
Abstract
Background:
Small series have reported that cryoablation (CA) is a safe and feasible minimally invasive nephron-sparing alternative for the treatment of renal angiomyolipomas (renal AMLs). The aim of the present study was to investigate the safety and efficacy of CA in patients with renal AML.
Materials and Methods:
A retrospective review of 19 renal AML lesions treated with CA at Aarhus University Hospital, Denmark, over a 5-year period.
Results:
The treatment was performed as laparoscopy-assisted CA on 7 lesions, and in the remaining 12 lesions CA was performed as a percutaneous ultrasound-guided CA. The mean patient age was 46 years [interquartile range (IQR) 30] and the mean tumor volume was 50.1 cm3 (IQR 53.3). In all cases, the procedure was effectively conducted with no conversion to open surgery, and no major complications were experienced. The mean follow-up time was 25 months (IQR 13). Mean maximum tumor volume was reduced from 50.1 cm3 (IQR 53.3) to 12.2 cm3 (IQR 14.1), p = 0.05. No patients presented with retroperitoneal hemorrhage or recurrence during follow-up.
Conclusion:
Treating renal AMLs with CA appears to be a safe and effective nephron-sparing approach and could be a valuable alternative to other treatment modalities. The low complication rate, absence of retreatment and a good preservation of renal function might allow treatment of even subclinical renal AMLs to minimize the risk of potentially life-threatening hemorrhage.
Introduction
R
Due to the unique radiographic characteristics of the lesions, the diagnosis of classic AMLs approaches 100% sensitivity with a combination of CT and ultrasound. 6,9 Epitholoid AML, which is composed of numerous atypical epithelioid muscle cells and contain few or no fat cells, are unlike classic AMLs potentially malignant. 1,10 Biopsy or multiparametric MRI (mpMRI) are essential for distinguishing epitholoid AMLs from other tumors, for example, renal cell carcinoma. 11
Renal AMLs may course flank pain, hematuria, filling in the abdomen, and spontaneous retroperitoneal bleeding. This has been reported in 15% of patients and may lead to circulatory shock in up to 20%–30% of these patients. 5,7,8 The treatment of renal AML is focused on nephron-sparing modalities such as partial nephrectomies (PN), renal angioembolization (RAE), or ablative therapies, for example, cryoablation (CA) or radiofrequency ablation (RFA). 6,7,12 –14
For the treatment of renal AMLs, CA has only been reported in two previous studies with a limited number of patients and short-term follow-up. 15,16 The aim of the present study is to evaluate the safety and efficacy of CA in patients treated for renal AMLs.
Materials and Methods
Patients and materials
With approval from the Danish National Health and Medicines Authority, a review of a prospectively maintained clinical database was performed to identify patients with renal AML who were treated with primary CA over a 5-year period at Aarhus University Hospital, Denmark. In all, 16 patients with a total of 19 treated lesions were identified. All medical records and images were retrospectively reviewed to collect detailed information regarding patient demographics, comorbidity, renal status, histology, procedure details, and postoperative follow-up. Patient characteristics are presented in Table 1.
IQR = interquartile range.
CA techniques
Treatment was performed as either ultrasound guided percutaneous cryoablation (PCA) (n = 12) or laparoscopy-assisted cryoablation (LCA) (n = 7). The decision to use LCA or PCA was based on an individual evaluation of tumor location and proximity to thermosensitive structures such as intestine, pancreas, and the pleura sinus.
In the PCA procedure, an endoscopic ultrasound (4-Way Laparoscopic 8666-RF; Analogic BK, Herlev, Denmark) was used for lesion identification, probe placement, and monitoring of the freezing process. A highly experienced interventional radiologist performed all the PCA procedures. The LCA procedure consisted of a standard three-port transperitoneal laparoscopic approach. Endoscopic ultrasound was used for tumor identification, probe placement, and monitoring of the freezing process.
An argon-/helium-based cryosystem (SeedNet and later Visual Ice; Galil Medical, Arden Hills, MN) with 17-gauge (1.47 mm) cryoprobes were used for both PCA and LCA. All lesions were treated with a standard double freeze–thaw cycle of 10-minute freeze, 8-minute thaw, and 10-minute freeze. Both procedures were performed under general anesthesia.
In contrast to standard tumor ablation, cryoprobe placement was arranged differently in these procedures. In standard tumor ablation cryoprobes are placed inside the tumor to create an ice ball covering the entire tumor, but for the treatment of renal AMLs the cryoprobes are placed between the lesion and normal renal parenchyma to interrupt the lesions connection with normal renal parenchyma and thus interrupt the blood supply. After removal of the cryoprobes, seeping bleeding from the puncture site was treated with application of the hemostatic agents TachoSil (Baxter International, Inc., Deerfield, IL) and Perclot (CryoLife, Inc., Kennesaw, GA).
