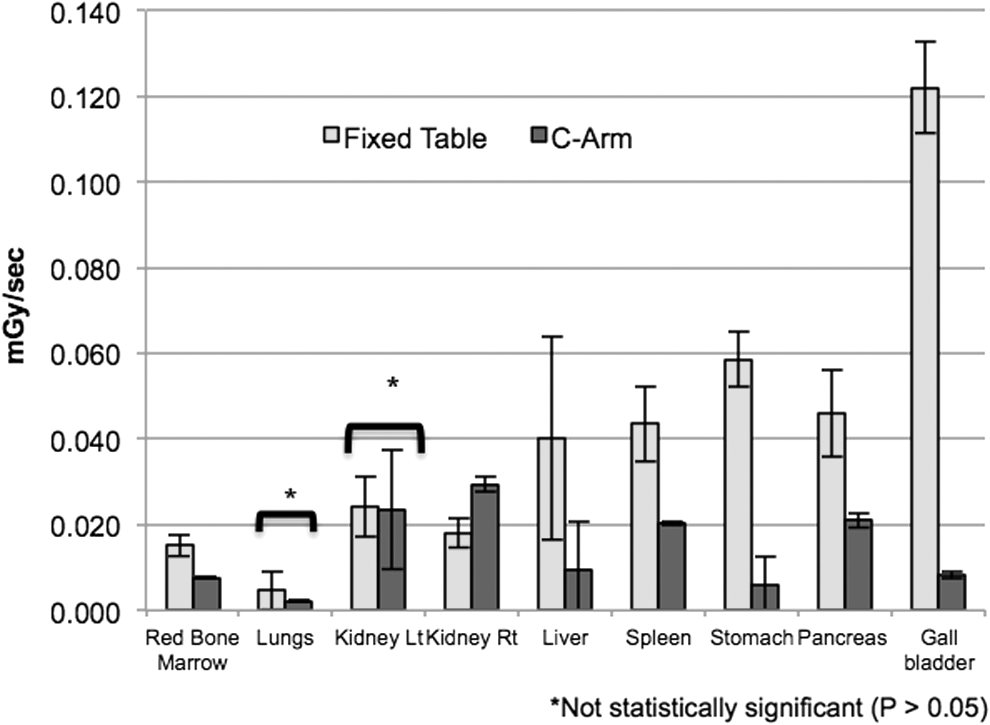
The table lists organ-specific dose rates for the fixed table and C-arm (Table 1). Of the organ-specific dose rates, dosimeters in the model's skin reported the highest levels of absorbed radiation (mean ± SD 0.329 ± 0.005 mGy; mean ± SD 0.007 ± 0.0001 mGy) for the fixed table and C-arm, respectively. Also, most internal organs were exposed to significantly greater doses with the fixed table compared with the C-arm (Fig. 5). The internal organs exposed to the most radiation with the fixed table included the gall bladder and stomach (mean ± SD 0.1221 ± 0.0106 mGy; mean ± SD 0.0586 ± 0.0065 mGy), respectively. The kidneys and, to a lesser degree, the pancreas and spleen absorbed most of the radiation during fluoroscopy with the C-arm.
Organ-specific dose rates (mGy/s) for the fixed table and C-arm.
SD = standard deviation.
The total ureteroscopy EDR was significantly higher by an order of magnitude during over-the-table radiation generation with fixed table compared with under-the-table radiation generation by portable C-arm at 0.0240 ± 0.0019 mSv/s and 0.0029 ± 0.0005 mSv/s, respectively (p = 0.0024) (Fig. 6).
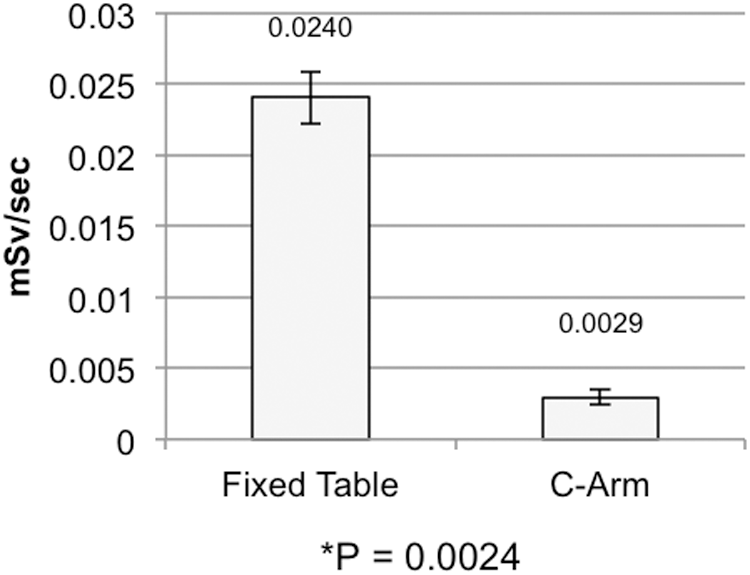
Effective dose rate for the fixed table and C-arm (mSv/s).
