
Abstract
Introduction:
To date, the ergonomics of flexible ureteroscopy (URS) have not been well described. We performed a study to assess the biomechanical stresses on urologists performing URS and to investigate the effect of ureteroscope type on these parameters.
Methods:
Electromyography (EMG) was used to quantify the activation level of muscle groups involved in URS. Surface EMG electrodes (Delsys, Boston, MA) were placed on the right and left thenar, flexor carpi ulnaris (FCU), extensor carpi ulnaris (ECU), biceps, triceps, and deltoid. Three endoscopes were studied: single-use digital (Boston Scientific LithoVue), reusable digital (Karl Storz Flex-Xc), and reusable fiber-optic (Karl Storz Flex-X2). Each ureteroscope was used to perform a set sequence of navigation and procedural tasks in a training model. EMG data were processed and normalized to compare the maximum voluntary contractions between muscle groups. Cumulative muscular workload (CMW) and average muscular work per second (AWS) were used for comparative analysis.
Results:
For navigational tasks, CMW and AWS were greatest for the ECU, followed in descending order by right and left thenar, FCU, biceps, deltoid, and triceps. For procedural tasks, CMW and AWS were greatest for the right thenar, followed in descending order by the left thenar, ECU, FCU, triceps, biceps, and deltoid. During navigational tasks, both LithoVue and Flex-Xc had lower CMWs for every muscle group than Flex-X2 (p < 0.05). LithoVue and Flex-Xc had similar AWS and both were lower than Flex-X2 for the right thenar, ECU, biceps, and deltoid activation (p < 0.05). During procedural tasks, both LithoVue and Flex-Xc had lower CMWs and AWS for right and left thenar, ECU, and biceps than Flex-X2 (p < 0.05).
Conclusions:
This study provides the first description of EMG-measured ergonomics of URS. Both the single-use and reusable digital ureteroscopes have similar profiles, and both have significantly better ergonomic metrics than the reusable fiber-optic ureteroscope.
Introduction
T
Despite its increasingly common use, the ergonomics of URS have not been well described. A better understanding of the biomechanical stresses placed on the body during performance of URS is critical to identify factors that may contribute to surgeon fatigue and discomfort, so that ultimately such factors may be mitigated, thereby preventing injury and maximizing efficiency. In addition, as there are multiple types of flexible ureteroscopes currently available to the surgeon (reusable fiber-optic, reusable digital, single-use digital), a better ergonomic characterization of the effects of these various ureteroscope designs will further broaden our understanding of URS ergonomics as a whole.
Therefore, we performed a study to investigate the biomechanical stresses, as measured by surface electromyography (EMG), on the urologist performing URS. In addition, we compared the ergonomic profiles of a reusable fiber-optic ureteroscope (Karl Storz Flex-X2), a reusable digital ureteroscope (Karl Storz Flex-Xc), and a single-use digital ureteroscope (Boston Scientific LithoVue).
Methods
Surface EMG was used to quantify the activation levels of the surgeon's muscle groups used in a URS procedure. EMG detects the electric potential generated by muscle cells and creates an electromyogram that can be analyzed to determine activation level and other biomechanical factors. Seven surface EMG electrodes (Delsys, Boston, MA) were placed on specific muscle beds before URS task initiation. Electrodes placed on the right and left thenar eminence measured muscle activation associated with deflection control and flexible tip manipulation. Electrodes placed on the flexor carpi ulnaris (FCU) and the extensor carpi ulnaris (ECU) measured activation of wrist flexion and extension, respectively. Additional EMG sensors were placed on the biceps, triceps, and deltoid to measure forearm flexion, extension, and shoulder movements, respectively. An example of surface EMG electrode placement can be seen in Figures 1 and 2.