Postoperative follow-up
The follow-up included assessment of the renal function by measurement of serum creatinine (s-Cr), estimated glomerular filtration rate (eGFR) levels, and radiologic assessment of changes in renal AML volume, either by magnetic mpMRI ultrasound or CT. Dependent on an individual medical assessment and the postoperative volume of the renal AML, patients underwent individualized follow-up regimes. A senior radiologist with 7 years' subspecialized uroradiologic experience (O.G.) evaluated all images. Preoperative tumor categorization and postoperative cryolesion's size, shape, and contrast enhancement patterns were measured in three levels; anterior–posterior, lateral–medial, and cranial–caudal. To compare whether the renal AML increased or decreased in size during follow-up, the volume was calculated by assuming that they adhered to a circular shape. When evaluating the postoperative outcomes, the radiologist had access to compare the follow-up images with the preoperative diagnostic images. Regarding postoperative complications, patients were classified according to the Clavien–Dindo classification.
Results
A total of 19 lesions in 16 patients were effectively treated using CA. None of the procedures resulted in conversion to open surgery or the need of retreatment.
The mean age was 46 years [interquartile range (IQR) 30], the mean tumor volume was 50.1 cm3 (IQR 53.3), and mean maximal tumor diameter was 4.7 cm (IQR 2.6). Four patients were diagnosed with TSC. All patients had normal preoperative s-Cr and eGFR levels. Treatment indications were as follows: risk of hemorrhage (n = 14), pain (n = 3), retroperitoneal hemorrhage (n = 1), and hematuria (n = 1). The mean operation time was 117 minutes (IQR 30) and the mean length of hospital stay (day of surgery not included) was 1.6 days (IQR 1). The mean follow-up time was 25 months (IQR 13). One patient with a single renal AML was lost to follow-up due to relocation (lesion 16). Postoperative s-Cr and eGFR revealed normal renal function in all patients with no significant difference compared to preoperative levels. Mean maximum tumor volume was reduced from 50.1 cm3 (IQR 53.3) to 12.2 cm3 (IQR 14.1), p = 0.05.
There were no major postoperative complications (defined as a Clavien–Dindo score ≥3). A total of 13 patients (treated for 15 lesions) scored 0, one patient (lesion 19) scored 2, and one patient with two lesions (lesions 6 and 7) scored 1. Intra- and postoperative complications are presented in Table 2.
LCA = laparoscopy-assisted cryoablation; PCA = percutaneous cryoablation.
Discussion
In this study, we presented a total of 19 renal AML lesions in 16 patients with a mean age of 46 years. All lesions were treated with either PCA or LCA. Figure 1 shows classic AML before and after treatment while figure 2 shows epitholoid AML also before and after treatment. The procedure was well tolerated in all cases. Minor complications were seen in only a few cases and a significant reduction in tumor size was found. With the prevention of hemorrhage and a good preservation of renal function supports the use of minimal invasive CA in these patients.
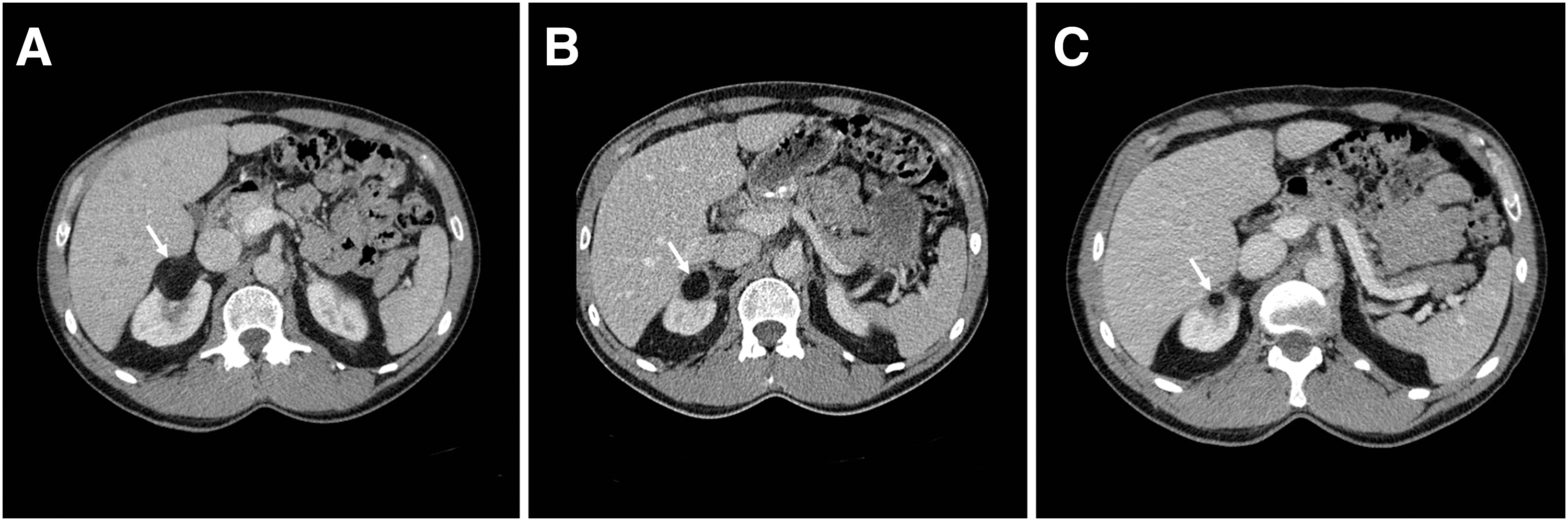
White arrows show Classic AML:

White arrows show Epitholoid AML:
The primary indication for treatment of renal AML is either presence of symptoms, risk of bleeding, or suspected malignancy. 2,17,18 The epitholoid AMLs are, because of their imaging characteristics, difficult to distinguish from malignant suspected lesions, and in these cases biopsy or mpMRI may aid in clinical decision-making. 11,12,18 In the present study, 11 lesions were biopsied and analyzed for their composition of large numbers of hyperplastic epithelioid cells arranged in sheets. It is well known that epitholoid AMLs are associated with a worse treatment and survival outcome compared with classic AMLs, but the present cohort was too small for us to investigate this aspect when treated with CA. 19,20