Discussion
Imaging technology is essential for the diagnosis and management of patients with urolithiasis. However, the annual per capita radiation exposure from medical sources in the United States has risen significantly from 0.54 mSv in 1980 to 3.0 mSv in 2006. 3 Further, the prevalence of kidney stones is on the rise and these stones will recur in a maximum of 50% of patients within 5 years. 4 Patients who are found to have a stone undergo an average of four imagings during the first year. 5 This has led to growing concern over radiation exposure in patients with urolithiasis, who undergo repeated diagnostic imaging studies and fluoroscopic procedures. The main concern is the lifelong risk of malignancy in patients with urolithiasis given the chronic exposure to radiographic imaging. A rough estimate of 29,000 future cancers in the United States can be attributed to the CTs performed in 2007 alone. 6
There has been a practice pattern change in the surgical management of urolithiasis, and many stones that were previously treated with SWL are currently treated with ureteroscopy. 7 Fluoroscopy, which is commonly performed during ureteroscopy, contributes to overall patient radiation exposure. The median equivalent dose for a nonobese man undergoing ureteroscopy has been reported to be 1.13 mSv, which is similar to the radiation from a KUB. 8 However, fluoroscopy times can be highly variable and depend on patient factors, including stone burden, location, ureteral dilation, and complex anatomy. Lowe and colleagues showed increased fluoroscopy times during complicated procedures. 9 The “ALARA” or “as low as reasonably achievable” principle has been recommended as a measure to reduce fluoroscopic times. 1 These include collimation to working area, placing image intensifiers closer to the patient, pulsed fluoroscopy, and last image hold. While following these principles, and tracking fluoroscopic times, Ngo and colleagues recorded a 24% decrease in fluoroscopy times during ureteroscopy. 10 Other techniques, including laser-guided fluoroscopy, tactile feedback guidewire placement, and stent placement under direct cystoscopic vision, have shown to be effective in reducing fluoroscopic times. 11 Lastly, some have reported a minimal-use protocol, which reduced mean fluoroscopy time to 3.3 s. 12
Fluoroscopy time alone is a poor measure of radiation exposure and absorbed patient dose, since it does not reflect patient size, machine mode, or radiation beam distribution. 13 Therefore, other factors, including energy source location, source to skin distance, patient thickness, and machine setting, are likely involved. Nakano and colleagues published that over-the-table fluoroscopy increases the radiation dose to the operator's hands more than under-the-table fluoroscopy during orthopedic procedures. 14 In our study, we compared a fixed table OEC Uroview 2800 (GE) with an over-the-table radiation source to a C-arm OEC 9800 Plus (GE) with an under-the-table radiation source. Interestingly, the majority of organs were exposed to more radiation by using the fixed table. Also, there was a 10-fold increase in total effective dose rate while using the fixed table. The utilization of exposure dosages of 80 kVp/3 mAs for fixed table and 80 kVp/1 mAs for c-arm were chosen while allowing for machine specifications required to equal a maximum voltage of 80 kVp. This difference in settings may aid in the increased difference between effective dose rate, but this also helps represent a clinical disparity between the devices in achieving similar endpoint imaging results. With these settings being standardized for each imaging device, we feel that our findings correctly represent EDR seen with common current devices used in clinical practices.
To our knowledge, this is the first article comparing organ-specific dose rate and EDR for over-the-table and under-the-table fluoroscopy by using a validated dosimetry model. We know that radiation from fluoroscopy is not distributed evenly and some organs are more exposed than others. The skin entrance is exposed first and absorbs the most radiation, followed by the gall bladder, stomach, and pancreas. Radiation absorption in these organs was significantly higher while using our over-the-table fixed fluoroscopy unit since these organs are mainly anteriorly located. The kidneys were exposed to slightly increased radiation with the portable under-the-table C-arm, since they are posteriorly located. In addition, these organs have different radio sensitivities according to data acquired from Japanese atomic bomb survivors. 15 Organs with higher radio sensitivity (WT) include the stomach, pancreas, gall bladder, and bone marrow. As such, the effective radiation dose absorbed by those organs will be higher compared with organs with a low WT such as the skin and kidneys.
It is important for urologists to understand the amount of radiation that they expose their patients to. Providers should also be familiar with the fluoroscopy units available at their institution and make efforts to reduce fluoroscopy, especially when using an over-the-table fluoroscopy unit. Some providers favor fixed fluoroscopy units since they are easily controlled by the surgeon and do not require a fluoroscopy technician. The X-ray emitter in the C-arm is portable, which allows versatility with operating room planning. Also, the C-arm can be rotated easily, which allows better access to the patient during percutaneous procedures. Also, during fluoroscopy with the C-arm, the table leads to some radiation scatter, which further affects total radiation absorbed by the patient.
There are some limitations with our study. A phantom was used to measure ODR and total EDR, which are estimates of actual radiation dosage from ureteroscopy. The phantom model and dosimetry equipment required a 5-minute period of uninterrupted exposure for sensitivity to be compared. This time frame does differ from currently reported fluoroscopic times during ureteroscopy, ranging from 2.5 to 3 minutes, but it was necessary for radiation detection by the dosimeter equipment. 10,16,17 Also, testing was performed with only one specific model of the fixed table and C-arm. More recent fixed table designs may have newer features to reduce radiation exposure to patients, including a below-the-table radiation source and improved collimation. Further testing with additional fixed table and C-arm models is warranted to verify the relevance of our findings. Lastly, our phantom model used has a male configuration, which does not consider female-specific organs, including breasts, uterus, and ovaries. Also, the amount of scatter radiation and the total absorbed radiation to staff and operator was not measured in this study.
Conclusion
Fluoroscopy used during ureteroscopy contributes to overall radiation exposure in patients with urolithiasis. Effective absorbed radiation is highly variable during ureteroscopy and frequently depends on fluoroscopy time, machine settings, and patient factors. We observed a 10-fold increase in total effective dose rate with the practical use of an over-the-table fixed fluoroscopy unit compared with an under-the-table C-arm. Further studies with additional fixed table and C-arm models should be performed to determine whether these results are reproducible. However, we believe that these results should still lead providers to become more familiar with the fluoroscopy units available at their institution. Thus, these would enable them to make appropriate efforts toward reducing fluoroscopy exposure to patients, especially when the choice of utilizing an over-the-table fluoroscopy unit versus an under-the-table fluoroscopy unit exists.
Footnotes
Author Disclosure Statement
No competing financial interests exist.