
Abstract
Background and Objective:
Robot-assisted radical prostatectomy (RARP) has become the preferred surgical treatment for localized prostate cancer in the United States. Little is reported about the association between predischarge outcomes and postdischarge outcomes following RARP. The objective of this study was to explore the predischarge predictors of readmissions and postdischarge complications in RARP.
Materials and Methods:
The National Surgery Quality Improvement Program (NSQIP) database was used to identify prostate cancer patients who underwent elective RARP from 2012 to 2014. Multivariable logistic regression was performed to assess potential predischarge predictors of readmissions and NSQIP-defined postdischarge complications within 30 days of RARP. To test the robustness of primary analysis, a secondary multivariable logistic regression was performed in the cohort of patients without any NSQIP-defined predischarge complications.
Results:
A total of 9975 patients were included. The readmission rate in the cohort was 3.3% (n = 332), and 4.4% (n = 441) had at least one complication. Multivariable logistic regression showed that American Society of Anesthesiologists (ASA) score of 3–4 (odds ratio [OR] = 1.27, 95% confidence interval [CI] = 1.00–1.62, p = 0.050), increasing operative time (OT, per minute) (OR = 1.002, 95% CI = 1.000–1.003, p = 0.012), increasing length of hospital stay (LOS, per day) (OR = 1.36, 95% CI = 1.23–1.49, p < 0.001), and predischarge complication (OR = 2.15, 95% CI = 1.27–3.65, p = 0.004) were associated with readmission. Increasing OT (OR = 1.002, 95% CI = 1.001–1.004, p = 0.002) and increasing LOS (OR = 1.16, 95% CI = 1.02–1.30, p = 0.020) were associated with postdischarge complications. Logistic regression in patients without predischarge complications (n = 9804) confirmed that ASA score of 3–4 (OR = 1.37, 95% CI = 1.07–1.75, p = 0.013), increasing OT (OR = 1.002, 95% CI = 1.000–1.003, p = 0.022), and increasing LOS (OR = 1.34, 95% CI = 1.21–1.49, p < 0.001) were associated with readmissions. Secondary analyses also confirmed that increasing OT (OR = 1.002, 95% CI = 1.001–1.004, p = 0.002) and increasing LOS (OR = 1.18, 95% CI = 1.04–1.34, p = 0.011) were associated with postdischarge complications.
Conclusions:
Predischarge complications, OT, and LOS are associated with readmissions and postdischarge complications after RARP. It may be possible to identify patients at a higher risk of postdischarge adverse events to direct prevention interventions. Further prospective studies are needed to validate our findings.
Introduction
P
In recent years, readmission after surgical discharge has been the subject of ever-increasing scrutiny and has become a research focus in various surgical specialties. 4 –9 Readmissions can contribute to increased healthcare costs and may be a surrogate for more severe postdischarge adverse events. Another important surgical outcome that is closely associated with readmission is postdischarge complications. 5 Identifying predictive factors for readmission and postdischarge complications may provide valuable information, which helps to target readmission prevention interventions to high-risk patients after discharge. 9 There is a paucity of information that specifically focuses on readmissions and postdischarge complications after RARP. 10,11 Also, limited data exist regarding the association between predischarge surgical outcomes (predischarge complication, operative time [OT], and length of hospital stay [LOS]) and postdischarge outcomes (readmission and postdischarge complication) after RARP.
To address this knowledge gap, we analyzed the data from the American College of Surgeons National Surgery Quality Improvement Program (ACS-NSQIP), a large, nationally representative risk-adjusted surgical outcomes registry. We summarized causes of readmissions and the distribution of pre/postdischarge complications after RARP. Then, we aimed to investigate potential predischarge predictors of readmissions and postdischarge complications in RARP.
Materials and Methods
Data source
Data of current study were derived from the ACS-NSQIP Participant Use Data Files (PUFs) (2012–2014). ACS-NSQIP prospectively maintains a national database of patients undergoing various surgical procedures in the United States. ACS-NSQIP PUF provides data regarding the postoperative 30-day morbidity and mortality outcomes. Detailed information about the ACS-NSQIP PUF, including variables and their definitions, can be found at the official website and user guide file. 12 This study used deidentified data and institutional review board approval was not required.