Renal angioembolization is often the first-line of treatment for patient with renal AMLs. 14,21 Regrowth and repeated hemorrhage after embolization, however, remains a concern. 2,14,21 Ramon and colleagues presented in their study a need for reembolization in 37% of the cases and a minor complication rate of 16% during the 30 days following RAE. 2 In comparison, Bardin and colleagues showed in their series a need for reembolization in 17% of the cases and a renal AML recurrence rate of 13%. Major complications were reported in 13 patients and minor postembolization syndrome in 61% of the cases. The mean size of asymptomatic renal AML before RAE was 8.9 and 12.4 cm for symptomatic renal AML. The mean renal AML size reduction rate was only 26% after a mean follow-up time of 21 months. 22 Kuusk and colleagues found that the 3-year rate of freedom from reintervention after embolization to be 63.5% and concluded that among treatment modalities, RAE was associated with a significant higher risk of reintervention. 18 This is to be compared with no need for reintervention, a minor complication rate of only 5.5% and a mean renal AML size reduction rate of 75.6% found in the present study. RAE might presumably be less costly, but with above mentioned recurrence rates and complication rate CA seems to be a promising alternative to RAE. It would be ideal to investigate this further with a randomized controlled trial that analyzes the outcomes and costs of CA compared to RAE.
Among other nephron-sparing treatments Castle and colleagues presented a study consisting of 15 cases with a mean tumor size of 26 mm, that was treated effectively using RFA. Their treatment has no need for reintervention and no radiographic recurrences at a mean follow-up of 21 months while reporting a complication rate of 13.3%. 23 These findings are in concordance with Prevoo and colleagues and Kuusk and colleagues who reported the same findings for RFA treatment of renal AMLs with a tumor diameter of 39 mm. 14,18
Another treatment for renal AML is PN and total renal nephrectomy (RN). Berglund and colleagues reported a series of 44 patients treated with PN for renal AML with a median diameter of 28 mm and found a 23% complication rate, 14% loss of a renal unit and six patients (16%) with new onset of chronic kidney disease. 23,24 These findings were supported by Msezane and colleagues. 21
In the present series, all patients were treated with either PCA or LCA. When the cryoablative modality initially was introduced in renal tumor treatment, it was generally performed as a laparoscopy-assisted procedure, which allowed a safe mobilization of fragile organs, for example, colon and the ureter. Furthermore, laparoscopy-assisted procedures allowed for a direct visualization of any hemorrhage and the opportunity to control this without the formation of a large hematoma. In recent years, the modality has changed toward a CT-guided procedure with the option to perform hydro- or gas-dissection in case fragile organs are in a close proximity of the tumor. Compared with laparoscopy-assisted procedures, a CT-guided procedure is generally considered less invasive, and in some well selected cases it can even be performed in local anesthesia. One major advantage of CT-guided procedures is the ability to visualize the extension of the ice ball, which can be difficult when using traditional or laparoscopy-assisted ultrasound. In our institution, all CA is now being performed as CT-guided procedure, but as of yet, no randomized study exists comparing surgical vs image-guided ablative procedures with regard to complications and outcomes.
