
Abstract
Objective:
The increasing number of flexible ureterorenoscopy (fURS) procedures, the fragility of devices, and their growing maintenance and repair costs represent a substantial burden for urologic departments. Disposable single-use fURS devices offer many advantages over reusable fURS. Among them, the LithoVue™ model shows the best clinical utility. In our study, we assessed the economic aspects of reusable fURS application compared with the potential costs and benefits of single-use fURS (LithoVue™). Indications for single-use fURS were proposed based on potential risk factors of reusable fURS damage.
Materials and Methods:
This single-center retrospective analysis compared the actual cost of reusable fURS procedures with the potential costs of LithoVue™ based on the price offered by the manufacturer. Consecutive case analysis of damaged fURS was performed to determine potential risk factors associated with fURS damage.
Results:
The study group consisted of 423 reusable fURS procedures conducted between January 2013 and December 2016. During this period, 102 (24.11%) diagnostic fURS and 321 (75.89%) fURS for kidney stone therapy were performed. In 32 of 423 (7.57%) fURS cases, devices were postoperatively deemed defective, 9 of which were used for diagnostic procedures (9/102; 8.82%), 7 for stone removal (7/148; 4.73%), and 16 for stone removal and laser (Ho:YAG) application (16/173; 9.25%). The average cost per reusable fURS procedure was found to be €503.26.
Conclusions:
Disposable fURS is a more expensive option for high-volume centers. Based on our case analysis, laser disintegration treatment of multiple, large stones in the lower kidney pole of recurrent stone formers, as well as a steep infundibulopelvic angle (IPA ≤50°), seems to be the main risk factor for fURS damage. For these cases, disposable fURS may be a cost-effective alternative; however, a prospective comparison of economic outcomes between disposable and reusable fURS, together with confirmation of the proposed damage risk factors, is needed.
Introduction
M
Despite improvements over the years in regard to miniaturization, passive and active flexion, and digital imaging, fURS instruments are still fragile and prone to damage. The increasing number of fURS procedures, together with the fragility of the devices and growing costs of maintenance and repair, represents a substantial financial and logistic burden for urologic departments worldwide. 6 –8
Optimization of the cost-effectiveness of these devices can be achieved through constant improvements in surgical technique to increase the durability of already established reusable instruments. 9,10 Some manufacturers have tackled this problem from a different angle by introducing alternative devices. 11 –13
Already present on the market, disposable single-use fURS devices offer many advantages compared with classical reusable digital or fiber-optic fURS. The LithoVue™ model, manufactured by Boston Scientific, has the highest evidence of clinical utility and is comparable to already validated reusable fURS devices. 14 –16
To our knowledge, only one cost analysis has been conducted to date, which compared the real costs of reusable fURS with the anticipated costs of disposable fURS (LithoVue™). 17 Martin et al. conducted a prospective summary of the annual costs of 160 reusable fURS procedures, as well as the repair costs, with a limited description of 11 fURS cases with proven device damage during the same period. Based on this study, reusable fURS was determined to be a far more cost-effective option for high-volume centers in the United States compared with LithoVue™. Further cost analyses, together with the identification of risk factors for fURS damage, are urgently needed.
The aim of our study was to retrospectively assess the economic aspects of application of reusable fURS in a single-center clinical setting, to compare the actual costs with the potential costs of LithoVue™ based on the price offered by the manufacturer, as well as to perform case analysis of damaged fURS to identify potential risk factors for fURS damage.
Materials and Methods
We retrospectively analyzed all fURS cases performed using only reusable fURS at our center between January 2013 and December 2016. Between 2013 and 2015, all fURS surgeries were performed with seven reusable Karl Storz Flex-X2 devices. The real costs consisted of the purchase of three new devices (Olympus URF-V), in service from 2016, the repair costs, as well as the reprocessing cost based on the internal labor cost of designated hospital workers and the fixed sterilization fee of €123 per case (external contract with Vanguard AG). The aforementioned labor cost was estimated to be €20 per case. Postoperatively, the devices were cleaned, tested for leakproofness, disinfected with 30 mL of 1% Gigasept PAA (Schülke & Mayr GmbH), dried, and prepared for transport for external sterilization. This process took around 60 minutes and was conducted by a designated hospital worker.
There was an additional cost of repair of defective fURS by an external outsourced company (Drägerwerk AG & Co. KGaA). The fURS devices that were deemed defective during routine postoperative processing were exchanged for new devices by the manufacturer. The cost of seven Karl Storz Flex-X2 devices that had been purchased before 2013 was not included in our analysis. The real costs and the average cost per procedure were compared with the anticipated cost of the same number of LithoVue™ procedures.
In addition, we conducted a detailed case analysis of damaged fURS to identify factors that could be considered candidates as risk factors for fURS damage. The infundibulopelvic angle (IPA) was measured in accordance with the El-Bahnasy definition. 18 The angle was measured between the ureteropelvic axis and central axis of the lower pole infundibulum based on retrograde pyelography images (Figs. 1 and 2).
