
Abstract
Introduction:
We present our experience with a novel three-layer two-step posterior reconstruction (PR) technique using peritoneum during robot-assisted radical prostatectomy (RARP) to improve recovery of postoperative urinary continence.
Methods:
Forty-eight patients with localized prostate cancer were enrolled in this study and were divided randomly into two groups, which were treated by the standard PR technique (standard PR group; n = 24) or the three-layer PR technique using peritoneum (three-layer PR group; n = 24) during RARP. We prospectively analyzed the continence rate by the 1-hour pad test. All patients underwent urethrocystography at 6 days postoperatively to evaluate position of vesicourethral junction. Pelvic MRI was also performed at 6 months postoperatively for anatomical evaluation.
Results:
Four weeks after RARP, the urinary continence rate was significantly higher in the three-layer PR group (57%) than in the standard PR group (26%, p = 0.036). Urethrocystography demonstrated that the postoperative craniocaudal distance from the symphysis pubis to the level of the vesicourethral junction was significantly shorter in the three-layer PR group than in the standard PR group (p < 0.01), suggesting that there was less tension on the vesicourethral anastomosis after three-layer PR. MRI confirmed that three-layer PR provided firmer reinforcement of the structures, supporting the posterior aspect of the urethral sphincter complex.
Conclusions:
This prospective comparative study might suggest that three-layer two-step PR using peritoneum during RARP is a simple and feasible method seeming to improve early recovery of postoperative continence compared with standard two-step PR, although larger multicenter randomized controlled trials will be needed.
Introduction
R
Numerous techniques to improve postoperative recovery of urinary continence after radical prostatectomy have been reported. 1 –10 Posterior reconstruction (PR) is one of the most common procedures for improving recovery of continence, and several modifications of this procedure have been reported. 11 –18 This technique aims to restore posterior support by reapproximation of the transected musculofascial plate (rhabdosphincter) posterior to the urethra and the cut edge of Denonvillier's fascia, and to make it easier to perform subsequent vesicourethral anastomosis under less tension. 11 –20 We considered that further reinforcement of posterior support and less tension on the vesicourethral anastomosis might lead to earlier return of continence after prostatectomy, and developed a new modification of the PR technique. In this study, we present our experience with this modified technique (three-layer two-step PR using peritoneum) in patients undergoing RARP and evaluate its efficacy for improving continence after RARP in comparison with the standard PR technique.
Materials and Methods
Forty-eight patients (median age: 68.5 years) with localized prostate cancer who visited Fukushima Medical University Hospital from April to September 2013 were enrolled in this study. Inclusion criteria were (1) clinically localized prostate cancer (T1c or T2), (2) age <75 years, and (3) Eastern Cooperative Oncology Group performance status of 0. Exclusion criteria were a history of urethral stricture, neurogenic bladder, previous prostate surgery, interstitial cystitis, or pelvic radiation. The patients underwent RARP by a single surgeon (Y.K.), who had experience of more than 200 RARP procedures, before designing the study. Before surgery, the patients were randomly divided into two groups at a 1:1 ratio, which were treated by the standard two-layer two-step PR technique (standard PR group; n = 24) or the new three-layer two-step PR technique using peritoneum (three-layer PR group; n = 24). Patients were blinded to their grouping, while the surgical team was only notified of the group after completion of prostatectomy. This study was approved by the Ethics Committee of our institution. Informed consent was obtained from all patients, after explaining the purpose and methods of the study.
In all patients, RARP was performed by the transperitoneal posterior approach reported by Guillonneau and Vallancien in conventional laparoscopic procedures. 21 This approach is initiated with transverse peritoneotomy between the bladder and rectum, followed by retrovesical dissection. The posterior part of the incised peritoneum between the bladder and the rectum was subsequently used for three-layered two-step PR technique (Fig. 1).

