
Abstract
Introduction:
To analyze the most recent temporal trends in the adoption of urologic laparoendoscopic single-site (LESS), to identify the perceived limitations associated with its decline, and to determine factors that might revive the role of LESS in the field of minimally invasive urologic surgery.
Materials and Methods:
A 15 question survey was created and sent to members of the Endourological Society in September 2016. Only members who performed LESS procedures in practice were asked to respond.
Results:
In total, 106 urologists responded to the survey. Most of the respondents were from the United States (35%) and worked in an academic hospital (84.9%). Standard LESS was the most popular approach (78.1%), while 14.3% used robotics, and 7.6% used both. 2009 marked the most popular year to perform the initial (27.6%) and the majority (20%) of LESS procedures. The most common LESS procedure was a radical/simple nephrectomy (51%) followed by pyeloplasty (17.3%). In the past 12 months, 60% of respondents had performed no LESS procedures. Compared to conventional laparoscopy, respondents only believed cosmesis to be better, however, this enthusiasm waned over time. Worsening shifts in enthusiasm for LESS also occurred with patient desire, marketability, cost, safety, and robotic adaptability. The highest rated factor to help LESS regain popularity was a new robotic platform.
Conclusion:
The decline of LESS is apparent, with few urologists continuing to perform procedures attributed to multiple factors. The availability of a purpose-built robotic platform and better instrumentation might translate into a renewed future interest of LESS.
Introduction
T
Over these past few years the enthusiasm for LESS has declined. The aim of this study was to analyze the most recent temporal trends in the adoption of urologic LESS, to identify the perceived limitations associated with its decline, and to determine factors that might revive the role of LESS in the field of minimally invasive urologic surgery.
Materials and Methods
A survey invitation containing a link for anonymous participation was sent to all Endourological Society members in September 2016. The distribution list consisted of 2800 e-mail addresses, but only members who performed LESS procedures in practice were asked to respond. The completed survey served as the consent to participate in the research study. No compensation was provided to participate in the study. A 2-month window to complete the survey was provided.
The survey consisted of 15 questions (Supplementary Data S1; Supplementary Data are available online at
Results
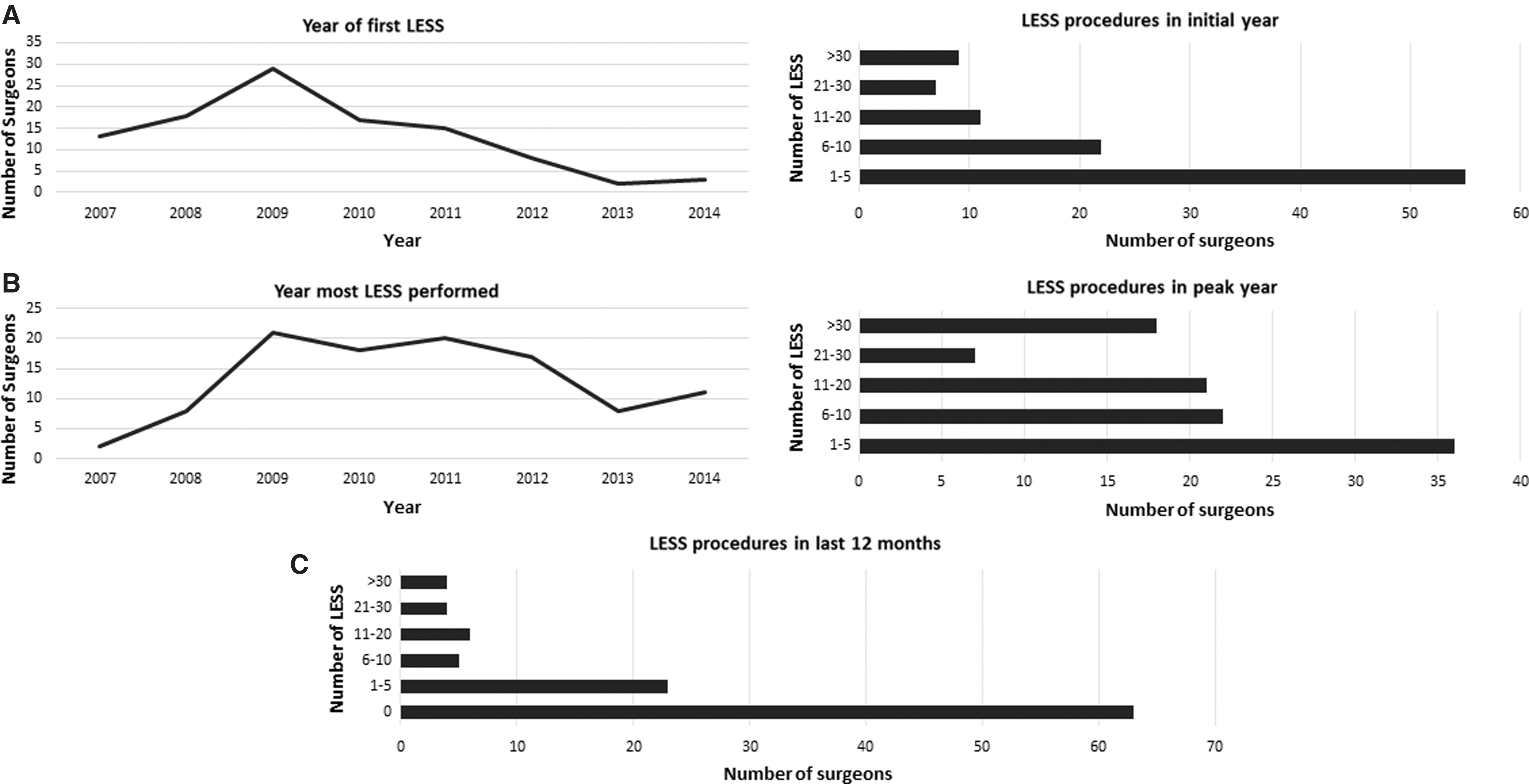