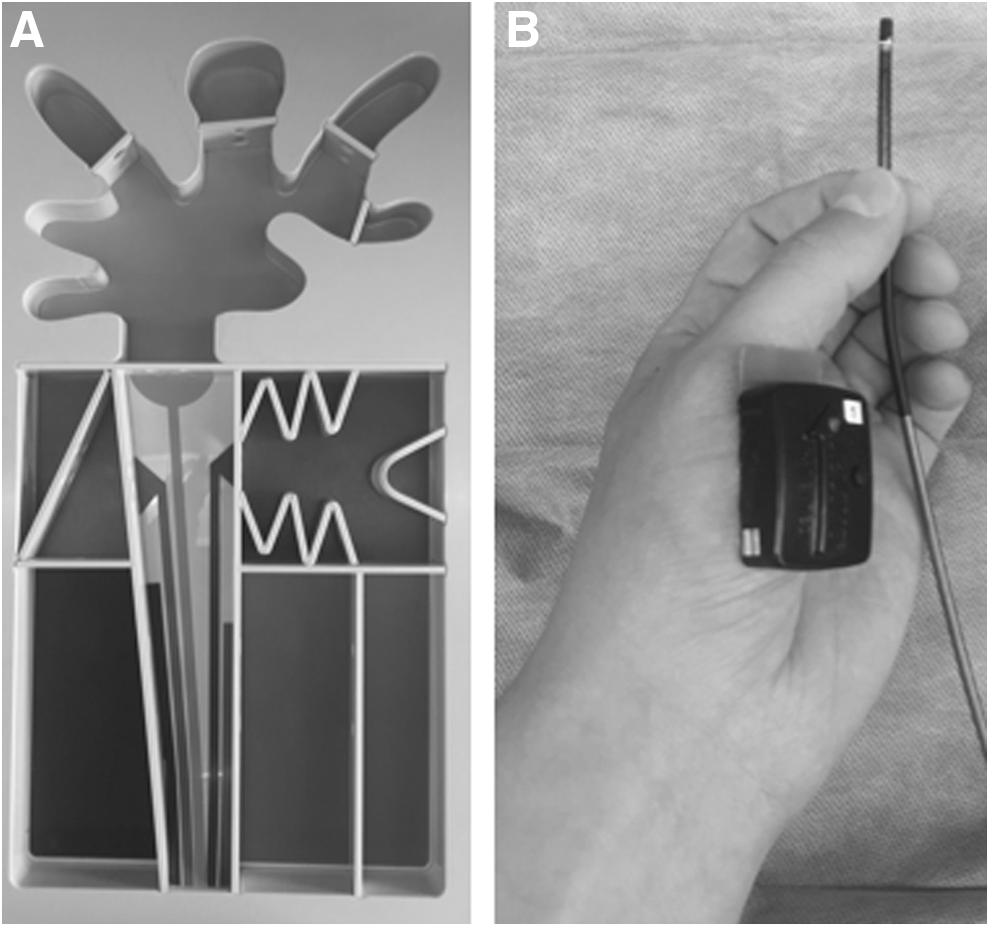
(
Navigational and procedural URS tasks were performed. For navigational tasks, a set sequence of objectives was performed in the Stone Institute Flexible URS Trainer (Boston Scientific) under direct vision (LithoVue n = 10, Flex-Xc n = 10, Flex-X2 n = 8), as seen in Figure 2. These tasks involved sequential inspection of nine distinct chambers and passage through eight 1.0-cm channels and two 0.5-mm channels. Procedural tasks included inspection under direct vision of two calices in the model; each calix contained a 0.5 × 0.5 mm diamond-shaped stone imitation (LithoVue n = 8, Flex-Xc n = 8, Flex-X2 n = 8). A 1.9F tipless Nitinol stone retrieval basket was deployed for the purpose of capturing the stone and an Amplatz super stiff wire was placed in the second calix as would be performed during a clinical URS procedure.