Transverse peritoneotomy between the bladder and rectum for the posterior approach to transperitoneal RARP. The posterior part of the incised peritoneum between bladder and rectum (arrows) is used for three-layer two-step PR. PR = posterior reconstruction; RARP = robot-assisted radical prostatectomy.
PR was performed before vesicourethral anastomosis. The standard PR technique involved two-layer PR using 3–0 barbed suture (V-Loc™ Absorbable Wound Closure Device; Covidien, Mansfield, MA). The first layer was created by apposition of the transected musculofascial plate (rhabdosphincter) posterior to the urethra with the cut edge of Denonvillier's fascia located halfway between the bladder and the urethra. The second layer was created by apposition of the rhabdosphincter just below the urethra with the posterior wall of the bladder about 2 cm dorsocephalad to the new bladder neck (posterior counterpart of the detrusor apron). In the three-layer two-step PR technique, 3–0 barbed suture was passed (1) through the posterior peritoneum incised between the bladder and the rectum described above, (2) through the cut edge of Denonvillier's fascia, and (3) through the transected musculofascial plate (rhabdosphincter) posterior to the urethra (first and second layers). (4) Then, the suture was passed through the retrotrigonal layer close to the bladder neck (third layer). As a result, the posterior part of the incised peritoneum completely covered Denonvillier's fascia, and this three-layer structure acted as a support for vescicourethral anastomosis (Figs. 2 and 3). (Supplementary Video SV1; Supplementary Data are available online at
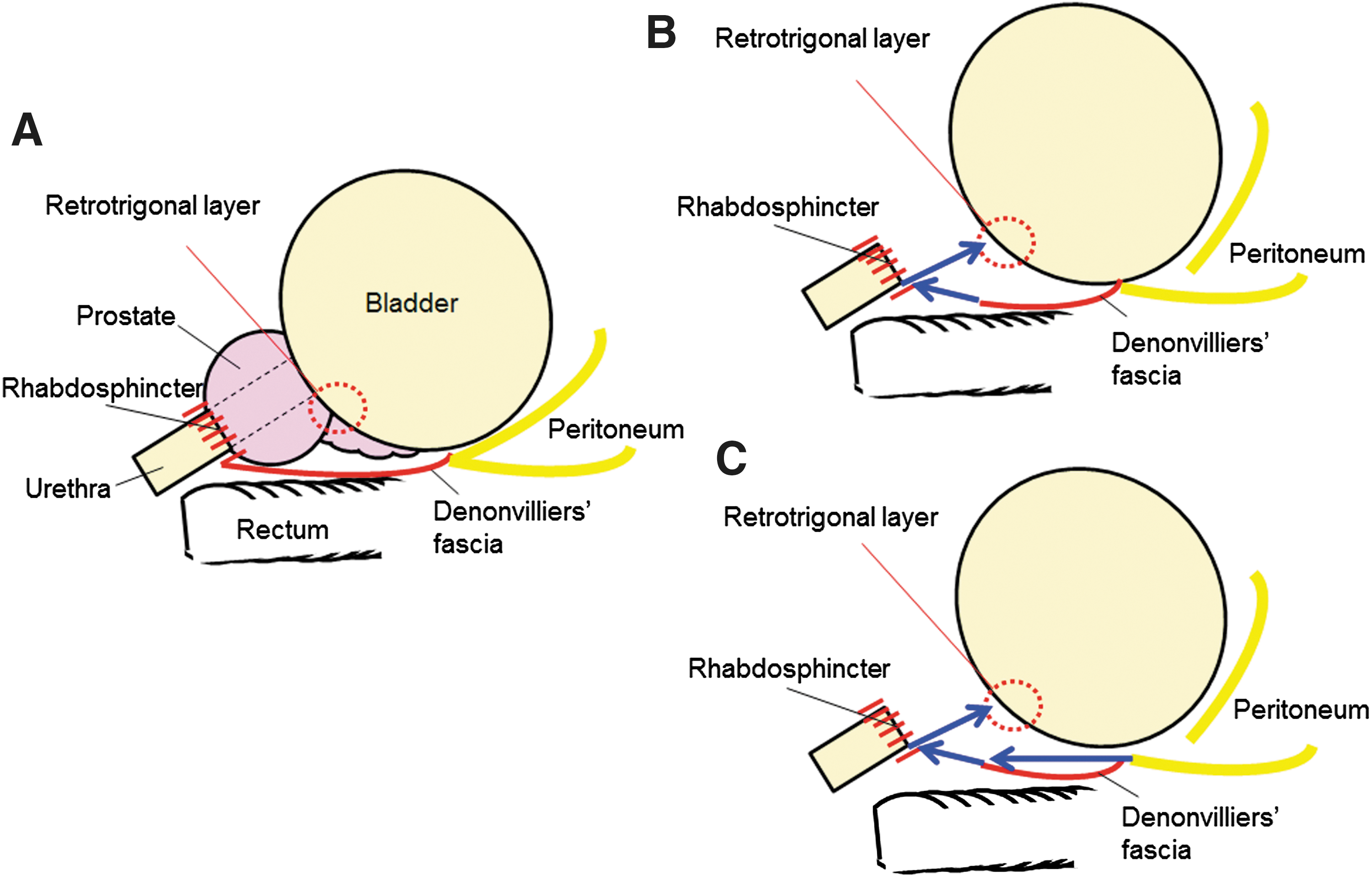
Structure of the posterior musculofascial plate before prostatectomy

Standard two-layer two-step PR
Urinary continence was assessed by the 1-hour pad test, as recommended by the International Continence Society. 