In total, 106 urologists responded to the survey spanning at least 26 countries, with the United States (35%) having the greatest representation as shown in Figure 1. Most surgeons worked in an academic hospital (84.9%). Standard LESS was the most popular approach (78.1%), while 14.3% used RLESS and 7.6% used both. Overall, 2009 marked the most popular year to perform the initial and the majority of LESS procedures, 27.6% and 20%, respectively. Number of surgeons performing LESS suddenly declined in 2013. Five or less cases represented the most popular number of LESS performed in the initial and peak year. Only 17.3% of surgeons performed >30 LESS cases in their peak year. When asked approximately how many LESS procedures have you performed in the past 12 months, 63 (60%) urologists stated none (Fig. 2C). Only 18.1% performed >5 LESS cases in the last 12 months. Surgeons who completed their first LESS case in or after 2009 were more likely to perform >5 LESS cases in the last 12 months compared to surgeons who completed their first LESS case before 2009 (22.7% vs 6.5%, p < 0.048).
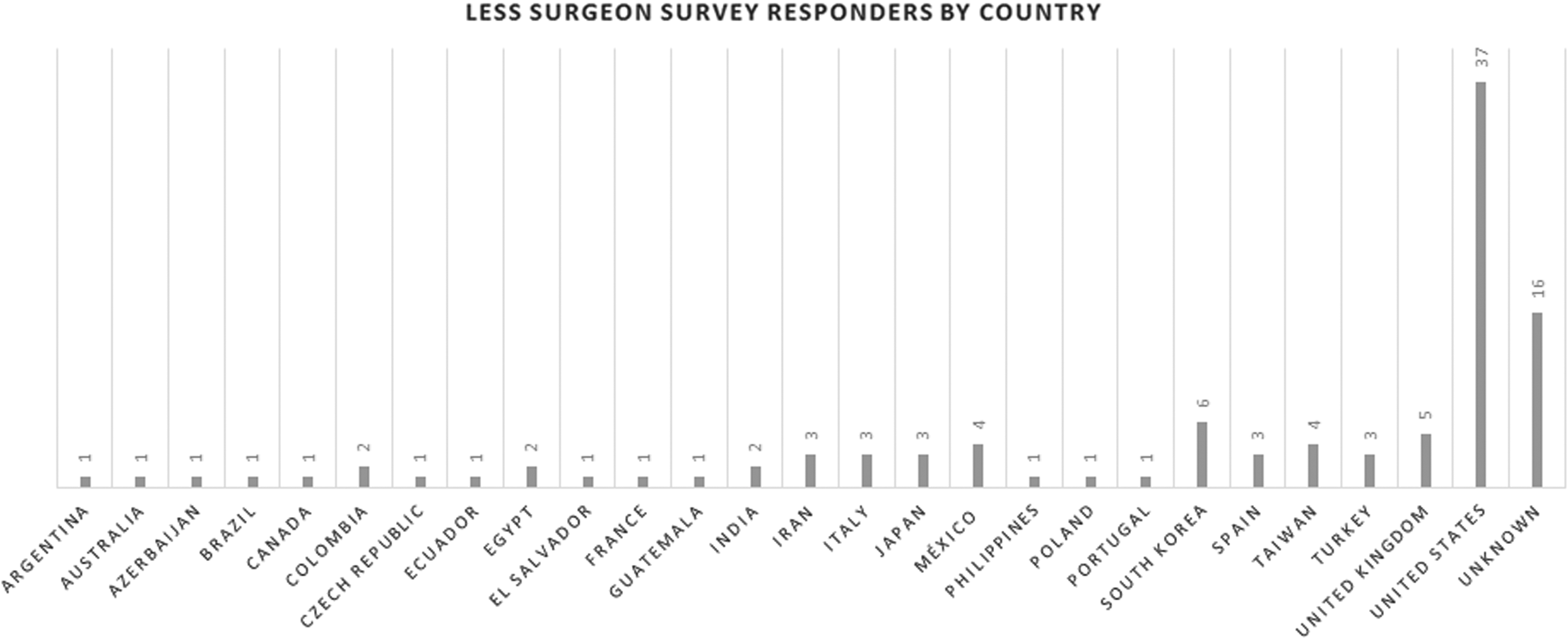
Survey responders by country.
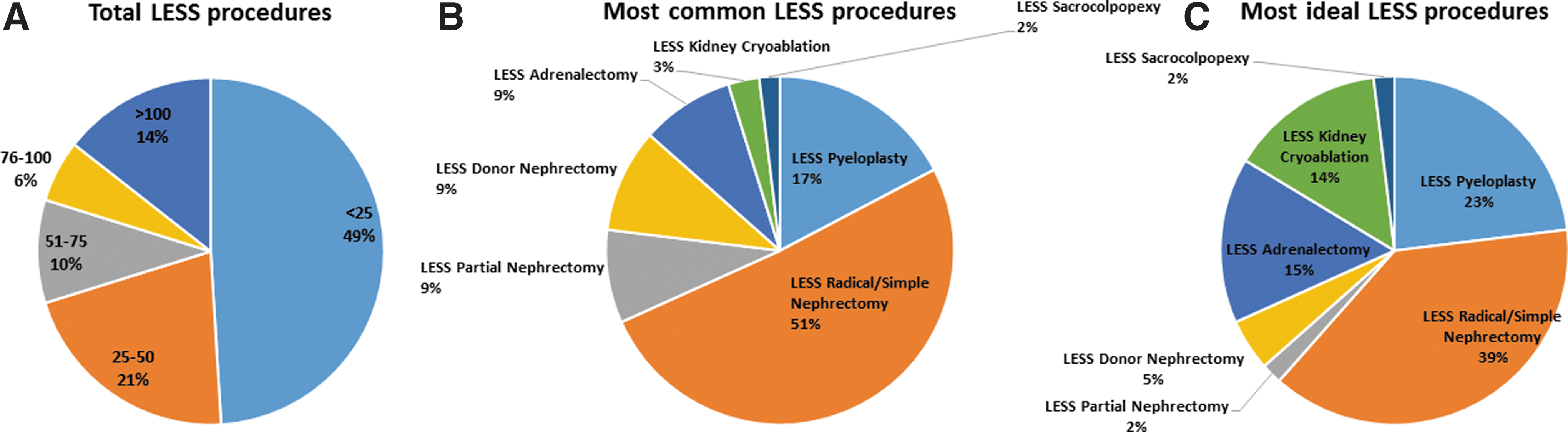
Overall, the majority of surgeons (49%) performed <25 LESS procedures throughout their career (Fig. 3A). The most common LESS procedure was a radical/simple nephrectomy at 51% followed by pyeloplasty at 17% (Fig. 3B). These were also rated as the most ideal LESS procedures at 39% and 23%, respectively (Fig. 3C). The least popular LESS procedure was sacrocolpopexy (1.9%).
