
Abstract
Introduction:
Ureteroscopy (URS) is the most common surgical treatment of urolithiasis and can be problematic in patients with a bleeding diathesis. The intent of this review is to systematically review the literature to assess the safety and efficacy of ureteroscopic procedures in these groups of patients.
Methods:
The systematic review was performed according to the Cochrane diagnostic accuracy review guidelines. The search strategy was conducted to perform a comprehensive database search (1990–2017). A cumulative analysis was done and where applicable a comparative analysis between bleeding diathesis patients and those without.
Results:
Eight studies included were all published between 1998 and 2016 with the total number of participants with bleeding diatheses being 1109 with an age range of 18–97. Overall stone-free rate across the studies was 90.8% vs 86.2% in the control group. There was no significant difference in complications between the bleeding diathesis group and control group (N = 12,757, p = 0.07, 95% confidence interval [CI] 0.92, 6.02, I2 = 78%). Pooled analysis for bleeding-related complications shows a statistically significant difference favoring the control arm (N = 12,757, p ≤ 0.0001, 95% CI 1.81, 5.73, I2 = 0%). Pooled analysis for thrombosis shows no statistically significant difference between the bleeding diathesis group and the control arm (N = 118, p = 0.67, 95% CI 0.23, 9.86, I2 = 48%).
Conclusion:
The use of URS with or without the holmium laser is a safe and efficient modality for treating patients with urolithiasis who also have a bleeding diathesis or are anticoagulated or on antiplatelet agents. However, this review would suggest that the increased risk of procedure related bleeding is not insignificant and a patient-centered approach should be taken with regards to continuing these agents or not correcting bleeding diatheses.
Introduction
U
Despite the evolution in optics and miniaturization of ureteroscopes, many urologists still tend to correct any coagulopathy before upper tract endourologic procedures. 5 This tendency can be problematic in some patients, where coagulopathy correction is not an option (i.e., metallic heart valves, high risk of deep vein thrombosis [DVT], and pulmonary embolism). Such patients are often not suitable for other treatments such as percutaneous nephrolithotomy (PCNL) or SWL. Another challenging cohort of patients are ones with a bleeding diathesis in whom an endourologic procedure needs to be done in the emergent setting. 6
Elkoushy and coworkers summarize the dilemma succinctly; anticoagulated patients often have multiple comorbidities, which in addition to the thrombogenic nature of surgery further increases their risk of thromboembolic episodes. 7 Surgeons must therefore balance the need to reduce the risk of thrombosis with the need to reduce the risk of bleeding by continuing antiplatelet (APT) or anticoagulation therapy or not correcting coagulopathies.
A previous systematic review on this topic has shown that it was safe to proceed with URS procedures in these groups of patients. However, the evidence was derived from only three available studies of low quality comprising 73 procedures. 5 This article formed a part of recent American Urological Association (AUA) guidelines on the topic “URS can be performed with continuing oral anticoagulation and APT therapy”. 8 Since then, further studies have emerged on this topic on the viability of URS in patients with bleeding diatheses. The intent of this review is to systematically review the literature to assess the safety and efficacy of ureteroscopic procedures in patients with bleeding diatheses.
Methodology
Search strategy and study selection
The systematic review was performed according to the Cochrane diagnostic accuracy review guidelines. The search strategy was conducted to find relevant studies from MEDLINE (1990–March 2017), EMBASE (1990–March 2017), Cochrane Central Register of Controlled Trials—CENTRAL (in The Cochrane Library—Issue 1, 2017), CINAHL (1990–March 2017),
Terms used included: “ureteroscopy”, “coagulopathy”, “anticoagulant”, “warfarin”, “bleeding”, “urolithiasis”, “aspirin”, “coumarin”, “clopidogrel”, “thrombocytopenia”, and “calculi”. Mesh phrases included: (“Ureteroscopy”[Mesh]) AND “Blood Coagulation Disorders”[Mesh], (“Anticoagulants”[Mesh]) AND “Ureteroscopy”[Mesh], (“Ureteroscopy”[Mesh]) AND “Hemorrhage”[Mesh], (“Anticoagulants”[Mesh]) AND (“Lasers”[Mesh] OR “Laser Therapy”[Mesh]), ((“Lasers”[Mesh]) AND “Calculi”[Mesh]) AND “Anticoagulants”[Mesh], (“Anticoagulants”[Mesh]) AND “Calculi”[Mesh], (“Ureteroscopy”[Mesh]) AND “Aspirin”[Mesh], (“Ureteroscopy”[Mesh]) AND “clopidogrel” [Supplementary Concept], (“Ureteroscopy”[Mesh]) AND “Coumarins”[Mesh], and (“Ureteroscopy”[Mesh]) AND “Thrombocytopenia”[Mesh], (“Kidney Calculi”[Mesh] OR “Ureteral Calculi”[Mesh]) AND “Aspirin”[Mesh], (“Coumarins”[Mesh]) AND (“Kidney Calculi”[Mesh] OR “Ureteral Calculi”[Mesh]), (“Kidney Calculi”[Mesh] AND “Ureteral Calculi”[Mesh]) AND “Coumarins”[Mesh], and (“Thrombocytopenia”[Mesh]) AND (“Kidney Calculi”[Mesh] OR “Ureteral Calculi”[Mesh]).