Byrd and colleagues reported the first study of seven adult patients with renal AML, who were all effectively treated with CA. 15 At follow-up, renal function was normal, and follow-up imaging revealed a tumor size reduction in all patients. Three complications occurred in two patients. One patient sustained a superficial liver laceration during port placement, and one had a CT-confirmed perinephric hematoma and incidentally identified small pneumothorax and pneumomediastinum. Johnson and colleagues presented a study of just three patients treated for renal AML using PCA. 16 They concluded that the modality was safe and effective when treating these lesions. Their patients experienced minimal to no pain during treatment and all were discharged the same day with no procedural or postoperative complications. These results are all in concordance with the findings of the present study. Trelborg and colleagues reported recently a study of eight renal AMLs in adolescents with a median lesion size of 39 mm and a postoperative follow-up time of 37 months. All lesions were effectively treated using LCA, supporting the safety and efficacy of CA. 3
Major hemorrhage is the most severe complication of renal AML, and prophylactic treatment may be indicated to avoid this. In the present study, all 18 cases of renal AMLs were treated effectively with CA. The procedure-specific complication rate was 5.5% with only one incident of “cracking” of the tumor surface. The prediction of major hemorrhage events associated with renal AML is an important clinical issue and often dictates a prophylactic treatment strategy. The traditional prophylactic treatment threshold is 4 cm as the risk of bleeding is associated with larger tumor diameter. With respect to CA, we did not have an upper limit on tumor size as seen by the variation in tumor size in the present series. Kuusk and colleagues showed in their latest analysis that the prevalence of major hemorrhage is significantly higher in renal AMLs larger than 6 cm in diameter and concluded that conservative treatment can be considered for renal AMLs <6 cm in diameter, whereas a threshold for invasive treatment of 4 cm may not be appropriate. 18 In the present series, minor bleeding from where the cryoprobes were inserted into the tumor was seen in five lesions, which is expected but this complication may be a significant concern if larger AMLs were to be treated, as larger tumors generally demand a larger number of cryoprobes. The present series was too small to allow for an estimation of a potential threshold for the treatment of renal AMLs with CA and long-term follow-up is necessary to assess true treatment efficacy. 18,25,26
When comparing current methods for treating renal AMLs, CA appears to be an attractive alternative to RAE or PN. RAE carries a risk of recurrence, hemorrhage, and postembolization syndrome. 23 PN has a significant conversion rate to RN when operating on renal AMLs. 18,23,24 RFA showed a low complication rate and promising efficacy. 18,23 CA appears to have a favorable complication profile and a good preservation of renal function. We have demonstrated with the present study, and existing data on CA, that the modality appears to be a safe and efficient long-term minimal invasive treatment for patients with renal AML.
Renal AMLs associated with TSC or lymphangioleiomyomatosis may not be amenable to surgery or ablative therapy due to their multiplicity and bilateral presentation. Oral mammalian target of rapamycin (mTOR) inhibitors have been evaluated for the management of AML in these patients. 27 Follow-up data from the EXIST-2 study showed that 81.6% of patients with TSC achieved AML reductions of ≥30%, and 64.5% achieved AML reductions of ≥50% following 96 weeks of treatment with the mTOR inhibitor everolimus. 28,29 The study concluded that longer term everolimus treatment appeared safe and effective in patients with TSC- or sporadic lymphangioleiomyomatosis-associated renal AML not requiring surgical intervention. 28
Limitations to the present study include the retrospective and nonrandomized design, thus introducing the risk of selection bias. The number of treated lesions was limited to only 19 lesions, which limits the study's ability to perform a direct comparison between LCA and PCA, despite the practical difference between the two modalities. A randomized controlled trial that analyzes the outcomes of CA compared with other treatment modalities, for example, RAE, would be ideal and should be performed.
Conclusion
Treating renal AMLs with CA appears to be a safe and effective nephron-sparing approach and could be a valuable alternative to other treatment modalities. The low complication rate, absence of retreatment, and a good preservation of renal function might allow treatment of even subclinical renal AMLs to minimize the risk of potentially life-threatening hemorrhage.
Footnotes
Acknowledgments
The authors thank Dr. John Denstedt and those who edited the paper.
Author Disclosure Statement
No competing financial interests exist.