22 The test was started by the patient putting on a preweighed pad without voiding. The patient then drank 500 mL of sodium-free liquid in <15 minutes and sat or lay down. Next, the patient walked for 30 minutes, including climbing a flight of stairs (up and down), and performed the following activities: standing up from sitting 10 times, coughing vigorously 10 times, running on the spot for 1 minute, bending to pick up an object from the floor 5 times, and washing the hands in running water for 1 minute. Finally, the amount of urine that had leaked out was determined by weighing the pad. If a moderately full bladder could not be maintained through these procedures (i.e., if the patient had to void), the test was started again. Assessment was performed before RARP as well as 4, 12, 24, and 48 weeks after RARP. The test was performed under medical staff supervision at each clinic visit. Urinary continence was defined as total urine leakage of <5 g in the 1-hour pad test (determined by weighing the pad), because our preliminary study showed that urine leakage in this test was <5 g in all patients before RARP. The primary endpoint was the percentage of patients achieving urinary continence (continence rate) after RARP at different time points, and the continence rates were compared between the two groups.
All patients underwent urethrocystography 6 days postoperatively to measure the craniocaudal distance from the proximal margin of the symphysis pubis to the level of the vesicourethral junction, which indicated postoperative position of vesicourethral junction as reported previously, 23 and to detect leakage at the vesicourethral junction. They also underwent pelvic MRI at 6 months postoperatively to evaluate the anatomy of the posterior aspect of the vesicourethral anastomosis and bladder neck. Since it was difficult to render this anatomical assessment accurately using MRI within 6 month after RARP because of postoperative adhesion and inflammation, we considered that the best time for assessment was 6 months after the operation in this study.
Continuous variables are presented as the median (with interquartile range). We analyzed the data by using Pearson's chi-square test, the Mann–Whitney U-test, or Fisher's exact test as appropriate. SPSS® software ver. 21 (Statistical Package for Social Sciences, Chicago, IL) was used for all analyses, and p < 0.05 was considered significant.
