
Abstract
Objective:
Vascular calcifications are associated with nephrolithiasis. Although studies have demonstrated correlations with vascular disease and calcium stones in kidney stone formers (KSF), an etiologic link has remained elusive. As a noncontrast CT (NCCT) scan is typically part of a stone evaluation, our objective was to evaluate the association of NCCT-based assessment of abdominal aortic calcifications (AACs) with 24-hour urine parameters and stone composition.
Materials and Methods:
Ninety-seven KSF were included with CT imaging and 24-hour urine studies. For each patient, semi-automated CT software was utilized to provide an AAC Agatston score from the celiac axis to the aortic bifurcation. Univariate analysis was performed to compare patients with or without AAC. Multivariate logistic regression was performed to assess for variables associated with 24-hour urine parameters and stone composition.
Results:
The presence of AAC was associated with hypertension, diabetes, peripheral vascular disease, and coronary artery disease. Patients with any AAC showed lower 24-hour urine citrate (399 vs 593 mg/day, p < 0.001) and lower 24-hour urine pH (5.862 vs 6.328, p = 0.003). When controlling for age, system comorbidities, the presence of AAC was associated with low urine pH <6 (odds ratio [OR] 2.86, p = 0.032) and hypocitraturia <320 mg/day (OR 4.37, p = 0.005). The receiver operating characteristic curve showed that increasing AAC was associated with low urine pH (area under the curve [AUC] 0.683, p = 0.002) and uric acid stone formation (AUC 0.698, p = 0.045).
Conclusions:
NCCT-based diagnosis of AAC is associated with low urine pH, hypocitraturia, and uric acid stone formation. The presence of AAC could be considered an additional prognosticator for the utility of alkalinization therapy.
Brief Description: This study demonstrates that patients exhibiting abdominal aortic calcifications on noncontrast CT have low urine pH and hypocitraturia on 24-hour urine studies and are prone to uric acid stone formation.
Introduction
T
Noncontrast CT (NCCT) imaging is the gold standard for detection of urinary calculi, and its utilization has increased to 71% in the work-up of renal colic in emergency rooms. 6 The American Urological Association (AUA) surgical management of stones guidelines provide a strong recommendation for CT imaging before surgical intervention. 7 As CT utilization increases and healthcare cost control becomes more critical, the concept of “opportunistic imaging” arises. Opportunistic CT imaging (1) provides retrieval of data on CT examinations that are ordered for other indications (urolithiasis), (2) carries no additional cost to the patient, (3) does not require additional equipment, and (4) carries no additional radiation exposure. 8 A quantitative assessment of abdominal aortic atherosclerosis observed in CT scans was first described in 1997. 9 The assessment of AAC in an opportunistic manner was introduced in 2006, when AAC score was obtained on patients undergoing CT colonography to assess risk for cardiac-related events. 10
Prior studies have demonstrated that kidney stone formers (KSF) with calcium kidney stones display higher degrees of aortic calcification than non-KSF. 11 The aim of this study is to identify the associations of AAC on an NCCT scan performed for the evaluation of nephrolithiasis with subsequent 24-hour urine metabolic studies and stone composition.
Materials and Methods
After Institutional Review Board approval was obtained for a query of our Kidney Stone Registry, 97 patients were identified as meeting the inclusion criteria of: noncontrast abdomen/pelvis CT imaging at the time of diagnosis of nephrolithiasis and at least one complete postimaging 24-hour urine study (urine volume, calcium, oxalate, citrate, sodium, uric acid, pH) within 6 months of imaging. Twenty-four-hour urine studies were ordered after the passage of stone or intervention and before initiating preventative medications. The Kidney Stone Registry contains patients seen from 2010 to 2016 by multiple urologists and nephrologists at a large, tertiary, academic center. It includes surgical and metabolic data from surgical and preventative clinics. Additional variables extracted from the registry included age, gender, body mass index (BMI), medical comorbidities (history of hypertension, diabetes, peripheral vascular disease, CAD), alcohol history, tobacco history, ever receiving a stone surgery (ureteroscopy, percutaneous nephrolithotomy, shockwave lithotripsy), and predominant (>50%) stone analysis component if available (calcium oxalate, calcium phosphate, uric acid, or struvite). Serum chemistry studies were also collected, including: parathyroid hormone, uric acid, vitamin D-25 hydroxy, calcium, sodium, potassium, chloride, and bicarbonate.