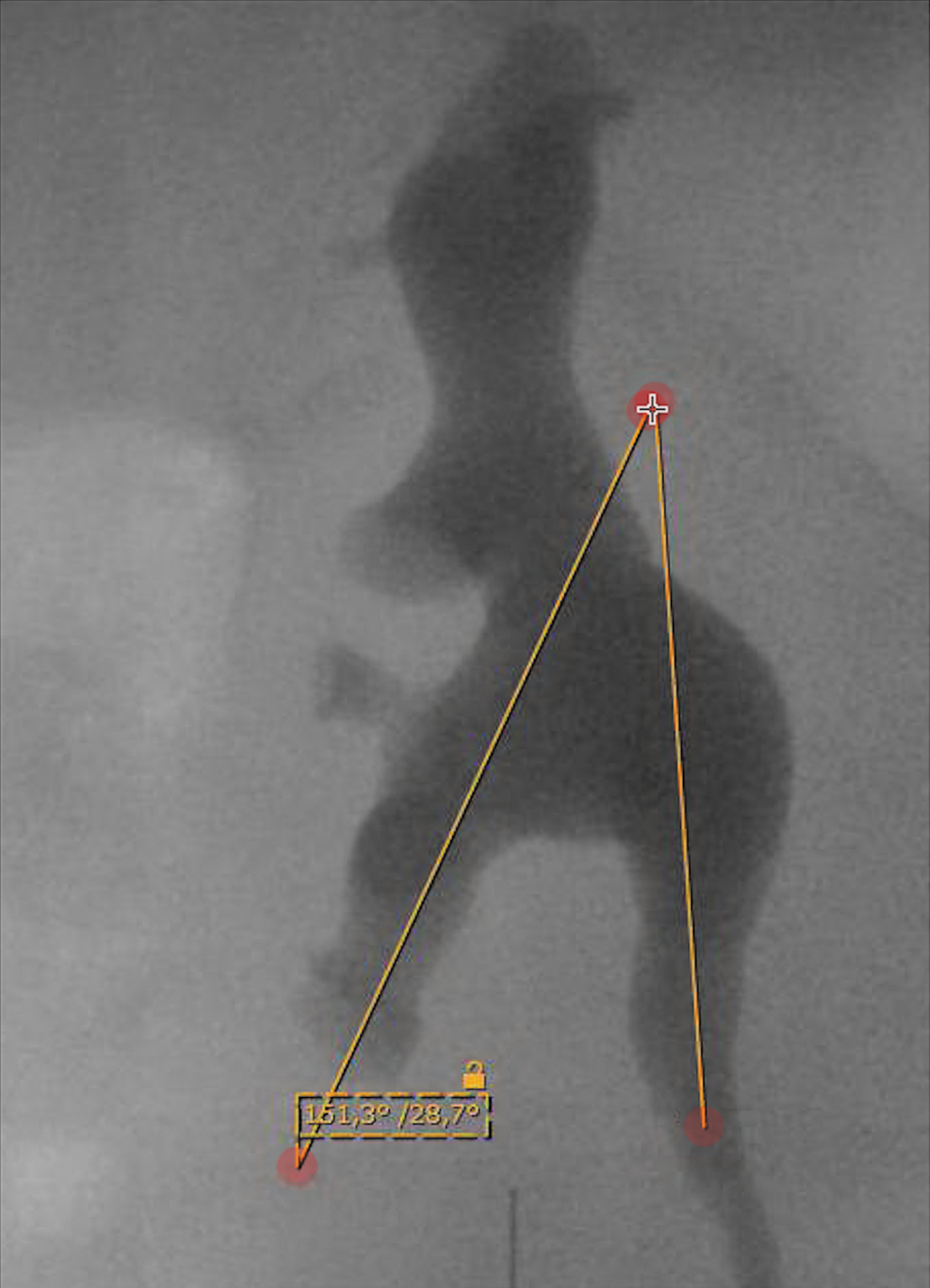
Retrograde pyelography: IPA ≤50°. IPA = infundibulopelvic angle.