Study cohort
Only patients who underwent RARP (Current Procedural Terminology [CPT] code 55866) and had a postoperative diagnosis of prostate cancer (International Classification of Diseases, 9th edition [ICD-9] code 185) were included. Then, any cases with other procedures or concurrent procedures not relevant to RARP were excluded. To restrict heterogeneity of our study cohort, we only considered laparoscopic bilateral pelvic lymph node dissection (PLND) (CPT code 38571) as relevant to RARP. However, the extent of lymph node dissection was not available in the NSQIP. Considering the objectives of our study, we only included patients who were admitted from home and discharged to home. 9 Additional exclusion criteria were as follows: disseminated cancer, preoperative hospitalization, preoperative sepsis, preoperative transfusion, OT <60 minutes (potential coding error), and cases with missing values on covariables and outcomes. NSQIP counts 30-day readmissions and complications starting from the day of operation; so, to limit the immortal time bias and to allow for most of the 30-day readmissions and postdischarge complications to accrue, we also excluded patients with a LOS >7 days. 9,13
Variables
For each patient, age, body mass index (BMI), race (white vs other), year of surgery, current smoking status, American Society of Anesthesiologists (ASA) score, steroid usage, dyspnea, weight loss, on dialysis, history of hypertension, diabetes mellitus, chronic obstructive pulmonary disease, and bleeding disorders were collected. PLND, OT, LOS, and predischarge complications were collected and considered as factors of interest.
Outcomes of interest
Primary outcomes of interests were NSQIP-defined readmissions and postdischarge complications within 30 days after RARP. In NSQIP, the readmission was classified as an “inpatient” stay by the readmitting hospital or reported by the patient/family as such. “Any readmission” was defined as any readmission (to the same or another hospital) for any reason within 30 days of the principal surgical procedure, and “unplanned readmission” was defined as unplanned readmission at the time of the principal procedure. “Unplanned readmissions” were categorized into two main groups based on that if the “unplanned readmission” was likely related to the principal operating procedure or not. Suspected causes of “unplanned readmissions” were captured and causes could be categorized into three entities: (1) NSQIP-coded reason (NSQIP-defined complication); (2) ICD-9 coded reason (an adverse event that could not be categorized into NSQIP-defined complication or adverse event that did not meet the criteria of NSQIP-defined complication); and (3) no reason recorded.
Individual NSQIP-defined 30-day complications were categorized into pre- and postdischarge complications based on the time interval (vs LOS) between RARP and the event. Then pre- and postdischarge complications were grouped as previously reported 14 : wound (superficial, deep, and organ space surgical site infections, as well as wound dehiscence), pulmonary (pneumonia, reintubation, and ventilator support >48 hours), renal (acute renal failure and progressive renal insufficiency), neurologic (cerebrovascular accident/stroke with neurologic deficit), cardiac (cardiac arrest and myocardial infarction), thromboembolic (deep venous thrombosis and pulmonary embolism), septic (sepsis and septic shock), urinary tract infection (UTI), and transfusion. We also considered reoperation as a separate complication event. Overall (pre/postdischarge) complication was defined as the occurrence of any (pre/postdischarge) complication.
Statistical analyses
Baseline patient and perioperative characteristics were described and compared between patients with readmissions and without readmissions. Data were reported as frequencies (percentages) and medians (interquartile ranges [IQRs]) for categorical and continuous variables, respectively. Categorical variables were compared using Fisher's exact test and continuous variables using Mann–Whitney U-test. Multivariable logistic regression adjusted for the covariables was performed to assess potential predischarge predictors of readmissions and postdischarge complications in the overall cohort. To test the robustness of our primary analysis, a secondary multivariable logistic regression was performed in the cohort of patients without any NSQIP-defined predischarge complications. All tests were two-sided, and a p-value of <0.05 was considered statistically significant. All analyses were performed using STATA 14 (StataCorp LP, College Station, TX).
Results
Patient and perioperative characteristics
After exclusion, a total of 9975 patients were included in the final cohort. Baseline patient and perioperative characteristics are presented in Table 1. The median age of the overall cohort was 62 years (IQR = 57–67) and the median BMI was 29.1 kg/m2 (IQR = 25.5–34.0). Most patients were white (n = 8572, 86.0%). The median OT was 195 minutes (IQR = 158–237); 5958 (59.7%) cases had OT ≥181 minutes; and 2357 (23.6%) had OT ≥241 minutes. A total of 3057 (30.6%) cases had LOS ≥2 days, and median LOS was 1 day (IQR = 1–2). A total of 171 (1.7%) patients had at least one NSQIP-defined predischarge complication.