For each patient's CT scan, semi-automated software, Aquarius iNtuition (version 4.4.6; TeraRecon, Inc., San Francisco, CA) was utilized to assess the aorta from the celiac axis to the aortic bifurcation, which was manually isolated as the region of interest. A patient was considered to have any AAC if calcifications ≥1 mm3 and voxels with attenuation >130 HU were present in the distal 8 cm of aorta. The Agatston method was then utilized to provide an AAC score (Fig. 1). 5 Stone volume was assessed with Siemens syngo ® .via Calcium scoring software (Erlangen, Germany).
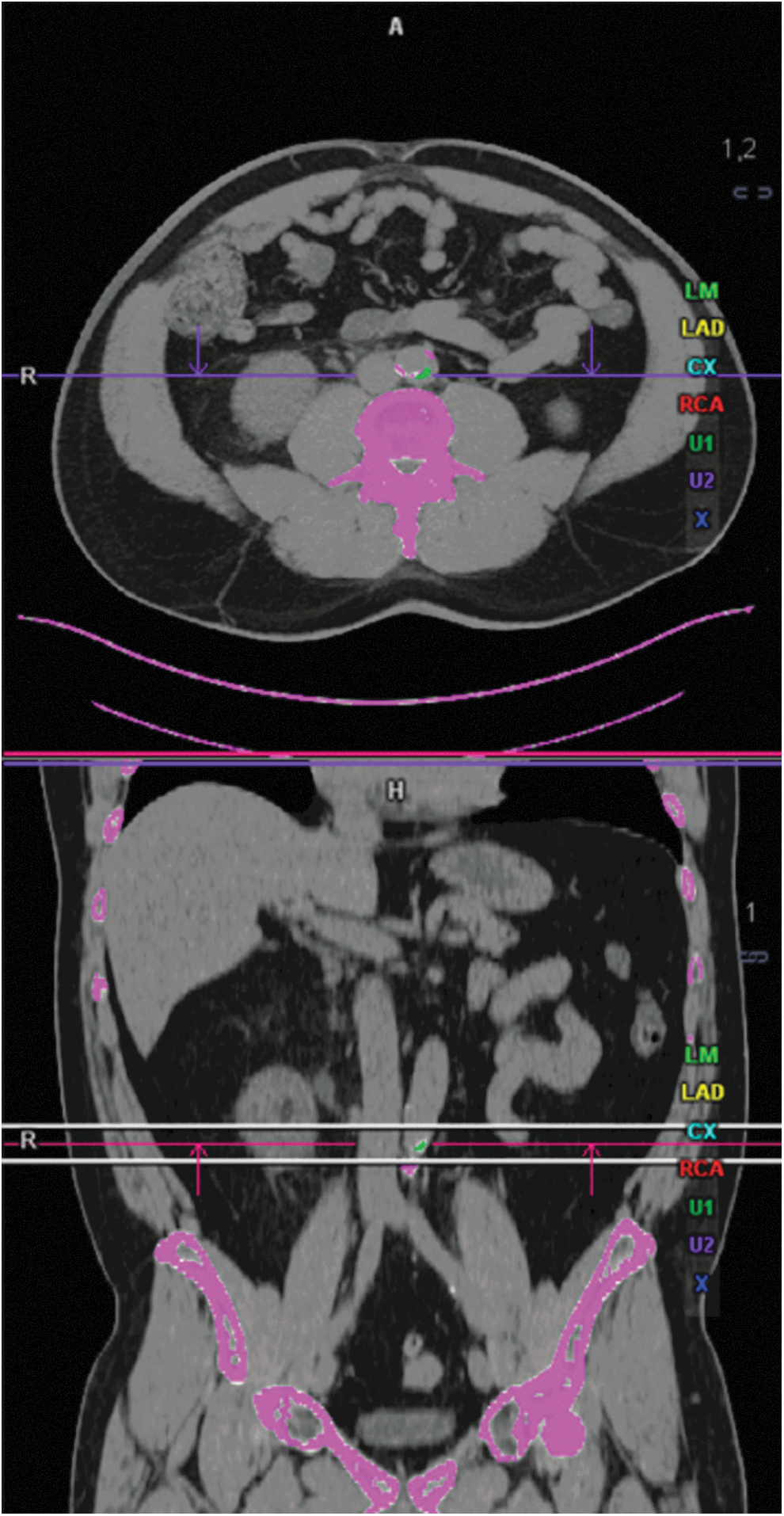
Detection of abdominal aortic calcifications defined as calcifications ≥1 mm3 and attenuation >130 HU present in the distal 8 cm of aorta.