Results
Baseline and postoperative characteristics of the patients in the standard PR group and the three-layer PR group are shown in the Table 1. The two groups were similar in terms of various patient characteristics, including the age, body mass index, prostate-specific antigen, Gleason score, and clinical stage. There were also no significant differences of surgical outcomes between the two groups, including estimated blood loss, prostate weight, and duration of catheterization (days). No patient required open conversion in either group, and there were no postoperative complications, including ileus and urinary retention up to 48 weeks after RARP in either group.
Medians (with interquartile ranges).
BMI = body mass index; PR = posterior reconstruction; PSA = prostate-specific antigen.
In this study, all patients underwent a 1-hour pad test during assessment. Before RARP, the amount of leakage during the pad test was <5 g in all patients of both groups, so the preoperative urinary continence rate was 100% in both groups. In the standard PR group, the urinary continence rates at 4, 12, 24, and 48 weeks after RARP were 26%, 71%, 78%, and 91%, respectively, while the rates in the three-layer PR group were 57%, 74%, 86%, and 89%, respectively (Fig. 4). At 4 weeks after RARP, the urinary continence rate was significantly higher in the three-layer PR group than in the standard PR group (p = 0.036), although there was no significant difference between the groups at 12, 24, and 48 weeks after RARP, indicating that our three-layer two-step PR technique using peritoneum improved early restoration of urinary continence compared with the standard two-layer two-step PR technique.
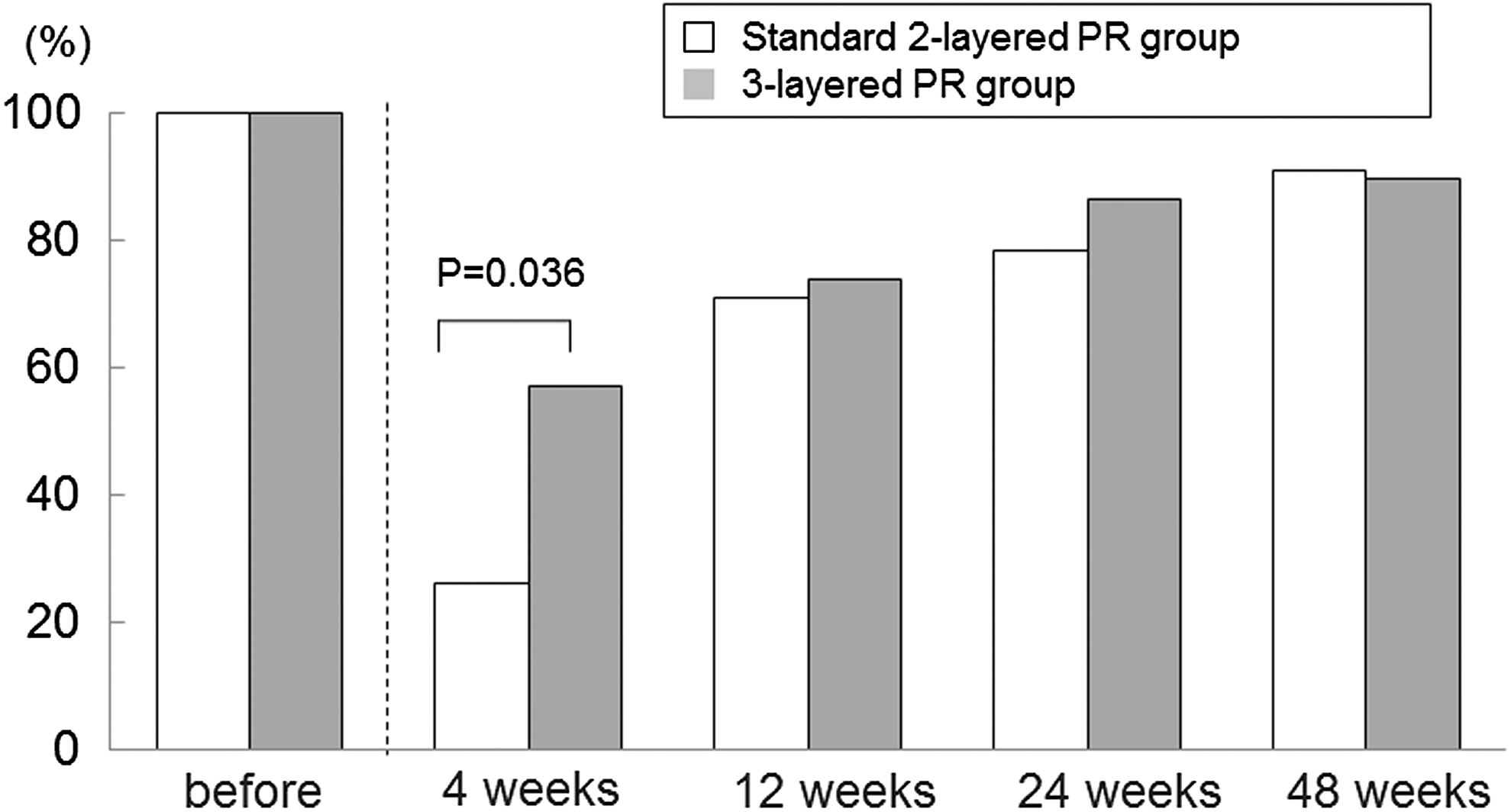
Continence rate at each time of evaluation after standard two-layer two-step PR and three-layer two-step PR.