ASA = American Society of Anesthesiologists; BMI = body mass index; COPD = chronic obstructive pulmonary disease; DM = diabetes mellitus; HTN = hypertension; IQR = interquartile range; LOS = length of hospital stay; OT = operative time; PLND = pelvic lymph node dissection.
Postdischarge complications and readmissions
A total of 441 (4.4%) patients had at least one NSQIP-defined complication and 280 (2.8%) patients had at least one postdischarge complication in the overall cohort. Distribution of the complications (pre- vs postdischarge) are shown in Figure 1. Among all the patients with complications (n = 441), 161 (36.5%) patients had only predischarge complications, 270 (61.2%) patients had only postdischarge complications, and 10 (2.3%) patients experienced both pre- and postdischarge complications. Only transfusion (98.3% vs 0%) and renal complications (55.0% vs 45.0%) had more predischarge events than postdischarge events. Septic, wound, thromboembolic complications, as well as UTI, occurred predominantly after discharge.
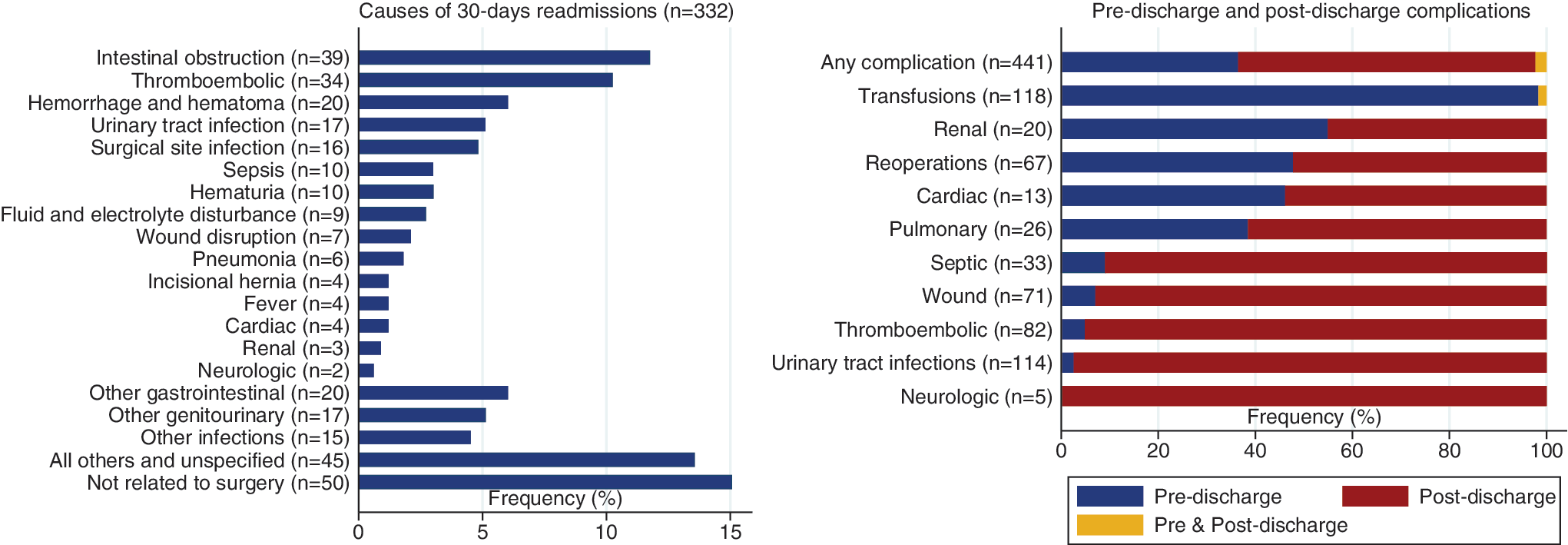
Causes of readmissions and distribution of pre/postdischarge complications.