Three endoscopes were used: single-use digital (Boston Scientific LithoVue), reusable digital (Karl Storz Flex-Xc), and reusable fiber-optic (Karl Storz Flex-X2). Ureteroscopes were used in an alternating manner during tasks, to minimize the effects of fatigue on a particular ureteroscope type. There was a short break between tasks and navigational and procedural trials were performed during separate encounters. Tasks were performed by a right-handed senior urology resident at a tertiary medical center that performs high-volume URS, to provide internal consistency across ureteroscopes. Data collection and analysis were similar to previous reports from our institution. 3 Maximum voluntary contraction (MVC) levels for each muscle were recorded to normalize activation data according to maximal muscle contraction. EMG recordings were collected at 1000 Hz to normalize activation levels between muscle groups. Each recording was full-wave rectified by removing the mean value, obtaining the absolute value of contractions and calculating the root mean square. The rectified EMG data were then divided by MVC and displayed as %MVC. The %MVC was adjusted by the time integral of data to calculate cumulative muscular workload (CMW). The average muscular work per second (AWS) was calculated by dividing CMW by the performance time. Continuous variables were compared using one-way ANOVA or paired t-tests. All analyses were performed using R, version 3.1.2. A p-value <0.05 was considered statistically significant.
Results
Navigational tasks
The median time for task completion was 77.3 ± 16.7, 73.3 ± 11.8, and 104.7 ± 23.5 seconds for LithoVue, Flex-Xc, and Flex-X2, respectively. Median task completion time was similar for the LithoVue and Flex-Xc ureteroscopes and significantly longer for the Flex-X2 ureteroscope (p = 0.01). Muscular activation, as measured by highest CMW and AWS, was greatest for ECU, followed in descending order by the right and left thenar, FCU, biceps, deltoid, and triceps. As seen in Tables 1 and 2, both LithoVue and Flex-Xc had lower CMWs for every muscle group than Flex-X2 (p < 0.05). In addition, biceps CMW was significantly lower for the LithoVue ureteroscope than for the Flex-Xc ureteroscope (p = 0.01). LithoVue and Flex-Xc ureteroscopes had similar AWS and both were lower than the Flex-X2 ureteroscope for the right thenar, ECU, biceps, and deltoid activation (p < 0.05). In addition, LithoVue had higher AWS for right thenar and lower AWS for biceps than Flex-Xc (p < 0.05).
ECU = extensor carpi ulnaris; FCU = flexor carpi ulnaris.
Procedural tasks
The median time for task completion was 75.8 ± 12.9, 76.8 ± 11.4, and 87.5 ± 21.1 seconds for LithoVue, Flex-Xc and Flex-X2 ureteroscopes, respectively. Median task completion time was similar for LithoVue and Flex-Xc ureteroscopes and trended toward longer for the reusable Flex-X2 ureteroscope (p = 0.17). For the LithoVue and Flex-Xc ureteroscopes, CMW and AWS were greatest for the right thenar, followed in descending order by left thenar, ECU, FCU, triceps, biceps, and deltoid. The Flex-X2 ureteroscope was similar; however, biceps were more activated than triceps. As seen in Tables 3 and 4, both LithoVue and Flex-Xc had lower CMW and AWS for right and left thenar, ECU, and biceps muscle group than Flex-X2 (p < 0.05). In addition, biceps CMW and AWS were significantly lower for LithoVue than for Flex-Xc (p = 0.01).
Discussion
We used surface EMG during navigation and procedural tasks to assess biomechanical stresses associated with URS and compared these stresses among commonly used ureteroscopes. For navigational tasks, the ECU and thenar muscles were most activated, whereas the deltoid and triceps muscles were the least activated. Activation across all muscle groups was lower for LithoVue and Flex-Xc than for Flex-X2. For procedural tasks, the right and left thenar were the most activated muscle groups, whereas the biceps, triceps, and deltoid were the least activated muscle groups. Right and left thenar, ECU, and biceps activation were lower for LithoVue and Flex-Xc than for Flex-X.2
An understanding of the ergonomics of URS is important, particularly as surgeon's occupational health is increasingly emphasized. 4 Endoscopic ergonomics have been studied in a variety of settings by surface EMG, such as colonoscopy and laryngoscopy. 5,6 Various body positions during laryngoscopy have been analyzed and a more favorable ergonomic stance was found to decrease muscle activation and pain while increasing surgical productivity. 7 Thus, knowledge of muscle activation levels during endoscopy can lead to alterations in performance that facilitate surgical improvements. In terms of urologic procedures, surface EMG was used to study the difference between direct and video-guided transurethral resections and found that video guidance reduced muscular strain and fatigue. 8 –10 Following these studies, the adoption of video guidance during transurethral resection has been an important factor in reducing urologists' muscular fatigue. With regard to URS, a previous study administered questionnaires to high-volume surgeons concerning the ergonomics of URS and found surprisingly poor characteristics. 7 Mean general ergonomic complaints were rated at three out of five, and upper extremity and hand pain consistently scored the highest complaint level. Our data corroborate this finding, with the highest activation levels belonging to the thenar muscles and ECU. ECU levels were higher during navigational tasks, likely because of increased ureteroscope positional changes compared with procedural tasks. Understanding which muscles have the highest activation levels may prompt urologists to conserve use of those muscle groups during particularly taxing ureteroscopic cases. Future studies may compare various techniques to determine ergonomically favorability, possibly decreasing muscular fatigue and increasing productivity.
