
Abstract
Purpose:
To evaluate the efficacy and safety of increasing the energy dose in treating urinary lithiasis with extracorporeal lithotripsy through an expanded number of Shock Waves Per Session (SWPS).
Materials and Methods:
a randomized, prospective, and comparative study was performed with patients with renal or ureteral lithiasis from 2011 to 2014. Two groups were studied: Group A (n = 136), treated with 3500 SWPS, and Group B (n = 171), subjected to an expanded treatment with 7000 SWPS. Patients were considered stone free when there was no lithiasis or it were less or equal to 4 mm after treatment. Variables related to the patient, stones, treatment, and complications were collected.
Results:
The global SFR was 75.0% and 87.7% in Groups A and B, respectively (p = 0.004). In renal location, the SFR was higher in Group B (74.1% vs 90.7%, p = 0.003) regardless of the size. In the ureteral location, there were differences in the pelvic only (73.7% vs 95.2%). There were no differences in either the complication rate (27.2% vs 25.7%, p = 0.77), or the severity between the two groups. The variable “number of SWPS” was seen to be an independent predictor of the resolution of lithiasis, having the probability of resolving lithiasis 2.62 (CI 95% = 1.40–4.89) times greater when applying 7000 SWPS.
Conclusion:
In our study, increasing the energy dose applied through an expanded number of SWPS has been shown to be more effective than standard regimens with a similar safety profile. However, more clinical studies on different types of lithotripters are required to confirm these results.
Introduction
E
Despite the latest improvements in SWL 2 and the wide experience, there are only recommendations for specific features (energy, frequency, or intensity) for stone treatments. Actually there is as absence of evidence and more studies are needed to assess which is the best strategy for each treatment. 3,4 The number of shock waves applied during each treatment has not yet been standardized and there is no evidence linking safety to treatment plans that are currently recommended. 5 In fact, most of these recommendations come from commercial companies and are not supported by clinical trials.
The main objective of this study was to evaluate the efficacy and safety of increasing the energy dose in treating urinary lithiasis with extracorporeal lithotripsy through an expanded number of shock waves per session (SWPS).
Materials and Methods
Randomization
From January 2011 to December 2014, a total of 406 patients were included consecutively in a prospective and comparative study with randomized allocation. It was determined by a random sequencing selection obtained from a table of random numbers generated by EXCEL software©.
The inclusion criteria were patients older than 14 years diagnosed with radiopaque urinary lithiasis (renal or ureteral) with indication for extracorporeal lithotripsy according to European Association of Urology (EAU) guidelines. 5 All the patients included gave informed consent in writing after having had explained to them the alternative available treatments.
The exclusion criteria corresponded to the classic EAU guideline contraindications. 5 Patients without informed consent and information sheet, or those who have not done the recommended preliminary preparation, were also excluded.
A sample size calculation was performed, assuming a stone-free rate (SFR) with Group A of 70% and an expected rate of nearly 90% with Group B. The sample size for each group was 121 for each group (power > 80%) with a type I error rate < 0.05.
Group A received a standard treatment for a maximum of 3500 waves per session and Group B received an expanded treatment as much as a maximum of 7000 waves per session. After treatment, 307 patients were valid for analysis: 136 (33.5%) from Group A and 171 (42.1%) from Group B. Of all patients initially included, 91 (22.5%) were excluded for a violation of protocol or incomplete follow-up, asymmetrically affecting the sample (Fig. 1).