The most popular open-ended responses for initial enthusiasm for LESS included cosmesis, novelty, marketing, faster recovery, keeping up with other surgeons, and scientific interest. When asked to compare LESS to conventional laparoscopy, only cosmesis was deemed to be better. Over time, 82% more urologists deemed LESS no different than laparoscopy for cosmesis, and 26% fewer urologists felt LESS was better than laparoscopy (Fig. 4). Worsening shifts in enthusiasm for LESS also occurred with patient desire, marketability, cost, safety, and robotic adaptability. Changes in opinion from LESS being worse to LESS being no different or better occurred with visualization, learning curve, operating room (OR) time, applicability to urologic procedures, range of motion, instrumentation, ergonomics, and suturing. A subset analysis comparing the highest and lowest volume surgeons did not reveal any significant differences in attitudes toward LESS.

Comparison of initial vs current opinions on less vs conventional laparoscopy. C = current; I = initial; OR = operating room; ROM = range of motion.
Factors rated the highest to help LESS gain popularity (Fig. 5) included a new robotic platform (4.25/5), instrument modifications (4.03/5), and improved suturing (3.97/5). Decreased operative steps was the least important factor thought to improve LESS (2.99/5)
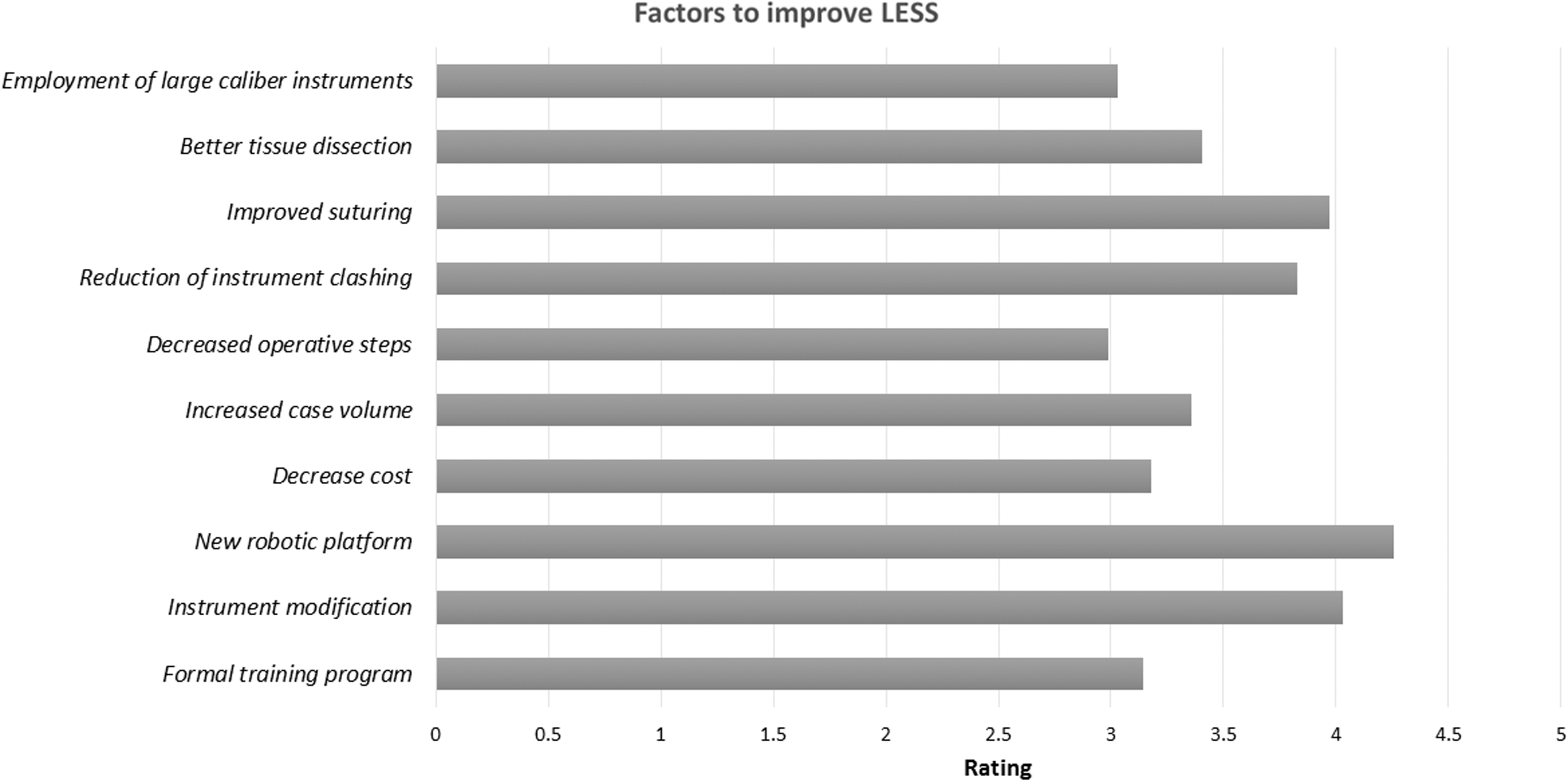
Evaluation of factors thought to improve LESS.
Discussion
