
Abstract
Objectives:
To present the first prospective randomized comparison between laparoendoscopic single-site surgery (LESS) and minilaparoscopy (ML) for treatment of upper urinary tract pathologies.
Patients and Methods:
Between January 2013 and June 2015, patients with different upper urinary pathologies were blindly randomized to both LESS and ML. All procedures were done by single experienced surgeon. Both cohorts were compared regarding demographic data, peri and postoperative characteristics, and visual analog pain scale (VAS). Cosmetic outcome was assessed after 12 months using patient scar assessment scale (PSAS) and observer scar assessment scale (OSAS).
Results:
Sixty patients were randomized into two equal groups with comparable demographic and preoperative characteristics. Indications included nephrectomy, pyeloplasty, cyst marsupialization, adrenalectomy, and repair of retrocaval ureter. Operative time was 167 ± 24 and 145 ± 39 minutes in LESS and ML groups, respectively (p = 0.09). Estimated blood loss was 59 ± 34 and 43 ± 42 mL in both groups, respectively (p = 0.2). VAS was 1.7 ± 0.6 and 2.8 ± 0.5 in both groups, respectively (p = 0.02). PSAS and OSAS were 5.9 ± 0.85 and 10.6 ± 1.98 vs 8.9 ± 0.9 and 13.5 ± 6.3 in both groups, respectively (p > 0.05). There were no intraoperative complications, conversions to open surgery, or conventional laparoscopy in both groups. Mean postoperative Diclofenac Na was 151.7 ± 35.6 and 169.7 ± 47.3 mg in both groups, respectively (p = 0.04). Postoperative complications rate and hospital stay were comparable between both groups.
Conclusion:
Both LESS and ML have comparable operative time, blood loss, complication rate, and hospital stay in treatment of upper urinary tract pathologies. However, LESS is associated with less analgesic requirement and better cosmetic outcome.
Introduction
L
The CL has recently evolved to minilaparoscopy (ML) in an attempt to decrease trauma to the abdominal wall, improve cosmetic outcome and recovery, as well as to avoid the challenges that come with LESS by offering smaller instruments that still preserve triangulation. 10 –12
LESS and ML reports have been limited mainly to case–control and retrospective studies from specialized laparoscopic centers, and there is no direct comparison between the two techniques. Our aim is to compare between LESS and ML for treatment of different upper urinary tract pathologies by conducting the first prospective randomized trial comparing both cohorts.
Patients and Methods
Study design
After IRB approval, a total of 60 patients with different upper urinary tract pathologies that warranted a urologic surgical intervention were randomized to either LESS or ML in the period between January 2013 and June 2015, the study was powered to detect a statistical significance of p-value of ≤0.05, and as such 30 patients were deemed necessary for this purpose. Randomization was structured by Alexandria University biostatistics department, where closed envelop randomization method was used. All procedures were performed by a single surgeon (AMA) at Alexandria main university hospital.
Patients
Inclusion criteria: • Patients older than 3 years. • Patients with upper urinary tract pathologies.
Exclusion criteria: • Patients with lower urinary tract pathologies. • Patients with absolute contraindications to laparoscopy.
Methods
ML was done using three-instruments, including 3 mm laparoscope (Karl Storz, Tuttlingen, Germany). Standard port arrangement was set according to each individual procedure and all procedures were done through the transperitoneal approach. On the contrary, in the LESS procedures, Covidien (SILS™) access port (Covidien, Chicopee, MA) was used in all patients through a 25 mm longitudinal transumbilical skin incision. An EndoEye 5 mm camera (Olympus, Tokyo, Japan) was used in all cases as well as both articulating and straight instruments. Both groups were compared regarding patients' demographic data, pre-, peri-, and postoperative parameters, indications for surgery, as well as a cosmetic outcome after 12 months. Visual analog pain scale (VAS) at discharge was used to assess pain. Cosmetic outcome was objectively assessed at 12 months postoperatively using the standardized patient scar assessment scale (PSAS) and observer scar assessment scale (OSAS) that were developed by plastic surgeons to evaluate skin scars. 13
Statistical analysis
Data were fed to the computer using IBM SPSS software package version 20. Qualitative data were described using number and percent. Comparison between different groups regarding categorical variables was tested using Chi-square test. Quantitative data were described using mean and standard deviation for normally distributed data. For normally distributed data, comparison between two independent populations was done using t-test. Significance of the obtained results was judged at the 5% level.
