
Abstract
Purpose:
Ionizing radiation is implicated in nearly 2% of malignancies in the United States; radiation shields prevent unnecessary radiation exposure during medical imaging. Contemporary radiation shield utilization for adult patients in the United States is poorly defined. Therefore, we evaluated the prevalence of protective shielding utilization in adult patients undergoing CT scans in United States' hospitals.
Materials and Methods:
An online survey was sent to established radiology departments randomly selected from the 2015 American Hospital Association Guide. Radiology departments conducting adult CT imaging were eligible; among 370 eligible departments, 215 departments accepted the study participation request. Questions focused on shielding practices during CT imaging of the eyes, thyroid, breasts, and gonads. Prevalence data were stratified per hospital location, size, and type. Main outcomes included overall protective shielding utilization, respondents' belief and knowledge regarding radiation safety, and organ-specific shielding prevalence.
Results:
Sixty-seven of 215 (31%) hospitals completed the survey; 66 (99%) reported familiarity with the ALARA (as low as reasonably achievable) principle and 56 (84%) affirmed their belief that shielding is beneficial. Only 60% of hospitals employed shielding during CT imaging; among these institutions, shielding varied based on CT study: abdominopelvic CT (13, 33%), head CT (33, 83%), or chest CT (30, 75%).
Conclusions:
Among surveyed hospitals, 40% do not utilize CT shielding despite the majority acknowledging the ALARA principle and agreeing that shielding is a beneficial practice. Failure to address the low prevalence of protective shielding may lead to poor community health due to increased risk of radiation-related cancers.
Introduction
O
The typical radiation dose associated with a standard CT scan ranges from 1 to 14 mSv, equivalent to the total annual dose of natural radiation that an individual might receive. Radiation dose and its effect on biological tissues are concerning given that 1.5% to 2% of all cancers in the United States are estimated to be due to physician-initiated radiation exposure. 1,2 As a result of concerns over radiation exposure, The United States Nuclear Regulatory Commission developed regulations for radiation safety and established the commonly used acronym, ALARA (“as low as reasonably achievable”) to stress the importance of minimizing radiation exposure. 4 As such, many radiation dose-reduction protocols and CT shielding techniques have been developed.
The use of radiation shields is one of the simplest mechanisms by which radiation dose can be diminished without negatively impacting diagnostic image quality when applied appropriately. 5 –8 Within the past decade, several studies have shown the effectiveness of shielding in decreasing radiation dose exposure to the thyroid, 9 –12 breasts, 11,13 eyes, 7,9,10,14 and testes. 12,14 –17
Accordingly, our objective was to evaluate the prevalence of protective shield utilization in adult patients undergoing routine abdominopelvic, chest, or head CT scans in a randomly selected group of U.S. hospitals.
Materials and Methods
Survey design
We designed a survey consisting of a series of multiple-choice questions pertaining to hospital CT imaging practices, use of organ-specific dosage-reduction protocols, and protective shielding practices, for adult patients. The respondents were first asked whether their department performed adult CT imaging; a negative reply resulted in exclusion from the study. If the reply was affirmative, the full-length questionnaire was presented for completion (Appendix 1). The survey was administered and data were collected using REDCap (Harvard Catalyst, Boston, MA) electronic data capture tools hosted at the University of Southern California. 18 REDCap (Research Electronic Data Capture) is a secure, web-based application designed to support data capture for research studies.
Participant selection and survey administration
Between June 2015 and June 2016, we randomly selected and sent a study participation request to every seventh hospital of the 6295 U.S. hospitals listed in the American Hospital Association (AHA) Guide. Established radiology departments conducting adult CT imaging were eligible for this study. Eligible departments were contacted by phone or email to request the direct contact information for CT personnel (including CT technologists, CT supervisors, radiology managers, and radiation safety officers) capable of completing the survey. These individuals were sent an email invitation to complete the full online-based survey through REDCap. In the initial email, departments were asked to complete the survey within 4 weeks of receipt. Further contact was made with nonresponsive departments 2 weeks following initial contact and again 1 week before the end of the 4-week survey period. No patient-specific information was acquired or recorded during this study.
Hospital data
Descriptive data, including Census Divisions (numbered 1–9), teaching status, community hospital status, bed size data (6–199 beds, ≥200 beds), type of authority responsible for establishing hospital policies (government, nongovernment, investor-owned/for-profit), were obtained from the AHA Guide. Other information, including hospital name, address, and contact information, were also recorded; hospitals were substratified by region (East, Midwest, West, and South).
Study outcomes and statistical analysis
Standard summary statistics were provided for hospital characteristics as well as the overall prevalence and the 95% confidence interval (CI) for protective shielding utilization. Similarly, point estimates and 95% CIs were calculated for the respondents' belief in shielding protection, their awareness of shielding use by other hospitals, and their familiarity with the ALARA safety principle. We compared the prevalence of protective shielding utilization across hospital characteristics, including academic status (teaching or nonteaching), hospital size (≤199 beds or ≥200 beds), geographical region (East, Midwest, South, West), and for for-profit, government, or nongovernment status. These comparisons were based on two-sided Chi-squared tests as well as two-sided Fisher's exact tests when the expected cell counts were less than 5. Similarly, we contrasted the prevalence of protective shielding utilization with the respondents' belief in shielding protection, their awareness of shielding use by other hospitals, and their familiarity with the ALARA safety principles. Finally, we determined the prevalence of organ-specific (i.e., eyes, thyroid, breasts, testes, and uterus and ovaries) shielding with 95% CIs among the 40 hospitals which employed protective shielding.