The peak of LESS for the majority of urologic surgeons occurred in 2009. LESS cases were steady until 2013 when a sharp decline occurred. Only 40% of the survey responders performed any LESS procedures in the last 12 months. Looking closer at the data, even in the peak year, the majority of surgeons only performed five or fewer LESS procedures. This is likely one of the factors leading to the decline of LESS as surgeons are not performing enough cases to overcome the steep learning curve. Furthermore, it appears that the majority of the pioneer surgeons of LESS have become disenchanted with the procedure and are currently only performing a minimal number of cases.
A Scopus® search for documents published on “laparoendoscopic single site surgery” revealed a similar trend in the literature that we found from our survey (Fig. 6). The leading years for LESS publications were 2011 and 2012, which coincides with the years prior when the majority of the cases were performed. Interestingly, a steep drop in publications occurred between 2011 and 2016 driven by the precipitous decline from the United States. It appears that the geographic distribution of LESS cases has shifted. A multicenter experience of 469 cases was recently reported in Japan making it the second largest analysis of various urologic LESS surgeries. 6 Additionally, Pavan and colleagues 7 recently reported on minimally invasive adrenalectomy and found centers from Asia and South America to have the highest rates of LESS adrenalectomy procedures. While the obesity epidemic is prevalent worldwide, the highest rates occur in the United States 8 and patient demand for LESS is likely affected. With lower obesity rates in other parts of the world, patient demand and focus on cosmetic outcomes may play a bigger role in these countries.