Reference lists of included studies were analyzed for suitable articles. Articles in languages other than English were included. Authors of the included studies were contacted whenever the data were not available or not clear.
Three reviewers (O.M.A., A.S., T.A.) identified all articles matching the inclusion criteria for full review. Each reviewer independently selected studies for inclusion in the review. Disagreement between them was resolved by consensus.
Data extraction and analysis
Studies reporting on the treatment of patients with a bleeding diathesis with both semirigid and flexible URS with or without laser lithotripsy were included. The authors assessed all patients having URS and not simply those with urolithiasis. Patients included were adults with a bleeding diathesis who had urinary stones. The following variables were extracted from each study: period and location of the study; all study population demographics; type of anticoagulant used or coagulopathy; pre or postop stent insertion; stone-free rates; and major and minor complications. The data of each study were grouped into excel tables to allow a numerical representation of the results.
Results
The literature search yielded 199 studies, of which 165 were excluded after abstract review. Thirty-four studies were then retrieved for further assessment with eight articles eventually included. One previously excluded study was included on closer interrogation; although the authors looked at various treatment modalities for stones, eight patients were ureteroscopically treated (six through Swiss LithoClast and two using the holmium laser). 9 The study is limited by the authors not providing specific demographic or coagulopathy data for these patients. The previous review process was unsuccessful in contacting the authors. 5 However, the outcomes of the intervention are relevant to this title. Thus, eight articles were included in the current review. 4,6,7,9 –13
Characteristics of the included studies
Seven of the eight included studies were retrospective, 4,6,7,9,11 –13 with one being a worldwide prospective study from Clinical Research Office of the Endourological Society database (Fig. 1). 10 All the included studies were published between 1998 and 2016 with the total number of participants with bleeding diatheses being 1109 with an age range of 18–97. Four studies were performed in the United States, two in Canada, and one a piece in Argentina and Austria.
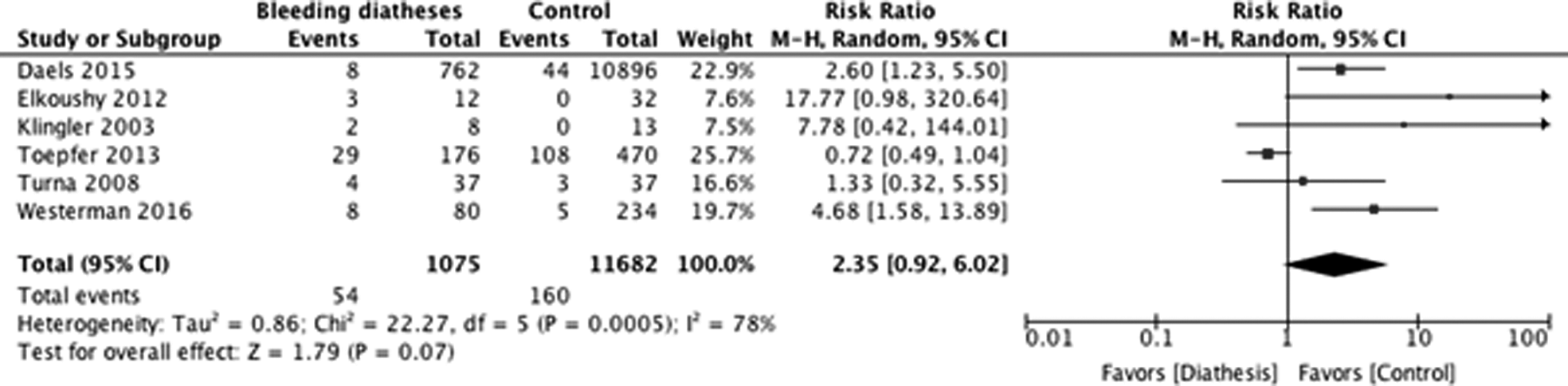
Pooled analysis of total complications.