Results
We identified 370 hospitals with an established radiology department, among whom 62 (17%) refused participation, 93 (25%) did not respond after initial contact, 215 (58%) accepted the survey request, and 83 (39%) submitted responses. Table 1 lists the characteristics of the 67 hospitals that completed the survey. Table 2 reports the prevalence of shielding use at these hospitals (A) and the knowledge and attitudes of respondents with regard to shielding (B), followed by a comparison of shielding prevalence by hospital characteristics and by respondents' attitudes outlined in Table 3. A post hoc analysis comparing the South to all other regions showed no significant difference in use of shielding (p = 0.1008, after adjusting for multiple comparisons).
ALARA = as low as reasonably achievable; CI = confidence interval.
Fisher's exact test two-sided p-value.
A breakdown of the prevalence of shielding use by the type of CT imaging and shielded organs is provided in Table 4 and depicted in Figure 1. Of note, only 20% of these hospitals reported shielding during all three types of CT studies.
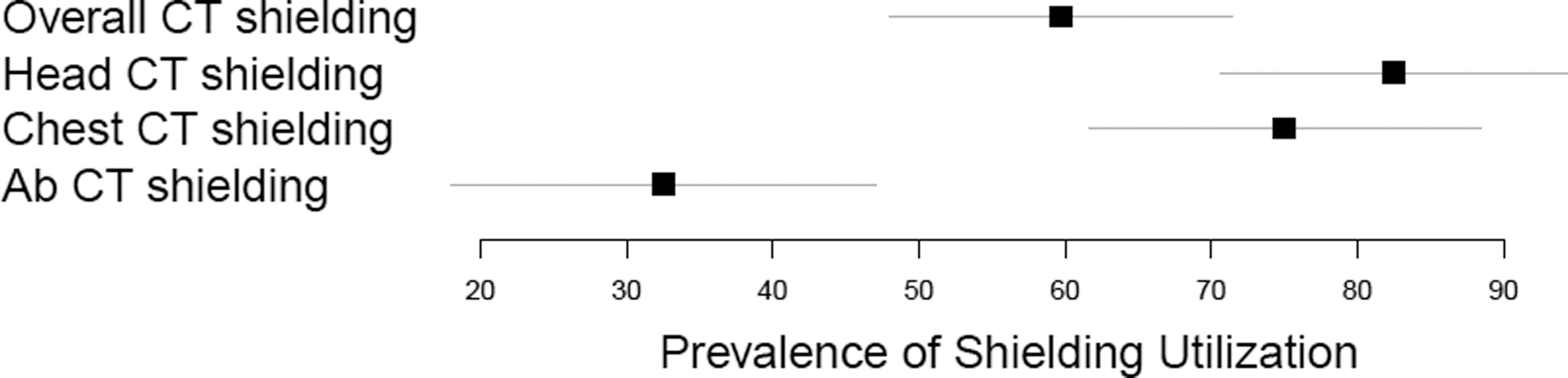
Prevalence of shielding (points) and 95% confidence interval (horizontal lines).
Discussion
The use of CT scans has dramatically increased, from about 3 million CT scans in 1980 to 70 million per year in 2007. 1,3 The deleterious effects resulting from exposure to ionizing radiation can be divided into two types: deterministic and stochastic. Deterministic effects (e.g., epilation, cataracts, etc.) only occur after a certain threshold of radiation is exceeded and generally do not apply for the amount of radiation from CT scans. 19 Stochastic effects, however, increase the probability of deleterious effects (e.g., genetic mutations and cancer) occurring with each radiation exposure, and therefore are an important concern with regard to CT imaging. 20 Several studies have directly linked iatrogenic radiation exposure to cancer risk; indeed, a recent study by Leuraud and colleagues. demonstrated a strong positive association between cumulative low-dose radiation exposure and risk of death due to leukemia. 2,21 –25 Furthermore, the risk of developing solid cancers due to radiation exposure increases throughout adulthood until age 60. 26 In this regard, there has been much interest in dose reduction to the imaged organs. For example, tube current modulation during abdominopelvic CT has dropped radiation exposure by as much as 68%. 27,28
Using shields during CT scans is perhaps the simplest modality for decreasing patient radiation exposure. 29 Numerous studies have reported remarkable radiation dose reduction due to radiation shields. Indeed, a study by Hohl and colleagues regarding testicular shielding during abdominopelvic CT scans demonstrated a drop from a mean testicular radiation dose of 2.40 to 0.32 mSv, an 87% reduction in radiation dose to the testes without any diagnostic impairment. 15 They additionally pointed out two other studies that showed similar dose reductions of 95% and 77% to the testicles. Another recent study investigating the effects of bismuth for eye shielding during brain CT scans demonstrated a 21% to 29% dose reduction to the lens of the eye, with no negative effect on CT image quality. 7 Identically, Hopper and colleagues reported radiation dosage reduction of up to 50% when bismuth-coated latex shielding of the eye is used during cranial CT. 30 A similar study concerning breast and thyroid shielding during chest CT scans recorded a 30% and 50% dose reduction, respectively. 31 Other studies have similarly corroborated significant dose reduction due to shielding techniques. 9,11
Despite these striking numbers, radiation shielding has been a topic of debate in the literature. 32 Some studies have indicated an increase in image noise in the area directly underlying the protective shield 31,33,34 ; in contrast, other studies indicate no significant effect on diagnostic image quality. 7,8,35 Radiation shields can be placed either over the area being studied and thus in the path of the radiation beam (i.e., “in-plane” shielding), or placed over areas outside of the area of interest (i.e., “out-of-plane” shielding). This is an important distinction as “in-plane” shielding can increase image noise, and thereby reduce image quality. 33 Additionally, if improperly applied, the dose reduction benefits of in-plane shielding can be lost. Following the results of their study investigating abdominal shielding during chest CT scans, Iball and Brettle strongly advocate for the use of “out-of-plane” shielding given the significant dose-reduction benefits and avoidance of potential image noise. 8