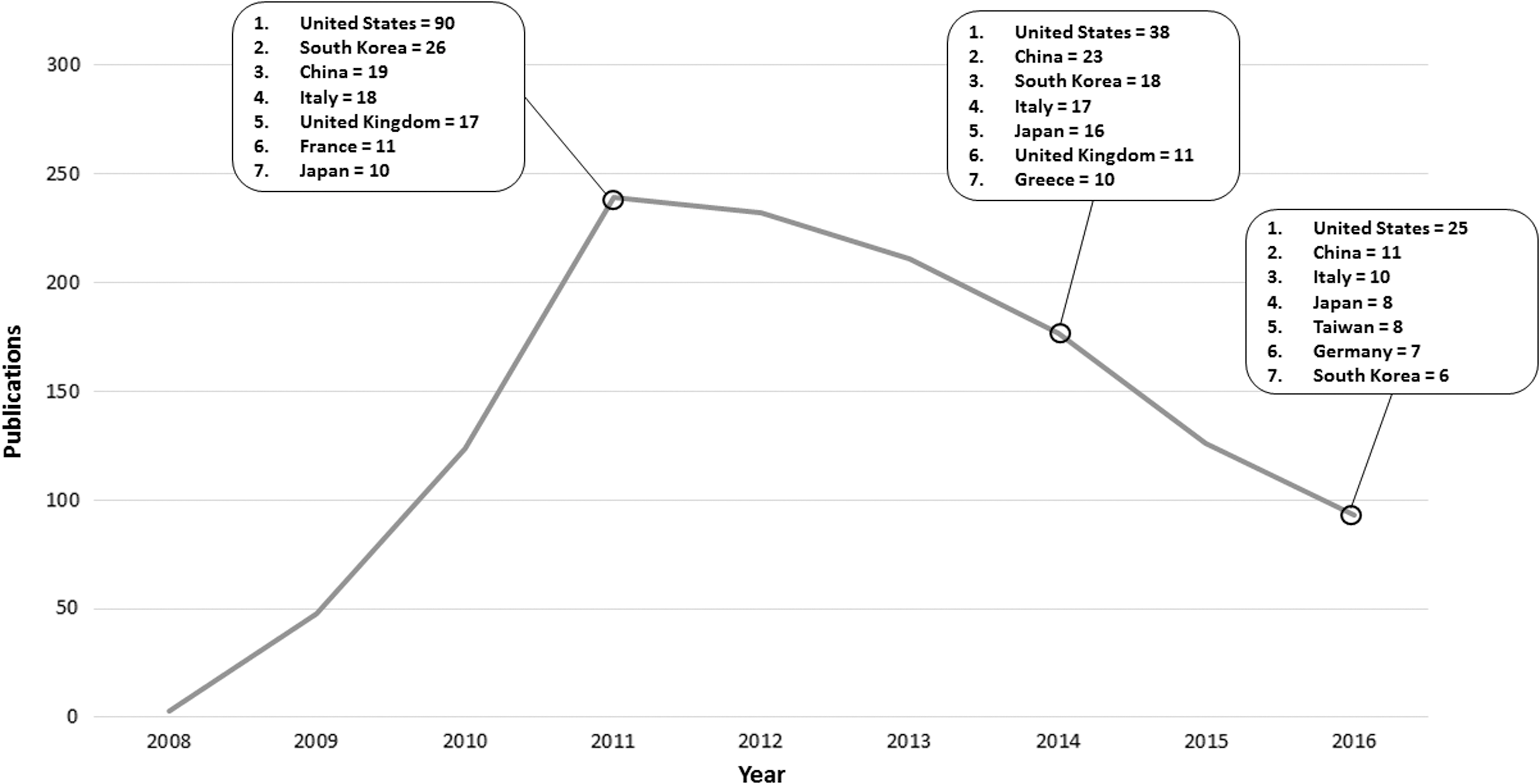
Scopus® search of LESS publications from 2008 to 2016 with top 7 countries of origin.
The most common LESS procedure performed according to our survey was a radical/simple nephrectomy. Pyeloplasty, a highly ideal procedure for LESS, was only rated 17% most common likely given the difficulty with LESS suturing. LESS donor nephrectomy (DN) represented the next frontier in minimally invasive surgery to further reduce morbidity, which would be highly advantageous in the field of living donation. Survey responders did not believe this was a very ideal procedure and was voted only slightly better than partial nephrectomy and sacrocolpopexy. A meta-analysis on LESS vs laparoscopic DN concluded that LESS DN offers comparable surgical and early functional outcomes with a lower analgesic requirement. 9 However, this procedure was thought to be more technically challenging shown by a greater likelihood of conversion. Aull and colleagues 10 performed a randomized prospective study on LESS DN (n = 49) vs laparoscopic DN (n = 51). Satisfaction scores were similar between the two groups in addition to recovery and recipient outcomes. Again, conversion rate was higher for LESS DN representing the technical demands of this procedure and the barrier to widespread adoption.