At 6 days after RARP, urethrocystography demonstrated that the craniocaudal distance (interquartile range) from the proximal margin of the symphysis pubis to the level of the vesicourethral junction was significantly shorter in the three-layer PR group than in the standard PR group (15.5 [12.8–18.2]) mm vs (19.6 [16.1, 23.2] mm, p < 0.01) (Fig. 5), suggesting that there was less tension on the vesicourethral anastomosis with three-layer two-step PR. Urethrocystography also demonstrated that no patient had leakage at the vesicourethral anastomosis in either group. Pelvic MRI confirmed that the three-layer two-step PR technique provided firmer reinforcement of the supporting structures for the posterior aspect of the vesicourethral anastomosis and bladder neck than the standard PR technique (Fig. 6).
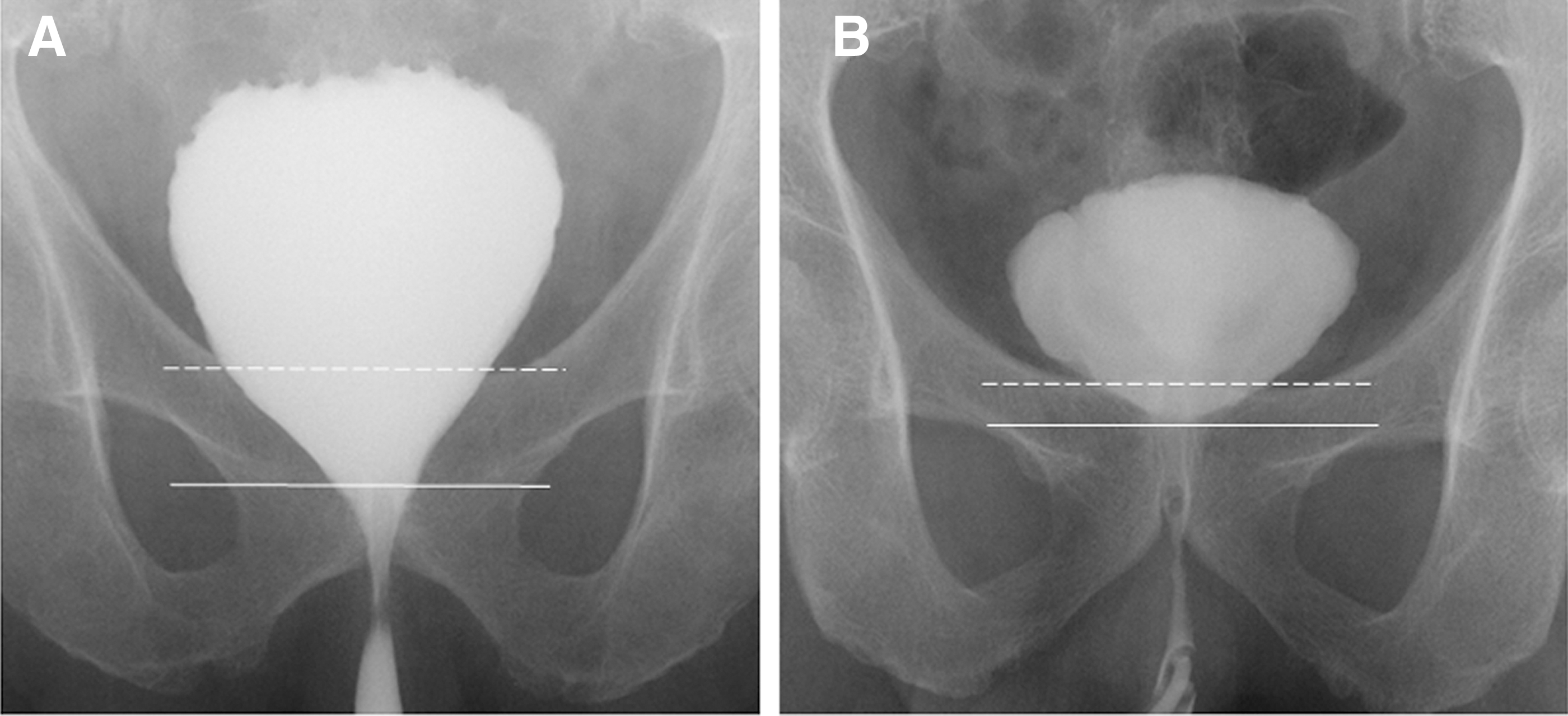
Representative urethrocystogram at 6 days after RARP.
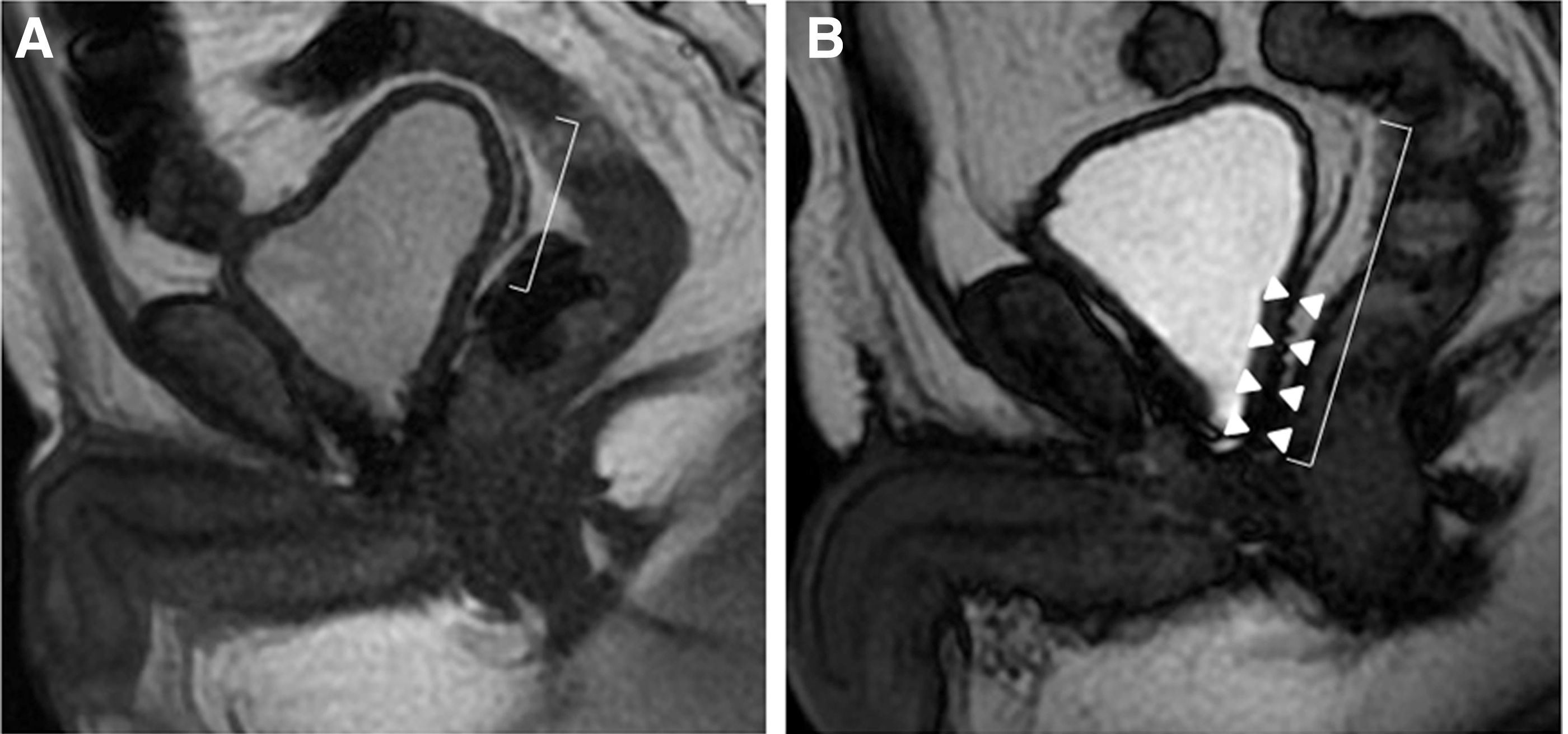
Representative pelvic MRI (T2) findings at 6 months after RARP.
Discussion
We developed a three-layer two-step PR technique using peritoneum, and we examined its usefulness for promoting early recovery of urinary continence after RARP in comparison with the standard PR technique.
PR is one of the most common procedures used to improve the recovery of continence after prostatectomy. In 2001, Rocco and colleagues first reported the use of this technique with retropubic radical prostatectomy. 24 PR achieves an anatomical state closer to the preoperative one with reconstruction of an effective urethral compression system to prevent postoperative urinary incontinence. 11 –18,20 PR also reduces tension on the vesicourethral anastomosis and lessens the risk of leakage. 11 –18 Several modifications of PR have been reported, 11 –17 which can be divided into one-layer one-step PR or two-layer two-step PR.
Previously, two techniques for one-layer one-step PR have been reported. 