Patients with and without any AAC were compared with independent-samples t-test (for normally distributed continuous variables), Mann–Whitney U-test (for non-normally distributed continuous variables), and chi-square likelihood ration or Fisher's exact test (for nominal and categorical variables). Spearman's rank correlation coefficient was obtained to assess for correlations between 24-hour urine parameters and AAC. Multivariate logistic regression was performed by a backward conditional method to assess for variables associated with AAC, 24-hour urine parameters, and stone composition. A two-sided p-value <0.05 was considered to represent a statistically significant difference. Receiver operating characteristic (ROC) curves were constructed for AAC (test variables) and 24-hour urine parameters and stone composition (outcome). The area under the curve (AUC) was calculated to assess for the performance of AAC in identifying 24-hour urine derangements and stone composition. Statistical analyses were performed with SPSS software (version 25; SPSS, Inc., Chicago, IL).
Results
Table 1 displays patient demographics. Overall, 51.5% of patients in the cohort underwent stone surgery, mean age was 59 ± 17 years, mean BMI was 31.2 ± 8.3 kg/m2, the most common predominant stone composition was calcium oxalate (46.4%), mean AAC score was 1445 ± 2782, 64% of patients exhibited any AAC, and mean stone volume was 179 ± 357 mm3. Table 2 compares patients with and without AAC. Compared with patients without AAC, patients with AAC were older (68.6 years vs 43.6 years, p < 0.0001), had lower 24-hour urine citrate (399 mg/day vs 593 mg/day, p = 0.001), lower 24-hour urine pH (5.862 vs 6.328, p = 0.003), higher serum uric acid (6.5 mg/day vs 5.6 mg/dL, p = 0.021), and larger stone volumes (247 mm3 vs 66 mm3, p = 0.005). Patients with detectable AAC had a higher prevalence of hypertension (85.5% vs 34.3%, p < 0.0001), diabetes (33.9% vs 5.75%, p = 0.002), peripheral vascular disease (19.4% vs 2.9%, p = 0.022), and CAD (33.9% vs 2.9%, p < 0.0001). Overall, 64.7% of calcium phosphate KSF had no AAC and 80% of uric acid stone KSF had evidence of AAC.
AAC = abdominal aortic calcification; BMI = body mass index; CAD = coronary artery disease; SD = standard deviation.
Bold type signifies a significant p-value difference.
Correlations between AAC with 24-hour urine parameters and stone volume are shown in Table 3. Significant correlations were seen with 24-hour urine citrate (R = −0.05, p = 0.014), 24-hour urine pH (R = −0.353, p < 0.0001), and stone volume (R = 0.368, p < 0.001). Multivariate analysis demonstrated that while controlling for other comorbidities, gender, low urine pH and urinary citrate, presence of diabetes (odds ratio [OR] 11.46, p = 0.031), and age older than 60 years (OR 13.5, p = 0.002) significantly correlated with finding any AACs on CT imaging. Although controlling for age, hypertension, diabetes, and CAD, multivariate regression analysis demonstrated that obesity (OR 3.04, p = 0.02), male gender (OR 3.52, p = 0.009), and presence of AAC (OR 2.86, p = 0.032) were associated with low 24-hour urine pH <6 (Table 4). Controlling for age and comorbidities, the presence of AAC (OR 4.37, p = 0.005) was associated with hypocitraturia, citrate <320 mg/day (Table 5). Low urine pH was associated with uric acid stone formation (OR 11.3, p < 0.002), and a nonsignificant association with AAC and uric acid stones was observed (OR 3.0, p = 0.186). Table 6 shows ROC curve analysis with AUC values for AAC. The AUC for increasing AAC to identify low urine pH was 0.783 (p = 0.002), hypocitraturia was 0.619 (p = 0.052), and uric acid stone formation was 0.698 (p = 0.045).