A total of 332 (3.2%) patients were readmitted in the overall cohort. Among all the patients who had readmissions, 145 (43.7%) patients had postdischarge NSQIP-defined complications. Patients with postdischarge complications had significantly more readmissions than patients without any postdischarge complications (51.8% vs 1.9%, p < 0.001). Only one (0.3%) readmission in the cohort was designated as “planned.” Among the 331 patients with unplanned readmission, 282 (85.2%) patients were reported to have readmissions related to RARP, and 49 (14.8%) were reported to have readmissions not related to RARP. Causes of all the readmissions are summarized in Figure 1. Three most common reasons for readmissions were intestinal obstruction (n = 39, 11.7%), thromboembolic events (n = 34, 10.2%), and hemorrhage/hematoma (n = 20, 6.0%).
Figure 2 shows the time-to-event distributions of readmissions and individual postdischarge complications with 10 or more events. Median time from RARP to readmission was 7 days (IQR = 4–14), and median time from RARP to postdischarge UTI was 16 days (10–23).

Time-to-event distributions of readmissions and individual postdischarge complications. DVT = deep venous thrombosis; IQR = interquartile range; PE = pulmonary embolism; SSI = surgical site infection; UTI = urinary tract infection.
Multivariable adjusted analyses
Multivariable logistic regressions for readmissions and postdischarge complications in the overall cohort (n = 9975) are shown in Table 2. Increasing OT (per 1 minute) (odds ratio [OR] = 1.002, 95% confidence interval [CI] = 1.000–1.003, p = 0.012), increasing LOS (per 1 day) (OR = 1.36, 95% CI = 1.23–1.49, p < 0.001), and predischarge complications (OR = 2.15, 95% CI = 1.27–3.65, p = 0.004) were found to be associated with readmissions. Another factor associated with readmission was ASA score 3–4 (OR = 1.27, 95% CI = 1.00–1.62, p = 0.050). Increasing OT (OR = 1.002, 95% CI = 1.001–1.004, p = 0.002) and increasing LOS (OR = 1.16, 95% CI = 1.02–1.30, p = 0.020) were associated with postdischarge complications. Other factors associated with postdischarge complications included increasing BMI (per 1 kg/m2) (OR = 1.03, 95% CI = 1.01–1.06, p = 0.016) and preoperative bleeding disorder (OR = 2.78, 95% CI = 1.37–5.63, p = 0.005).
Statistically significant results are shown in bold.
CI = confidence interval; OR = odds ratio.
Secondary multivariable logistic regressions in the cohort (n = 9804) of patients without any predischarge complications are shown in Table 3. The results still demonstrated that ASA score of 3–4 (OR = 1.37, 95% CI = 1.07–1.75, p = 0.013), increasing OT (OR = 1.002, 95% CI = 1.000–1.003, p = 0.022), and increasing LOS (OR = 1.34, 95% CI = 1.21–1.49, p < 0.001) were associated with readmissions. The results also confirmed that increasing OT (OR = 1.002, 95% CI = 1.001–1.004, p = 0.002) and increasing LOS (OR = 1.18, 95% CI = 1.04–1.34, p = 0.011) were associated with postdischarge complications.
Statistically significant results are shown in bold.
Discussion
Main findings
In this contemporary NSQIP (2012–2014) study, we comprehensively reported the incidences, causes, and predischarge risk factors of readmissions and postdischarge complications after RARP. Our analysis of data from 9975 patients showed that predischarge surgical outcomes, including predischarge complication, OT, and LOS were significantly associated with readmissions and postdischarge complications.
Comparison with previous studies
Two prior studies have reported the risk factors of readmissions after RARP. Moschini et al. 10 analyzed the incidence of 30-day readmission after RARP in a single European center and showed that patients in intermediate to high-risk D'Amico groups and patients who incurred postoperative complications are at a higher risk of readmission. Pilecki et al. 11 compared 30-day postoperative complication and readmission rates between open radical retropubic prostatectomy and RARP using NSQIP (2011). OT and preoperative dyspnea were the only two identified risk factors for readmission after RARP.