Results
Sixty patients were randomized into two equal groups (n = 30). Patients' demographics and preoperative characteristics are summarized in Table 1. There was no statistical significance in regard to all aspects between the two groups. Indications of surgery are summarized in Table 2. In LESS group, there were 2 adrenalectomies, 9 nephrectomies (5 simple and 4 radical [T1–2; 2 chromophobe, 1 papillary carcinoma, and 1 clear cell carcinoma]), 9 pyeloplasties, 9 cyst marsupializations, and a case of retrocaval ureter. In ML group, there were 3 adrenalectomies, 9 nephrectomies (5 simple and 4 radical [T1–2; 1 chromophobe, 2 papillary, and 1 clear cell carcinoma]), 9 pyeloplasties, and 9 cyst marsupializations.
LESS = laparoendoscopic single-site surgery; ML = minilaparoscopy.
NFK = nonfunctioning kidney; RT = renal tumor.
Peri- and postoperative characteristics are summarized in Table 3. Operative time and estimated blood loss were comparable between both groups. There were no intraoperative complications or conversions to either open surgery or CL in both groups. Also, postoperative hospital stay was comparable in both cohorts. Five millimeters extra port was added in three cases of LESS pyeloplasties and the retrocaval ureter repair. Meanwhile, in ML group, we used a 10 mm port in 12 cases (3 adrenalectomies and 9 nephrectomies) to use the Hem-O-lock clip applier.
OSAS = observer scar assessment scale; PSAS = patient scar assessment scale; VAS = visual analog pain scale.
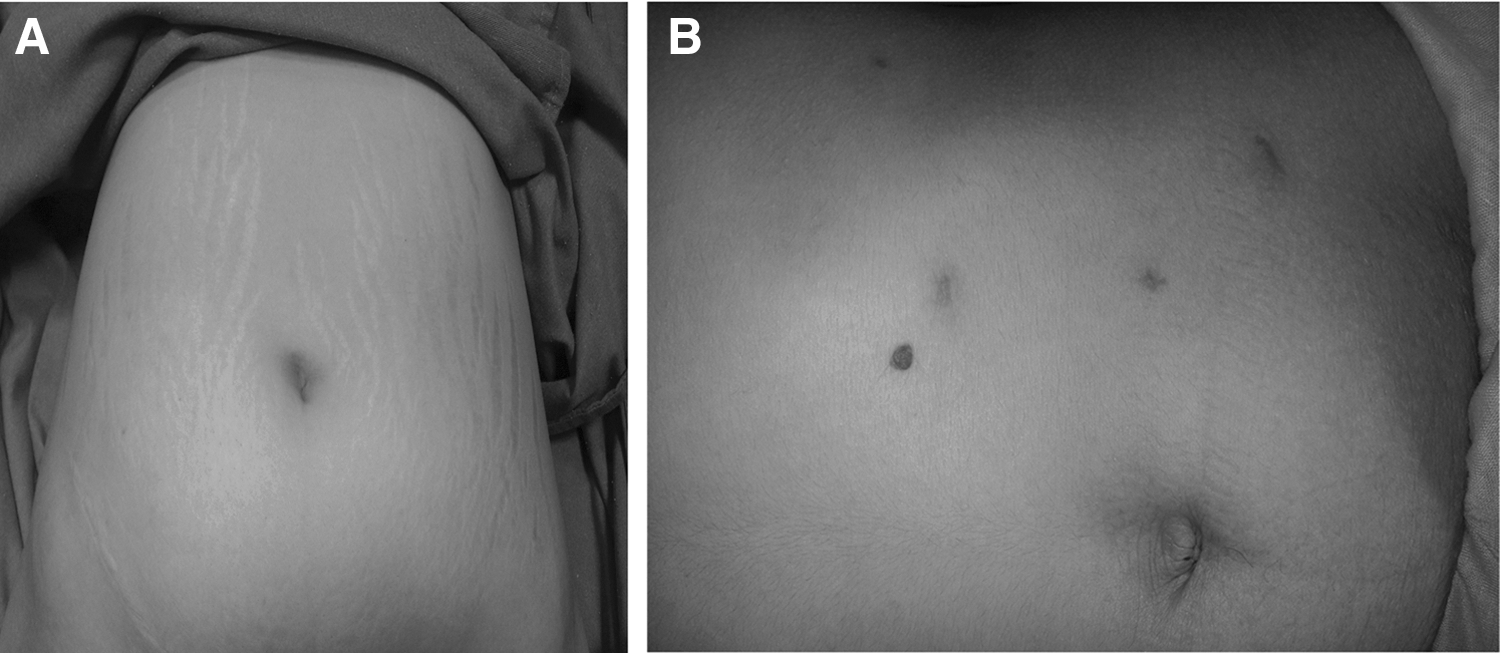
In LESS ablative procedures, specimens were extracted through the port insertion site where the original incision was extended and the size of the incision was related to specimen's size (Fig. 1A), while in ML ablative procedure, the site of insertion of the 10 mm port was extended and through which the specimen was extracted (Fig. 1B)

Mean inpatient analgesic requirement in the postoperative period was 151.7 ± 35.6 mg of Diclofenac Na in LESS Vs 169.7 ± 47.3 mg in ML (p = 0.04), and also, VAS at discharge was significantly less in LESS group (1.7 ± 0.6 in LESS and 2.8 ± 0.5 in ML) (p = 0.02).