Bleeding diatheses or anticoagulation or APT agent
Of 1109 participants, 643 underwent URS while on Aspirin, 153 on Warfarin, and 121 on Clopidogrel. Seven patients had thrombocytopenia, two von Willebrand disease, and three liver dysfunction. Other agents included tinzaparin (n = 1), dual agent therapy (n = 27), calcium carbasalate (n = 47), nadroparin (n = 33), and unknown (n = 77) (Table 1).
AC = anticoagulation; AF = atrial fibrillation; APT = activated partial thromboplastin; ASA = american society of anaesthesiologists; CBI = continuous bladder irrigation; DVT = deep vein thrombosis; ED = emergency department; INR = international normalized ratio; IVC = inferior vena cava; MI = myocardial infarction; NS = non-steroidal; PE = pulmonary embolism; UTI = urinary tract infection; VWD = von Willebrand disease; x = not reported.
Stone characteristics
For those articles which characterized stone burden, the range was 3–25 mm in diameter. Of those articles supplying mean stone burden, this was 11.9 mm, 7 6.8 mm, 9 and 13.2 mm, 12 giving an aggregate mean of 10.5 mm. Several articles had control arms where the aggregate mean of stone diameter was 10.1 mm. 7,11,12 Two articles performed statistical analysis on the size of stones between bleeding diathesis groups and control groups, one found no difference 12 and another found that the control group had significantly smaller stones (p = 0.01). 7 Stone density was not commented on in any of the included articles (Table 2).
FURS = flexible ureteroscopy; FURSL = flexible ureteroscopy and laser lithotripsy; NS = non-steroidal; URS = ureteroscopy; UTTCC = upper-tract transitional-cell carcinoma; x = not reported.
Procedure details
Of those included participants, 225 had flexible ureteroscopy (FURS) and laser stone fragmentation, 19 had URS and stone fragmentation, and 29 had diagnostic URS/FURS with the remaining 779 being unclear whether the patients received semirigid or FURS or both. An access sheath was used in 53% of procedures, and in the three articles assessing the outcome 62% of patients were pre-stented with 67%–100% of patients being stented post procedure. In two of three articles there was no significant change in Hemoglobin (Hb) 12,13 post procedure, but in one the Median postop Hb significantly decreased in anticoagulated patients vs controls (0.8 vs 0.2 g/dL; p = 0.001) (Table 2). 7
Stone-free rate
Overall stone-free rate across the seven articles which looked at this variable is 90.8% vs 86.2% in the control group (Table 2).
Complications
All articles reported complications as described below.
Major complications
There were two major complications in this series; Watterson and colleagues 6 reported one case of a large retroperitoneal hemorrhage in a patient who needed concomitant electrohydraulic lithotripsy for stone clearance. Another patient in the series by Elkoushy and coworkers required embolization 7 (Table 2).
Bleeding-related complications
There were 25 bleeding-related complications in the pooled cohort of patients. This represents a bleeding rate of 2.2%. Of these there were 4 cases of clot retention, 2 cases of clot colic requiring earlier removal of stents, and 16 cases of mild hematuria. There was one case of epistaxis and the above two mentioned cases of major hemorrhage (Table 2).
Intraoperative complications
There were no intraoperative complications in the bleeding diathesis group and one in the control group (proximal ureteral perforation) (Table 2).
Minor complications
There were 16 cases of urinary tract infection or sepsis (1.4%), 18 cases of poorly controlled pain (1.6%), and 1 case (0.09%) each of urinary retention and atrial fibrillation (Table 2).
Thromboembolic episodes
There was one case each of DVT 7 in the bleeding diathesis group in the control arm 12 (Table 2).
Pooled analysis of total complications
Meta-analysis of six articles with a control arm should prove that overall, there was no significant difference in complications between the bleeding diathesis group and control group (N = 12,757, p = 0.07, 95% confidence interval [CI] 0.92, 6.02, I2 = 78%) (Fig. 1).
Pooled analysis of bleeding-related complications
Pooled analysis for bleeding-related complications shows a statistically significant difference favoring the control arm (N = 12,757, p ≤ 0.0001, 95% CI 1.81, 5.73, I2 = 0%) (Fig. 2).