Compared with previous studies, our study has two novel differences. First, in addition to readmissions, we evaluated postdischarge complications. Our data showed that among all the patients who had readmissions, only 43.7% were coded to have NSQIP-defined postdischarge complications. This finding is consistent with one previous NSQIP study on general, vascular, and thoracic surgeries, which reported that only 37% of patients had an NSQIP-defined postdischarge complication coded as a reason for their readmission. 9 This is due to specific and strict definitions of individual complications in NSQIP. Some of the reasons (ICD-9 coded) for readmissions did not meet the criteria of NSQIP “complication.” We believe combining readmissions and postdischarge complications could potentially capture all postdischarge adverse events in the NSQIP database. Second, we demonstrated an association between pre- and postdischarge surgical outcomes. We aimed to identify predictors that were on hand before the patient was discharged, which was another reason that we categorized complications into pre- and postdischarge. Unlike other studies showing that postoperative complication was a strong predictor of readmission, our study considered predischarge complication as one of the covariables since only predischarge complication could be available before discharge. 10,15 –17 Adding OT and LOS as another two covariables allowed us to apply all the available predischarge information from the database. Ultimately, we found that predischarge complications, OT, and LOS were associated with readmission and postdischarge complication. Of note, the ORs of 1.002 for OT were based on per 1-minute increase. When changing the unit to 1-hour increase, ORs increased to 1.12 and 1.15 for readmission and postdischarge complication, respectively.
Interpretations and implications
Although several other factors, such as higher ASA score, increasing BMI, and preoperative bleeding disorders, were associated with either a higher risk of readmission or postdischarge complication, only increasing OT and LOS were associated with both readmission and postdischarge complication (Table 1). After we excluded patients with predischarge complications, the results were essentially unchanged (Table 2). One of the main interpretations of the current study is that common quality metrics of the surgery, such as OT and LOS, are associated with readmissions and postdischarge complications after RARP. Readmission is a multifactorial and complex metric that some could argue is an inappropriate measure of surgical quality. However, the associations showed in our study suggest that readmission after RARP may serve as an additional surgical quality indicator, especially when combined with postdischarge complications. The associations between longer OT/LOS and increased risk of readmission and postdischarge complication are probably related to that both factors may be surrogates for surgical complexity and surgical experience. 9,18,19 In addition, longer LOS may also suggest some predischarge adverse events that could not be categorized into any of the NSQIP-defined complications or did not meet the strict definitions of those complications. 9 Indeed, among patients with LOS ≥3 days (n = 908), only 12.9% (n = 117) had coded predischarge NSQIP complications. The reasons for the prolonged LOS in the majority of those patients were not clear.
It is unclear to the degree that variables such as predischarge complications, OT, and LOS can be modified. 18 Postdischarge adverse events are also an inevitable component to having major surgery. Implicitly, efforts to reduce these complications would likely also improve readmission rates. Identifying those patients at higher risk could allow for integrated interventions and targeted resources to decrease the risk of readmission. For a frequently performed procedure such as RARP, it would be ideal to target readmission prevention interventions to high-risk patients. An implication of our study is that we may be able to identify some patients who may have a higher risk of readmission and postdischarge complications before discharge. We then can give those patients specific counseling, more frequent phone calls, and enhanced outpatient management and coordination of care. For example, this can be accomplished on an institutional level with developing surgical pathways involving nurses, physicians, and pharmacists. As refinements are made to predictive risk models, healthcare systems will be able to improve the cost efficiency. 20
Limitations
Limitations of our study are predominantly related to the features of the NSQIP database. First, only 30 days of follow-up are available in NSQIP, and 30-day readmission is counted from the day of surgery instead of the day of discharge. Although we excluded patients with an LOS of longer than 7 days, the immortal time bias was not eliminated. Second, NSQIP is designed to capture data from a wide range of surgical operations and most of the variables in the database are generic in nature. Surgery-specific complications and minor adverse events were not captured in NSQIP. Third, facility-level factors are also not reported in NSQIP, and there are likely institutional differences in counseling, treating, and following patients with a disease process. Early ambulation, opioid-sparing analgesia, timing of catheter removal, obtaining a voiding cystourethrogram, surgical antibiotic prophylaxis, and catheter removal are among some examples of institutional differences. Postoperative care pathways and discharge policies could also differ significantly within a large cohort of hospitals included in the NSQIP. Fourth, detailed pathologic variables are not available in the database, and they may also indirectly be related to complications. Finally, there might be some collinearity between some of the covariables, such as bleeding disorder and OT. Further prospective studies are warranted considering the limitations.
Conclusions
Predischarge complications, OT, and LOS are associated with readmissions and postdischarge complications after RARP. It may be possible to identify patients at higher risk of postdischarge adverse events to direct prevention interventions. Further prospective studies are needed to validate our findings.
Footnotes
Acknowledgments
The American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) and the hospitals participating in the ACS-NSQIP are the sources of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.
Author Disclosure Statement
No competing financial interests exist.