In the modern landscape, there are numerous flexible ureteroscopes available to urologists. When choosing a ureteroscope, there are many factors to consider. Fiber-optic ureteroscopes last only 15 passes before breaking a significant number of optical fibers and typically require costly repairs in fewer than 30 uses. 11,12 Ureteroscope functionality comparison studies have found LithoVue, Flex-Xc, and flexible fiber-optic ureteroscopes to have similar optics, deflection, and flow. 13 Multiple studies have found reduced operative times using both reusable and disposable digital ureteroscopes than when using fiber-optic ureteroscope. 14,15 Indeed, a recent prospective case–control study comparing LithoVue with a reusable flexible fiber-optic ureteroscope found that cases using LithoVue were on average 10 minutes shorter. 16 The authors note that the etiology of this finding is not understood, but speculate that it is because of LithoVue being lighter and easier to flex than reusable fiber-optic ureteroscopes. Our study may provide data supporting this claim—there is significantly less muscle activation and thus fatigue associated with LithoVue.
Broadly speaking, ergonomics should be a factor to consider when choosing a ureteroscope. Across muscle groups, digital ureteroscopes were consistently superior to the fiber-optic ureteroscopes; this is likely because of differences in ureteroscope weight—with LithoVue being the lightest, followed by Flex-Xc and then Flex-X2. In addition, as Flex-X2 is not digital, it requires use of a separate camera, which adds substantial weight. This relationship could be seen particularly in navigational tasks, in which biceps activation was greatest for Flex-X2, followed by Flex-Xc and then LithoVue. With decreasing ureteroscope weight, less forearm flexion is required. We found shorter task duration for the digital ureteroscopes, which may be because of ease of use and less fatigue. This finding is in agreement with a number of studies that compared digital and fiber-optic ureteroscopes in a clinical setting. 14 –16
Perhaps the greatest limitation of this study is its in vitro nature. In our protocol, we measured muscular activation during predetermined navigational and procedural tasks that were designed to mimic clinical maneuvers performed during an actual surgical procedure. The Stone Institute trainer replicates many aspects of URS, but there are some components of the simulation, such as navigation from the bladder into the ureteral orifice that are not precisely replicated. It is possible that the ergonomic measurements of real-time URS procedures may reveal a different profile. Such an analysis would be an important next study, building on the foundation created herein. Future studies may be designed to capture real-time EMG measurements during actual URS clinical cases to identify specific steps associated with a poor ergonomic profile. This may aid urologists in improving ergonomics, allowing URS to become more comfortable, safe, and efficient.
Conclusions
This study provides the important first description of the ergonomics of URS as measured by surface EMG. The thenar and ECU are the most activated muscle groups, whereas the biceps and deltoid are the least activated. Digital ureteroscopes, in this case LithoVue and Flex-Xc, have similar profiles during navigational and procedural tasks, and both have significantly better ergonomic metrics than the fiber-optic ureteroscope that was evaluated.
Footnotes
Author Disclosure Statement
No competing financial interests exist.