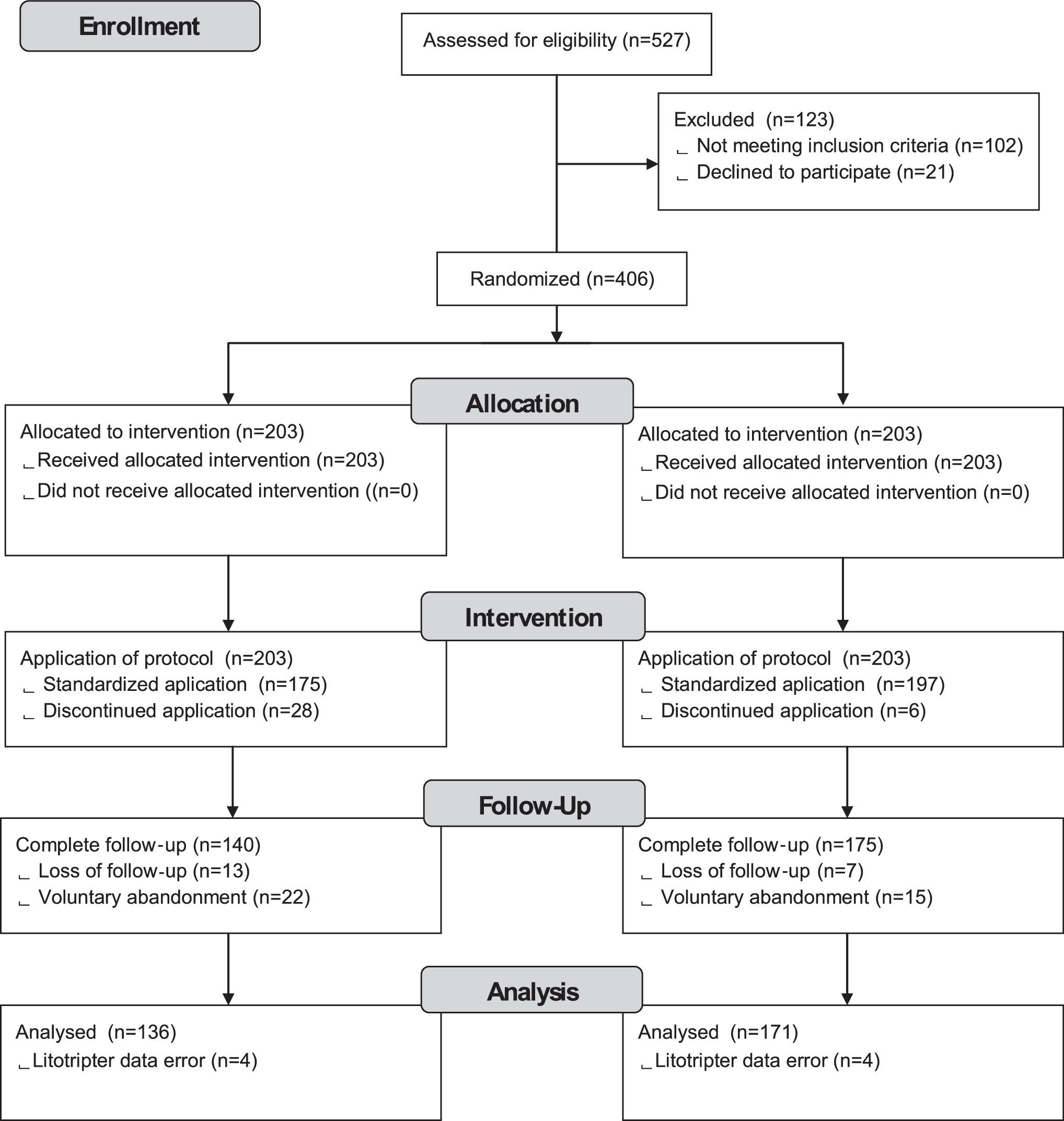
Flow diagram and patient disposition.
Variables referring to the patient, lithiasis, treatment, and complications were analyzed. The hardness of lithiasis was measured in HU when a CT had been performed as part of a previous study only. The patient pain was assessed through the visual analogic scale (VAS) (0–10) at the end of the session.
Technique
The treatment was performed on an outpatient basis under analgesia-sedation, strictly with the same protocol in each session. Four-hour fasting and adequate condition of the patient's hemostasis were mandatory. Urine culture was systematically requested before each procedure too. All patients received premedication intravenous (IV) ondansetron 4 mg, 20 mg of IV hydrochloride pethidine, and 1 g of IV paracetamol. New doses of pethidine were administered during the treatment on demand. Continuous monitoring of the patient throughout the treatment (blood pressure, heart rate, respiratory rate, and blood oxygen saturation, including electrocardiographic tracing) was performed. During the treatment, when blood pressure figures exceeded 165/95 mmHg, 10–50 mg IV urapidil was administered progressively until stabilization achieved.