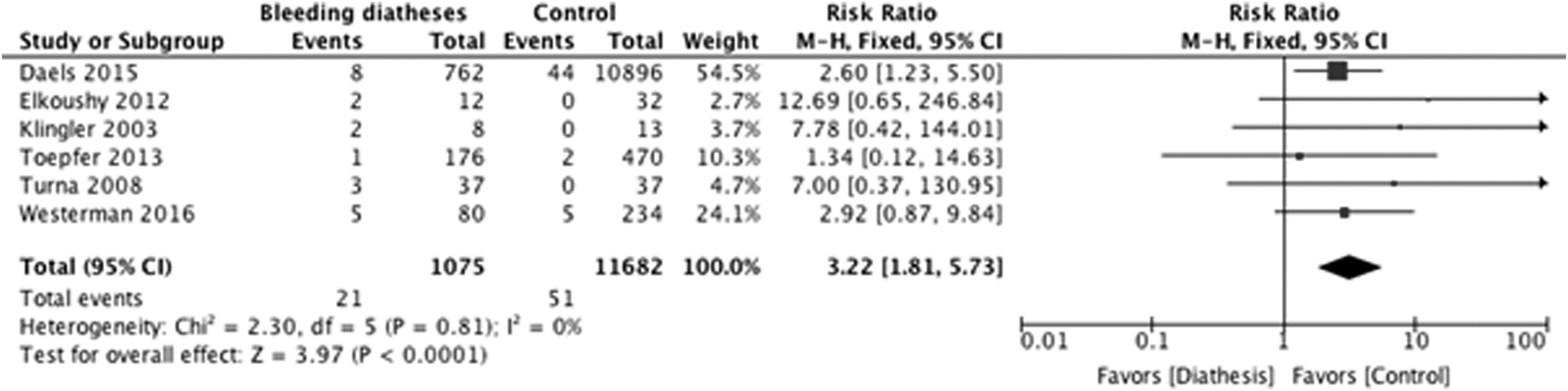
Pooled analysis of bleeding-related complications.
Pooled analysis of thrombosis events
Pooled analysis for thrombosis shows no statistically significant difference between the bleeding diathesis group and the control arm (N = 118, p = 0.67, 95% CI 0.23, 9.86, I2 = 48%) (Fig. 3).

Pooled analysis of thrombosis events.
Discussion
Findings of our study
This review has found that the use of URS in patients with anticoagulated or those on APT agents or who have bleeding diathesis is generally safe with comparable stone-free rates to matched controls. While meta-analysis shows no significant difference in overall complication rates, there is a significantly increased bleeding risk. Cumulative analysis shows that the risk of bleeding is more than five times that of controls (2.5% vs 0.42%). There is no difference in the risk of thrombosis.
Current practice
Normalizing coagulopathy before surgery is currently standard practice among surgeons. However, the risk of thromboembolic events during perioperative bridging with heparin is 1%–2%. 14 Furthermore, treating the coagulopathy is significantly more costly compared with patients without coagulopathy undergoing similar procedures; the average cost for URS in patients with bleeding diathesis in one unit in Austria is $4611 vs $2342 control. 9
Level of evidence and limitations of this review
Only one of the articles in this review is prospective, with the remaining seven being retrospective reports. Therefore, at most this review has a level 2a Levels of Evidence according to Centre for Evidence-Based Medicine. 15 Most of the articles are from single centers with small numbers of patients. A further limitation is the heterogeneity of study population; the majority of patients were on Aspirin with several studies providing insufficient detail on the nature of the bleeding diathesis. Whether such heterogeneity would impact outcomes is not known. All included studies may incur bias as recruitment of patients was from databases in seven of the eight included studies, possibly promoting selection and reporting bias. No studies were randomized. Despite these limitations, the aspiration of this study is to add weight to a previous review based on only 70 patients with a much larger study population of more than 11,000 cases.