Postoperative complications were reported in 6.6% and 3.3% both in LESS and ML groups; respectively; while following simple nephrectomy, one case developed mild wound infection after LESS, and another had prolonged clear fluid drainage into the tube drain for 6 days following ML nephrectomy that resolved spontaneously, while another patient with LESS pyeloplasty had urinary tract infection (UTI) that was managed with antibiotics. All postoperative complications in both cohorts were classified according to modified Clavien–Dindo score (Table 3). 14
In LESS group, PSAS was 5.9 ± 0.85 while OSAS was 10.6 ± 1.98. Meanwhile, In ML group, PSAS was 8.9 ± 0.9 and OSAS 13.5 ± 6.3. The difference was statistically significant with a p-value of 0.02 (Fig. 2A, B).
Discussion
Robot-assisted and pure laparoscopic surgery have become the standard of care for many urologic procedures since their introduction in the 1990s. 15 The evolution toward minimally invasive surgeries have been driven by the lower degree of pain, better cosmetic results, and optimal outcomes associated with these procedures when compared with the open surgery. 16
CL surgery typically results in multiple trocars triangulated toward targeted tissue, which subsequently results in multiple skin incisions and abdominal wall openings with associated multiple scars and other port-related complications. 17 The principle of scarless surgery is gaining more popularity in the field of urology over the last few years. This concept leads to development of new surgical approaches, such as LESS, natural orifice translumenal endoscopic surgery (NOTES), and ML, aiming to minimize the surgical morbidity associated with CL, faster recovery of patients, and better cosmetic outcomes. 18 However, it seems that only hybrid NOTES or NOTES-assisted laparoscopic procedures are the current applications of NOTES in the clinical practice. 19,20 LESS is getting more worldwide adoption both in urology and other specialties with reported superiority to CL related to postoperative pain cosmetic outcome. 7,21 However; although feasible, pure LESS is still a real technical challenge for the surgeons. ML has gained recent interest. This interest was encouraged by the development of special optics and instruments that may minimize abdominal trauma and decrease the postoperative surgical scars while maintaining the concept of triangulation. However, in the field of urology, reports of ML are mainly case–control and retrospective studies. 12,22,23
To our knowledge, to date, there is no direct comparative studies between LESS and ML in urology. In the current study, we present the first prospective randomized comparative study between LESS and ML for treatment of different upper urinary tract pathologies. The current study included two comparable cohorts of patients with almost identical demographic data and indications for laparoscopic interventions. Porpiglia et al. retrospectively reported the safety and efficacy of ML that was performed in 192 patients in multi-institutional European study, using 3 mm instruments with excellent outcomes, when compared with the standard laparoscopy literature. 10 About 70% of their patients had upper urinary tract nononcologic ML procedures. Their results are to a great extent comparable to our results of ML group in the current study, except for the longer mean hospital stay (5 ± 2.1 days), which may be related to the fact that their study included more complex indications such as radical prostatectomy and partial nephrectomy as well as the multi-institutional nature of their study that included different surgeons with variable level of surgical experience and different surgical protocols. Recently, Breda and colleagues reported a prospective multicentric study from six laparoscopic Spanish centers that included 110 patients who had renal and adrenal ML. They concluded that ML was superior to CL and resulted in excellent pain control and cosmetic outcomes, despite having longer operative time. 24
Our results of LESS group of patients are comparable with those that have been published in the literature. 7,12,18,21,25,26 However, the complication rate in our group of patients is less than what has been reported in the literature. This may be explained by the fact that the current study was done by a single surgeon who probably acquired a good experience in LESS before starting this study, while most of the reported LESS studies are multi-institutional studies that included a large group of surgeons with variable levels of surgical expertise. Also, the current group of patients did include neither lower urinary tract LESS indications nor LESS partial nephrectomies, which are associated with higher surgical difficulty and probably higher complication rate. 27 Comparison between LESS and ML groups in the current study showed that both cohorts of patients had comparable blood loss, hospital stay, complication rate, and convalescence. Operative time was longer in the LESS group, which reflects the technical difficulty that was related to loss of triangulation and difficult ergonomics, especially with reconstructive procedures, therefore, 5 mm extra port was added in three patients of LESS pyeloplasty and one patient of LESS repair of retrocaval ureter. However, the difference in the operative time was not statistically significant between the two groups.