The SWL treatment was performed using a third generation electromagnetic lithotripter (Siemens Lithoskop, shock wave system Pulse, Erlangen, Germany). The maximum focal width was 12 mm and the maximum penetration depth was 16 cm. Treatment was performed with the patient in supine position. For all cases, X-rays were used for stone localization during SWL treatment. The shock frequency was 120/min. The maximum intensity achieved was 4 kV for renal location and 6 kV for ureteral location, according to the manufacturer's recommendations.
The follow-up was completed a week after each session of extracorporeal lithotripsy; an X-ray of the urinary tract and a renal ultrasonography were undertaken to identify any delayed complications and consider the need for retreatment in the case of nonfragmentation or the presence of fragments not expelled.
Efficacy was evaluated according to the SFR, defined as the absence of lithiasis or nonsignificant fragments (less or equal to 4 mm) identified in the X-ray or non-contrast CT.
Statistics
For statistical analysis, the Chi-square test was used for the univariate analysis of qualitative variables, and Student t for quantitative variables. Binary logistic regression was the most appropriate statistical method chosen to determine the association between a set of predictor variables and a categorical response variable. Values of p < 0.05 were considered significant. Statistical analysis was performed with the statistical package SPSS 17.0.
Results
The descriptive and comparative analysis of the analyzed variables are detailed in Table 1. Both study groups were comparable in terms of age, gender, body mass index (BMI), pre-Double-J stent or nephrostomy, and of having a personal history of prior treatments for the resolution of lithiasis. Distribution side, location, hardness, and number of stones were also homogeneous among both groups, but not as to the stone size. The size was categorized into >1 cm or <1 cm; the sample analysis showed that the larger were found more frequently in Group B (p = 0.02), justified by the asymmetry of the rate of exclusion in both groups at the beginning of the study. The characteristics of the sessions of extracorporeal lithotripsy, which were applied to each group, are shown in Table 2.
IV = intravenous; VAS = visual analogic scale.
The global SFR was 75% in Group A (standard treatment) and 87.7% in Group B (p = 0. 004) (Table 3). A higher efficacy was found with the treatments in which more energy was applied (Group B) and being greater when the location of lithiasis was renal, regardless of its size.
Clinically insignificant residual fragments.
The multivariate analysis selected as predictor factors of success (SFR), stone size less than 1 cm, BMI less or equal to that of 25, and the treatment group to which the higher energy was applied (Group B). In this group, the probability of resolution of lithiasis was 2.621 (CI 95% 1.403–4.89) times greater (Table 4).
No statistically significant differences in terms of complications were found in either group (frequency and description detailed in Table 5). Two (1.47%) renal hematomas were detected in Group A (one (0.7%) was clinical and the other one subclinical (0.7%) and three (1.75%) in Group B, one (0.56%) of which required a selective embolization (Clavien III) and the other two (1.1%) were subclinical.
1 week after treatment.
Discussion
Since the first application of extracorporeal lithotripsy for the treatment of urolithiasis in 1980 by Chaussy in Munich, 6 successive generations of lithotripters have appeared on the market, with increasingly wider focal areas and greater power for fragmentation, each time offering improved safety profiles. 7,8 However, despite all the progress made in recent generations of lithotripters, none has improved the results of the initial prototype HM3. Hence, the search of treatment strategies that increase the clinical effectiveness, although maintaining a similar safety profile, is one of the current objectives of urologists who perform extracorporeal SWL.