Comparison of different studies
Since the previous systematic review on this topic in 2012, 5 several relevant studies have been published on this topic. Most recently, Westerman and associates retrospectively reviewed 4799 URS procedures, of which 314 were on APTs. The patients were divided into three groups: patients who held APT (234), patients who continued on a single APT (63), and patients who continued on dual APT (17). This review showed that there was no increased risk of bleeding in patients who continued APT; however, patients on dual therapy were more likely to be readmitted within 30 days of discharge than those who withheld APT or were on a single APT. 4
Daels and colleagues 10 conducted a prospective study which included 11,179 patients who underwent URS for nephrolithiasis. Seven hundred sixty-two of these patients had a coagulopathy; 426 patients were on aspirin, 94 were on clopidogrel, 47 were on acenocoumarol, 41 were on phenprocoumon, and 154 were on other anticoagulants, including calcium carbasalate and nadroparin. Forty-nine (7%) patients on anticoagulants suffered from complications with this group having the highest rate of complication compared with patients with diabetes (5.5%), cardiovascular disease (5%), and obesity (4.9%). Complications included bleeding in eight patients (1.1%). This study found that postoperative bleeding was significantly higher in patients on anticoagulants (1.1% vs 0.4%; p < 0.01) [8/762 vs 44/10,896]. They also found that patients with risk factors for stone formation had more complications than those without (4.9% vs 3.0%, p < 0.001). 10
Toepfer and coworkers 11 conducted a retrospective study comprising 646 patients, 176 of whom were on an anticoagulant. One hundred thirty-seven patients were on aspirin, 22 were on warfarin, and 17 were on clopidogrel. Eleven of the patients on warfarin were also on aspirin. These groups were compared with each other and to 470 patients who were not on anticoagulation. Stone sizes were similar between groups with the median size for the control group being 9 mm and for the anticoagulant group being 10.5 mm. Perioperative complications were uncommon, and the frequency was not statistically different among the groups. Of the patients on anticoagulation, 6.8% required repeat surgery compared with 7.2% in the control group. Patients on aspirin were more likely to be admitted within the first 30 days compared with all other groups. Clot retention occurred in only one patient on aspirin (0.56%) compared with two in the control group (0.4%). The study found no difference in bleeding complications among the groups. 11
Elkoushy and coworkers 7 performed a retrospective study, which included 12 patients on anticoagulation undergoing URS and nephrolithiasis. Six patients were on warfarin, three were on aspirin, one was on a combination of aspirin and clopidogrel, one on tinzaparin, and one patient who had cirrhosis with thrombocytopenia. They were compared with a control group of 32 patients. Nine patients underwent nephrolithiasis, and three patients had biopsies. The median stone size was 14 mm. Due to significant stone burden, two of the nine patients had a staged procedure. Therefore, 17 URSs were performed. Two patients developed significant postoperative hemorrhage with one requiring angioembolization. One other patient developed a DVT with pulmonary embolization. 7
The previous review on this topic had excluded an article by Klingler and associates. 9 On interrogation, it was felt suitable for inclusion. The authors found no complications in the control arm vs two patients in the anticoagulated group experiencing bleeding necessitating earlier removal of stents. 9
Recommendations and areas of future research
Overall, this article has added to the previous review by highlighting that the bleeding risk in this cohort of patients is higher than previously documented. While the overall risk of complications is equivalent between patients with bleeding diatheses and controls, the increase in bleeding risk is not insignificant (being fivefold). Fortunately, the vast majority of these events were not significant events with only one reported case of major hemorrhage in a cohort of 1109 patients (0.09%). Until further work is done in this area, a fair conclusion would corroborate that of Jóhann P. Ingimarsson cited in Urology news that the decision to continue anticoagulation or APT agents should be tailored to the patient's risk of a thromboembolic event vs the risk of bleeding associated with URS. 4,16 Indeed, the associated editorial by Brian Matalaga highlights that this trend will continue for the foreseeable future, particularly for those stone patients who must remain anticoagulated meaning they cannot receive PCNL or SWL thereby limiting their treatment options to URS. Matalaga highlights recommendations in the AUA Surgical Management of Stones guidelines, including steps which can be taken to reduce the risk of bleeding, reducing intrarenal pressure through use of an access sheath, nonpressurized irrigation, and bladder decompression with a Foley catheter if an access sheath is not utilized. 8,16
Conclusion
The use of URS with or without the holmium laser is generally a safe and efficient modality for treating patients with urolithiasis who also have a bleeding diathesis or are anticoagulated and or on APT agents. However, this updated review would suggest that in contrast to the previous review in this domain, the increased risk of procedure related bleeding is not insignificant and a patient-centered approach should be taken regarding continuing anticoagulation or APT agents or not correcting bleeding diatheses. While no intraoperative complications were reported in this cohort, higher quality ideally multicenter research is still required to inform future guidelines on this challenging group of patients.
Footnotes
Author's Contributions
A.S. performed literature search and data collection and wrote first draft. T.A. performed literature search, data collection, and meta-analysis and edited first and subsequent drafts. B.K.S. provided academic oversight and edited all drafts. O.M.A. commissioned the article, performed the systematic review of the literature, and edited all drafts. Members of EAU Young Academic Urologists—Endourology and Urolithiasis Working Group are O.M.A. and B.K.S.
Author Disclosure Statement
No competing financial interests exist.