11 –14 One of these involves placing sutures between the transected musculofascial plate (rhabdosphincter) posterior to the urethra and the cut edge of Denonvillier's fascia located halfway between the bladder and the urethra, while the other technique involves fixation between the transected musculofascial plate (rhabdosphincter) and the posterior wall of the bladder. On the contrary, the original technique reported by Rocco and colleagues was two-layer two-step PR, 1,19,24 in which reconstruction is performed in two layers. The first layer is created by suturing the transected musculofascial plate (rhabdosphincter) posterior to the urethra with the cut edge of Denonvillier's fascia, while the second layer is produced by suturing the rhabdosphincter just below the urethra to the posterior wall of the bladder (the posterior counterpart of the detrusor apron). Some prospective and retrospective studies on the clinical outcome of one-layer one-step PR and two-layer two-step PR after RARP have been performed recently, but the role of PR in postoperative recovery of continence remains controversial. 11 –17 Two retrospective studies of one-layer one-step PR (with approximation of the rhabdosphincter posterior to the urethra to the cut edge of Denonvillier's fascia) showed a beneficial effect on early postoperative return of urinary continence, 11,12 but two prospective studies demonstrated no significant advantage of this technique. 13,14 Jeong and colleagues recently reported the results of a randomized controlled trial (RCT), which showed that a new one-layer one-step PR technique with fixation of the rhabdosphincter to the posterior wall of the bladder was of marginal benefit for early recovery of social continence. 15 Gondo and colleagues reported that two-layer two-step PR was significantly associated with early recovery of urinary continence at 1 month after catheter removal according to univariate analysis. 16 However, Sutherland and colleagues found no advantage of two-layer two-step PR in their RCT. 17