Since the introduction of LESS as an alternative minimally invasive option in the field of urology, there have been many studies stating the cosmetic and reduced pain benefit of LESS over CL for multiple urologic procedures. 7,18,21,25,26 Also, Al Nasser and colleagues reported the cosmetic superiority of the ML retroperitoneoscopic pyeloplasty when compared with the standard equivalent with no higher complication rate. 28 In our study, LESS group of patients were superior to ML group, regarding the cosmetic outcome and postoperative pain. Many scales for assessment of scars are available, such as Manchester scar scale and Vancouver scar scale, and also matching assessment of scars and photographs. 29 However, the PSAS and OSAS are the most frequently used scales for assessment of scars. 13 We used both the PSAS and OSAS for postoperative scar assessment in our study. In their study, Al Nasser and colleagues used only the OSAS for scar assessment. It seems that the site of insertion of the single port in LESS through the umbilicus, which is a natural scar, results in a concealed scar that may be more accepted than multiple transabdominal scars, even if they are small ones. Also, with ML, there was inevitable need to insert ports larger than 3 mm; especially in ablative procedures to apply clips. This was justified according to Porpiglia et al. who reported a liberal use of standard (larger) trocars and instruments in ML extirpative surgeries. 10 This may reflect the need of overcoming the current shortcoming of ML instrumentation.
Overall, each access has its own technical difficulties and limitations. ML instruments are weak and tend to bend especially when exerting counter traction while dissecting large masses. Furthermore, the 3 mm laparoscope has a significantly limited and poor-quality field of vision. Moreover, in case of bleeding, the illumination-induced light absorption causes a substantial decrease in image quality. The necessity of adding 10 mm port in ablative procedures makes ML probably more applicable to reconstructive urologic procedures. While doing suction or desmoking, the flow is weak as the 3 mm trocar just admits the 3 mm instrument, and the caliber of 3 mm suction tube is relatively small and has weak flow. On the contrary, with LESS, difficulties were mainly related to its inherent technical limitations that are related to the lack of triangulation and loss or ergonomics especially with reconstructive procedures. Also, although it was not studied, LESS seems to be more costly than ML due to the disposable ports and instruments of LESS.
Our study still has some limitations. First, the number of the patients in each cohort may not be too large, and certain indications may need more patients. The results represent the experience of a surgeon with extensive laparoscopic background both in LESS and CL, therefore transferring the results in a different setting should be carefully considered. However, to the best of our knowledge, this is the first prospective randomized study to compare between LESS and ML, which are regarded as minimally invasive alternative to CL. The current study represents a single-center single-surgeon experience, which excludes the heterogeneity of the evaluation parameters and gives a solid conclusion about the feasibility, safety advantages, and disadvantages of each technique.
Conclusion
This prospective randomized study demonstrates that both LESS and ML are feasible and safe options for treatment of different upper urinary tract pathologies with comparable operative time, blood loss, hospital stay, and complication rate.
LESS is associated with less postoperative pain, less analgesic requirement, and better cosmetic outcome. However, each procedure has its technical difficulties and limitations.
Footnotes
Author Disclosure Statement
No competing financial interests exist.