In the foregoing national survey, we found that while the vast majority of radiology personnel responsible for conducting diagnostic adult CT imaging are aware of the ALARA safety principle, they believe that shielding practices are beneficial to patients. Despite this belief, overall only 60% of hospitals utilized radiation shields, and among these hospitals only 20% employ protective shielding for all three types of CT imaging. Similarly concerning is that while the ovaries cannot be shielded during abdominopelvic scanning, none of the hospitals elected to use gonadal shielding among their male patients during abdominopelvic CT scanning. With the increasing prevalence of CT imaging, there is significant opportunity to reduce ionizing radiation exposure with the thoughtful application of shielding.
In our post hoc analysis, we found notable variance with respect to organ-specific shielding practices. Gonadal shielding was more prevalent than shielding for the eyes or thyroid, and shielding during head and chest CT was more common than during abdominopelvic scans. One potential reason for this low use of shielding could be the effectiveness of dose reduction due to organ-based tube current modulation, in which CT tube current is automatically reduced when nearing certain organs. 33,36,37 This type of automatic exposure control may counteract the shield. 37 Therefore, several studies discourage concurrent shielding and tube current modulation. 5,29,37
A limitation of our study was the low overall response rate; taking into account the 370 radiology departments we contacted, only 22% submitted a response, and 18% fully completed the survey. However, this concern is mitigated by the use of Fisher's exact test on the assessment of our data. Unfortunately, this does not account for the possibility that we may be over- or underestimating shielding compliance as we did not query nonhospital radiology service settings, such as surgical centers or clinics. Survey administration and response rate could have potentially been improved by sending a hardcopy letter first, followed by the actual web-based survey delivered through email. 38,39 Another limitation of this study is that it was fully based on self-reporting from a single individual at each hospital; we did not audit responses nor confirm the compliance with shielding at the hospitals. Similarly, the reply was completed by a diverse array of individuals in the various radiology departments. This may indicate a possible reason for the low response rate, and may highlight a nonresponse bias in that individuals who did not complete the survey may have felt unqualified to respond. Another weakness of the study was that respondents were not queried regarding why they elected to not use shielding as we had, as it turned out, erroneously assumed that the use of shielding would be widespread. An additional consideration is that survey participants may have found the nature of this study to be provocative, and thus avoided responding. If so, we may have underestimated how many departments fail to shield patients.
Conclusions
To the best of our knowledge, this is the first study to examine national shielding practices during CT imaging in adults. Given the steep rise in the use of CT scanning and recent information about the risk of radiation exposure associated with cancer, there is a need to limit radiation. In keeping with the ALARA principle, we believe that employing appropriate in-plane and out-of-plane shielding of all radiosensitive organs during CT imaging is a simple and necessary method to markedly reduce nontarget organ ionizing radiation exposure. Paradoxically, while the vast majority of radiology departments recognize the importance of ALARA and the benefit of shielding, most do not put these beliefs into practice. The reason for this conundrum has yet to be elucidated. Regardless, in our opinion, the next step is to better educate the public about the rise of radiation exposure in hope that patient demand for shielding will push more hospitals to adhere to their stated practices. In the hopefully near future, CT scanning without appropriate shielding may well be considered yet another “never event” which when violated would result in sanctions, both financial and reputational.
Footnotes
Acknowledgments
The authors thank Rahul Dutta, MD, for help with data collection, and Danh V. Nguyen, PhD and Tuyen Hoang, PhD, for help with the data analysis. In addition, the authors acknowledge the statistical support received from the Institute for Clinical and Translational Science at the University of California, Irvine.
Authors' Contributions
All authors had a role in preparing this article.
Author Disclosure Statement
No competing financial interests exist.