The posterior musculofascial plate plays a significant role as a dynamic support structure for the prostatomembranous urethra. 25,26 This supporting tissue, which increases structural stability, extends from the peritoneum of retrovesical pouch to the perineal membrane and central tendon of the perineum. 19,26 Prostatectomy causes anatomical and functional destruction of this support structure, which may result in postoperative incontinence. 20 We considered that multilayer reconstruction of this support system by modified PR could potentially restore anatomic and functional defects more effectively and provide stronger posterior support for the urethral sphincter complex. Hence, we developed a new three-layer two-step PR technique using peritoneum to improve the recovery of urinary continence after RARP, and compared the outcome with standard two-layer two-step PR at our hospital. The present study demonstrated that the urinary continence rate was significantly higher 4 weeks after RARP in the three-layer PR group than in the standard PR group, suggesting that our three-layer two-step PR technique using peritoneum might be more effective than standard PR for promoting early recovery of continence. Pelvic MRI showed that three-layer two-step PR achieved firmer anatomical reinforcement of posterior supporting structures for the vesicourethral anastomosis and bladder neck. This confirmed that peritoneum provides a stronger base with more structural stability, allowing three-layer two-step PR to improve early recovery of urinary continence compared with standard PR. In addition, the craniocaudal distance from the proximal margin of the symphysis pubis to the level of the vesicourethral junction was significantly shorter in the three-layer PR group than in the standard PR group, suggesting that the peritoneum pulls the rhabdosphincter and urethra upward in the cranial direction and that three-layer PR thus reduces tension on the vesicourethral anastomosis.
In this study, there was no significant difference between the groups at 12, 24, and 48 weeks after RARP. The cumulative analysis of comparative studies published in 2012 showed that standard PR improves early return of continence within the first 30 days after radical prostatectomy, while continence rates 90 days after surgery are not affected by use of the reconstruction technique. 