Bold type signifies a significant p-value difference.
Bold type signifies a significant p-value difference.
Bold type signifies a significant p-value difference.
Bold type signifies a significant p-value difference.
Discussion
Our study highlights several important findings that are relevant to KSF. Foremost, KSF with the presence of any AACs on CT imaging demonstrated lower urinary citrate (399 mg/day vs 593 mg/day, p = 0.001), lower urine pH (5.862 vs 6.328, p = 0.003), and larger stone volumes (247 mm3 vs 66 mm3, p = 0.005). A high percentage of uric acid stone formers (80%) demonstrated AAC and though the presence of AAC did not correlate with uric acid stones, an increasing AAC severity score on preoperative imaging did predict uric acid stone formation with an AUC of 0.698. Although controlling for age and diabetes, the presence of AAC was associated with low urine pH (OR 2.86) and finding hypocitraturia (OR 4.37) on 24-hour urine studies. Finally, we demonstrated that a greater severity of AAC was linked to a 24-hour urine pH below 6 (AUC 0.683).
The association of vascular disease and nephrolithiasis has been established by prior studies. In a study of 4564 KSF compared with age- and gender-matched controls, Rule and colleagues found that KSF were at a 31% increased risk of myocardial infarction while adjusting for chronic kidney disease and other comorbidities. 12 By extracting data from the Coronary Artery Risk Development in Young Adults study, Reiner and colleagues demonstrated an association between a history of kidney stones and subclinical carotid atherosclerosis in young adults aged 18–30 years. 13 Hsi and colleagues utilized data from the Multi-Ethnic Study of Atherosclerosis (MESA) cohort study to demonstrate that recurrent kidney stone formation was associated with moderate or severe coronary artery calcifications. 14 Utilizing an AAC scoring method, Shavit and colleagues showed that calcium KSF and non-KSF have a similar prevalence of AAC (38% vs 35%, p = 0.69), whereas calcium KSF have higher degrees of aortic calcification compared with non-KSFs. 11
A vascular theory behind the association between Randall plaques and calcium stone formation has been proposed. 15 First, as regions of turbulent flow, including the bifurcations of major arteries, are predisposed to inflammation and atherosclerosis, the turbulent flow at the renal papillary tip with a 180-degree transition may induce plaque and subsequent stone formation. Second, the hyperosmolar papillary tip accumulates inflammatory cytokines and may result in plaque aggregation. Third, as the papillary tip demonstrates decreased oxygen-carrying capacity, this may result in a sloughed papilla and subsequent inflammation and plaque formation. Although these theories may explain calcium stone formation in vasculopathic patients, they may not account for the findings in our study, namely the association between aortic calcifications and uric acid stone formation or AAC and risk factors for uric acid stone formation (i.e., low urine pH).
Urine pH affects the overall risk of stone disease by precipitating uric acid crystals in a pH <6. Insulin resistance has been theorized as an etiology for uric acid nephrolithiasis in KSF. Insulin resistance leads to impairment in renal ammonia secretion, thereby resulting in the decreased buffering capacity for urinary acidification, with the final product being low urinary pH and potentially uric acid nephrolithiasis. 16 An analysis of 1632 participants from the MESA cohort demonstrated that insulin resistance, as estimated by the homeostasis model assessment-insulin resistance index, was associated with the presence of coronary artery calcifications, but not AACs. 17 In our cohort, a history of diabetes and associated insulin resistance was associated with a nearly 12-fold risk of detecting AAC on CT imaging. In addition, visceral fat volume has been shown to be significantly correlated to abdominal aorta atherosclerosis. 18 Analysis of data from a concurrent study on our same cohort also demonstrated that patients exhibiting AAC had a higher visceral fat area (VFA). 19 Visceral obesity, through high fatty acids and low adiponectin, has been implicated in the development of insulin resistance. 20 The visceral fat compartment, as opposed to the subcutaneous fat compartment or total obesity (represented by BMI), has been associated with uric acid stone formation and may predict uric acid nephrolithiasis better than BMI or urinary pH, with insulin resistance defining the underlying mechanism. 21,22
Screening for abdominal aortic calcium is important as the diagnosis carries significant predictive value. In a study of 1974 participants in the MESA cohort, AAC was independently related to cardiovascular disease mortality rate, and AAC showed a stronger association than coronary artery calcification with total mortality rate. 23 Our study presents a method for AAC screening by utilizing existing NCCT scans to identify patients at risk for cardiovascular events and utilizing AAC to predict stone composition and 24-hour urine abnormalities. As such, screening for AAC may identify KSF who are at higher risk for a perioperative cardiac or cerebrovascular event, and it may help select those who could benefit from more aggressive perioperative evaluation and preparation.