There are a number of factors that have been shown to influence the efficiency of fragmentation. Several studies have reflected on the inversely proportional relationship between the distance of the shock wave generator and the lithiasis, and the rate of fragmentation. 9,10 On the other hand, a more intensive fluoroscopic monitoring during the session, a greater analgesic control, and an effective reduction of respiratory motion, all increase the proportion of waves that reach the focal point of the stone, hence increasing the total energy accumulated. 11 –13 The use of strategies of ramping, particularly in the renal location of lithiasis, has shown a decrease in the rate of renal hematomas attributable to the effect of renal vasoconstriction, which is produced by the procedure. 14,15 In addition, lower frequencies (60–90 waves/min) have shown greater effectiveness in the fragmentation. 16,17
However, despite extensive experience in the treatment of extracorporeal lithotripsy, the treatment is not universally standardized, particularly regarding the number of waves or maximum power to be applied during a treatment session. Currently, neither European nor American clinical guidelines make recommendations with respect to this. 5,18 Traditionally, the number of waves administered per session has been established generically by the recommendations of each manufacturer, despite having no scientific studies that support these recommendations. One of the few studies that tried to analyze the effect of the number of expanded shock waves was performed retrospectively by Hadj-Moussa and colleagues, 19 who did not find any difference in safety between cohorts of patients who received about 4000 shock waves between all sessions performed. Budía-Alba and colleagues 20 published a retrospective study aimed to assess the safety profile of a treatment strategy with a greater number of shock waves, demonstrating that neither the number of complications nor their severity increased. The results referred to in this article supported the theory that the increase of energy applied by applying a greater number of shock waves had no association with a parallel increase in complication rate. Therefore, to our knowledge, currently our work is the first prospective study that evaluates the effectiveness and safety when increasing the dose energy applied by increasing the number of SWPS in the treatment of urinary lithiasis with extracorporeal lithotripsy.
Our study has shown that the application of a higher energy dose per session by the increase in the number of waves has a good tolerance on the part of the patient; when the two study groups were compared, differences in neither the average power achieved during the treatment session, nor the final energy level administered, nor in the VAS were found to exist. Despite the scientific evidence recommending usage of a low pulse frequency rate to increase the effectiveness of treatment, 21,22 we decided establishing a frequency of 120 waves to be administered per minute to avoid an excessive duration of the treatment, which would have been impossible regarding patient tolerance. Since the two groups were treated with the same frequency of shock wave rates, this fact does not imply a bias in the comparative results between the two groups.
With regard to the standard treatment for urinary lithiasis, the increase of energy applied during an extracorporeal lithotripsy session has shown to increase the overall efficacy of the treatment. This was particularly evident when lithiasis was in the kidney, regardless of the size. In ureteral location, the greatest efficiency observed by applying a higher energy did not reach statistical significance. Despite it, when each portion of ureter was analyzed, statistical significance was achieved in the distal ureter. In addition, this study has shown that the amplification of shock waves applied to stones of less than 1 cm at the pelvic location may become the preferred technique, rather than other more invasive techniques such as the ureterorenoscopy, since it resolved 100% of cases compared to 70% in which standard treatment was applied. Also, a downward trend with respect to the number of sessions necessary to achieve resolution of the stone was observed in group B; specific studies should be carried out to analyze this hypothesis.
According our results, we think that the recommendations that are currently followed (mainly provided by the manufacturers of lithotripters) should be reviewed since they lack the necessary scientific support, and should be based on adequately tested energy criteria according to size and location.
The relatively low sample size of patients is one of the main limitations of the study, which does not allow analyzing the distribution of extremely rare events, such as the only Clavien III complication described, occurred in group B. However, no overall increase in complications has been demonstrated in group B; so it seems there is no increase in the complications of the expanded treatment. More clinical studies on different types of lithotripters are required to confirm these results.
The sample size also affects patients having lithiasis located in the iliac and pelvic ureter. The main reason being that of the patient's choice for an alternative technique to resolve their pathology, only those patients who accepted treatment of extracorporeal lithotripsy could be included in this study. This fact limits the possibility of a stratified analysis by ureteral sample size, although permitting it globally or in terms of its location. The confirmation of these results, with newly designed clinical trials to that effect, would be another step in the optimization of extracorporeal lithotripsy as a treatment for urinary lithiasis, both in its efficacy and the increasingly more relevant issue of cost-effectiveness. Despite this, we believe that this study provides a relevant addition to scientific literature, indicating the need to increase the energy applied to the stone during extracorporeal lithotripsy session. This increase improves its effectiveness without affecting the safety profile, nor requiring a change to the parameters of the recommendations given regarding the limitations in the application of this treatment. The parameter that should be used is the total energy dose applied per session and not the total number of shock waves applied, allowing for comparisons to be made between different lithotripters with the same energy source.
Conclusion
In our study, increasing the energy dose applied through an expanded number of SWPS has been shown to be more effective than standard regimens with a similar safety profile. However, more clinical studies on different types of lithotripters are required to confirm these results.
Footnotes
Author Disclosure Statement
No competing financial interests exist.