There have been several comparative series through the years between LESS and conventional laparoscopy. A critical analysis of the literature described several procedures such as simple and radical nephrectomy, pyeloplasty, adrenalectomy, simple nephrectomy, sacrocolpopexy, and kidney cryoablation. 4 The studies were all limited by retrospective data, small numbers, nonrandomized designs, and lack of standardization in postoperative outcomes. The authors concluded that these studies showed noninferiority of LESS over conventional laparoscopy with encouraging trend toward less pain and better cosmesis. This certainly adds to the results of our survey on the decline of LESS. There is a dearth of new surgeons attempting LESS and it is hard to fault them in adopting new technology that shows no superiority over an established minimally invasive approach. On the other hand, the robotic approach has seen increases in usage given its advantages over laparoscopy in partial nephrectomy, 11 pyeloplasty, 12 and prostatectomy 13 among others. Furthermore, the ability to transition from open to robotics without prior laparoscopic experience is a big incentive for novice surgeons. Even with extensive laparoscopic experience, urologists experienced with LESS will attest to the steep learning curve and difficulty with suturing.
Enthusiasm declined in areas surgeons thought initially to be better in LESS but turned out to be no different or worse. Improved cosmesis was a major driving force to adopt the technique. Conceptually, a single periumbilical incision has a better cosmetic result than three or four extraumbilical incisions required for conventional laparoscopy. Patients objectively thought this was the case as well in a survey conducted by Olweny and colleagues 14 comparing attitudes toward cosmesis before and after surgery in LESS vs laparoscopic/robotics vs open kidney surgery. They showed the median score for “size/number of scars” was significantly higher for the LESS cohort before surgery, but there was no significant difference among cohorts after surgery. Similarly, our survey showed that surgeons believed cosmesis would be far better in LESS, however, the largest decline in enthusiasm in our study occurred in the cosmesis category after surgeons performed more operations. This change in surgeon attitude may be a reaction to how patients perceive their cosmetic results postoperatively. Another important category where enthusiasm declined was patient desire. It appears that patients are more concerned with surgeon reputation, efficacy, and safety. 14,15
A new robotic platform that can improve suturing and adopt better instruments is perhaps the answer to revive LESS. The current platform, which was not designed for single-site use, suffers from the limited range of motion of the robotic instruments, loss of pneumoperitoneum, limitation of surgical assistance, and inability to use the fourth arm. 5 Development of the da Vinci VeSPA (Intuitive Surgical, Sunnyvale, CA) robotic surgical instruments with a new multichannel port was thought to improve some of the technical issues in a porcine model. 16 However, in practice the new instruments made suturing more difficult, with persistent issues relating to external collisions and restriction of assistant's motions still exist. 17 Further, loss of pneumoperitoneum is a problem with the VeSPA and novel devices such as the AirSeal® to counter this cannot be incorporated into this single-site port. The current da Vinci system for RLESS is not ideal given its existing configuration of robotic arms and bulkiness. 17 The most recent addition for RLESS is a purpose-built da Vinci model SP1098 single-port robotic platform for extraperitoneal surgery. Limited experience in cadavers using the system for a perineal prostatectomy, partial nephrectomy, and radical nephrectomy have shown promising results while preserving triangulation and eliminating clashing. 18 While this is optimistic, clinical evaluation in humans is needed.
There are multiple limitations to our survey study worth mentioning. The survey was only sent to members of the Endourological Society and therefore some LESS surgeons may have not been included. Additionally, the survey was only available in the English language and could have hampered the survey response rate from other countries. Further, most of the answer choices were prefilled multiple choice questions and little room for open responses was available. This was an attempt to keep response rates high and keep time to complete the survey minimal. In addition, given the historical questions asked, there is the potential for recall bias. The benefit of our survey is that it is the most current evaluation on the status of LESS. Furthermore, we were able to objectively demonstrate the decline in LESS and the attitudes among surgeons to accompany the decline.
Conclusions
The decline of LESS surgery is apparent. Although there were many early adopters, fewer surgeons continued to perform a high volume case load. Subsequently, in the last 12 months, most survey responders performed no LESS procedures. Enthusiasm over time for cosmesis, patient desire, marketability, cost, safety, and robotic adaptability in LESS saw declines. The availability of a purpose-built robotic platform and better instrumentation overcoming current ergonomic challenges might translate into a renewed future interest of LESS.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.