Previously, the utilization of HU on CT imaging was shown to have a sensitivity of 86%, a specificity of 87%, and an AUC of 0.852 in predicting uric acid stones. 24 We propose that the additional finding of AAC (AUC 0.698) may also be potentially applied to predict uric acid stone composition. Our ROC curve analysis demonstrated that increasing AAC correlated with low urine pH (AUC 0.683). This finding is relevant during the decision-making process as to which patients would benefit from further work-up with a 24-hour urine study. The AUA Guidelines on the Medical Management of Kidney Stones recommend additional testing for high-risk or interested stone formers. 25 However, as a maximum of 35% of 24-hour urine studies may show no abnormality, 26 judicious and appropriate ordering of this study may avoid unnecessary testing. High-risk KSF are generally categorized by having a large stone burden, uncommon composition (cystine), comorbid system conditions (gout, Crohn's disease, sarcoidosis), or urogenital abnormalities (solitary kidney, ureteropelvic junction obstruction). In addition to these traditional risk factors, we propose that patients demonstrating AAC on CT imaging can also be considered at high risk and may benefit from additional 24-hour urine studies that may reveal low urinary pH or low urinary citrate. Alternatively, empiric use of potassium citrate supplementation may be warranted in those with AAC.
Although screening for AAC is important, directed treatment strategies based on screening findings may treat calculi with dissolution or decrease further kidney stone recurrence. Standard therapies for low urine pH in recurrent KSF may consist of alkali drugs (potassium citrate, sodium bicarbonate or sodium citrate). Oral dissolution therapy for the treatment of uric acid nephrolithiasis with potassium citrate may prevent endourologic intervention in a maximum of 73% of patients. 27 Prevention of uric acid stone recurrence with citrate therapy has been reported to be as high as 94% of patients experiencing remission from uric acid stone episodes. 28 Further studies will evaluate the prognostic value of AAC in a model for predicting response to alkalinization therapy.
This is the first study to our knowledge to demonstrate an association of CT-based diagnosis of AACs with uric acid nephrolithiasis and low urine pH and citrate on a subsequent 24-hour urine study. However, some limitations regarding our study warrant discussion. First, clinical data were collected in a retrospective manner and inferences regarding the ability of CT-assessed AAC to predict 24-hour urine findings may be limited by unknown confounding factors. Second, although we included a history of other comorbidities, including hypertension, peripheral vascular disease, and CAD, our data did not include an analysis of cardiovascular events after CT imaging and diagnosis of AAC. Third, our cohort included a small number of uric acid KSF (10 of 98), thus limiting the impact and generalizability of our results. Fourth, we did not account for potential medications, such as certain anti-hypertensives, that may alter urine pH and confound the results. Finally, we did not account for the impact of VFA in patients exhibiting AAC and underlying insulin resistance may confound our results. As such, elevated visceral fat and AAC may express collinearity (i.e., vascular disease is associated with visceral obesity and components of the metabolic syndrome) and insulin resistance itself may be the etiology of our findings of low urine pH and uric acid stone predisposition, rather than a purely vascular etiology. Further studies examining the relationship between vascular calcifications and low urine pH will be valuable in supporting our findings.
Conclusions
AAC diagnosed on an NCCT scan performed for nephrolithiasis is associated with low urine pH and low urine citrate on subsequent 24-hour urine studies. When AAC was present, a greater AAC score predicted uric acid stone formation. This information can provide valuable screening mechanisms as to which KSF may be at risk for future cardiovascular events, uric acid stone formation, or exhibiting abnormalities on 24-hour urine evaluations. Our findings may also guide treatment decisions to prevent future stone recurrences.
Footnotes
Author Disclosure Statement
No competing financial interests exist.