27 The recent overall analysis of comparative studies have shown that PR improved early continence recovery at 3–7, 30, and 90 days after catheter removal, while the continence rate at 180 days was statistically but not clinically affected. 18 Since not only does postoperative continence rate usually improve over time regardless of surgical technique because of recovery from pelvic nerve and muscle damage but also standard two-layer PR can be also expected to improve urinary continence, significant difference may be not found at 12, 24, and 48 weeks after RARP between two groups in this study.
There were some limitations of this study. First, the number of patients is small. Second, our investigation is a single surgeon series at a single center and has a potential for bias. Third, we did not calculate the power and sample size needed to demonstrate a significant difference between the two procedures, although this was a prospective study with patients randomized to two groups and blinded to their group allocation. Therefore, we performed a concurrent cohort study rather than an RCT. Larger multicenter RCTs will be required to confirm our findings. Fourth, this technique is available only when RARP is performed by the transperitoneal posterior approach. Fifth, we did not perform preoperative urethrocystography to compare the position of vesicourethral junction before and after each individual technique to measure the craniocaudal distance from the symphysis pubis to the level of the vesicourethral junction and show if there is a difference between the two techniques. Further study will be needed to confirm our encouraging findings.
Conclusion
This prospective comparative study might suggest that three-layer two-step PR using peritoneum during RARP is a simple and feasible method seeming to improve early recovery of postoperative continence compared with standard two-step PR, although larger multicenter RCTs will be needed.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.