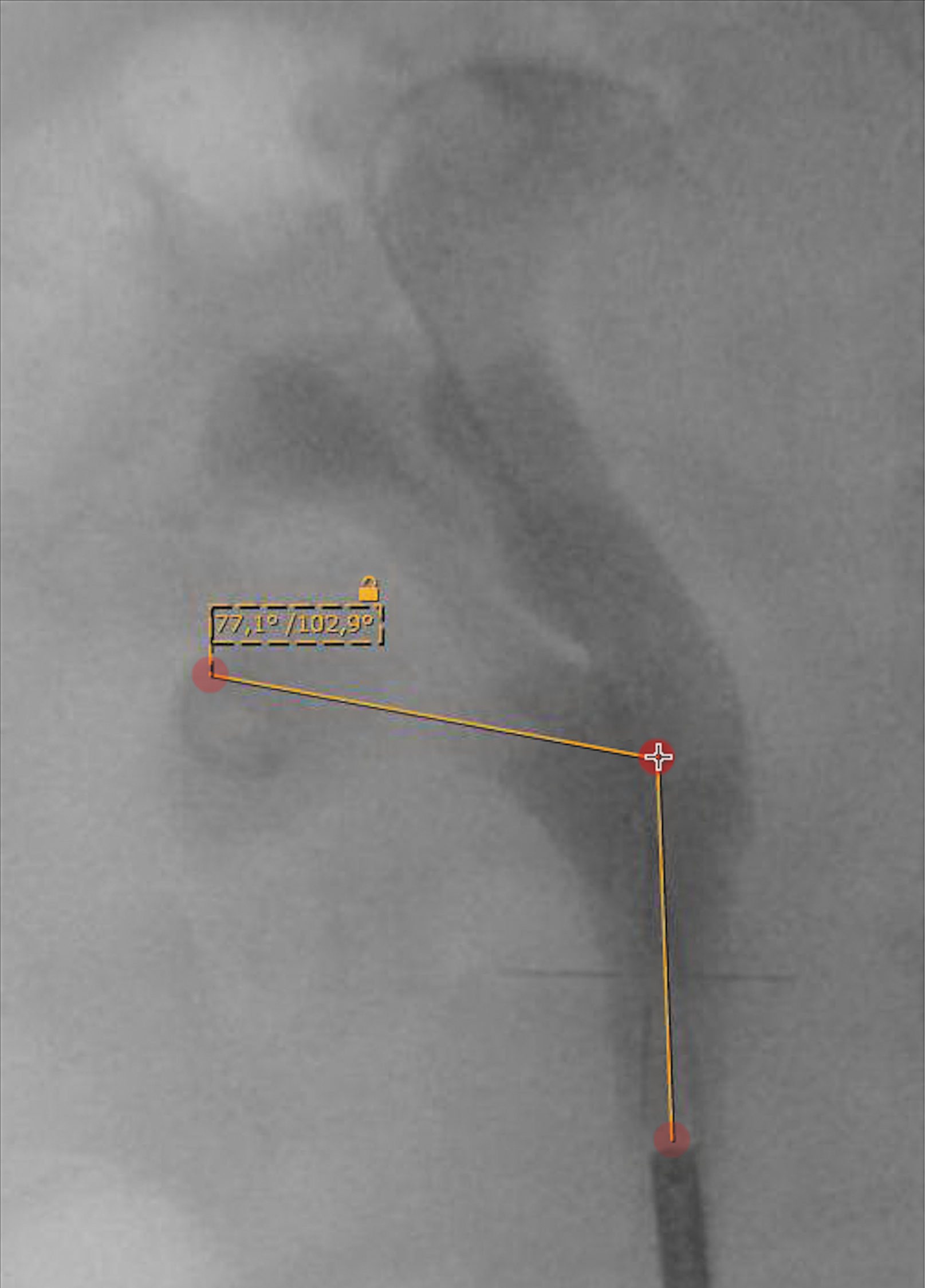
Retrograde pyelography: IPA >50°.
Results
During the given period (January 2013–December 2016), 423 (100%) fURS procedures were performed, 102 (24.11%) of which were diagnostic procedures and 321 (75.89%) for kidney stone therapy. The latter subgroup consisted of 148 (34.99%) fURS for stone removal and 173 (40.9%) fURS for stone removal combined with laser (Ho:YAG) application.
In 32 out of 423 (7.57%) fURS cases, the devices were postoperatively deemed defective and required repair. Of these, 9 had been used for diagnostic fURS (9/102; 8.82%), 7 for fURS with stone removal (7/148; 4.73%), and 16 for fURS with stone removal and laser (Ho:YAG) application via fURS (16/173; 9.25%). Thirty-one of 32 (96.86%) cases with proven fURS damage involved exploration of the lower kidney pole. Twenty out of 23 (86.96%) managed stones were located in the lower kidney pole. The stones that were managed with subsequent fURS damage had a mean diameter of 8 mm (standard deviation [SD] ±6.67 mm) and a mean density of 918 HU (SD ±292 HU). The mean operation time for cases with fURS damage was 80 minutes (SD ±32 minutes). More than half of the damaged fURS cases (18/32; 56.25%) demonstrated a steep IPA ≤50°. Stone-free status was achieved in less than half of cases (10/23, 43.48%). Repair reports revealed two main causes of fURS damage: device leakiness (18/32; 56.25%) and tip break-off (7/32; 21.86%). The average number of cases resulting in fURS damage was estimated to be 14.4. Detailed results regarding damaged fURS are presented in Tables 1 and 2.
fURS = flexible ureterorenoscopy; PNL = percutaneous nephrolithotomy; SD = standard deviation; SWL = extracorporeal shockwave lithotripsy.
The total cost of all fURS procedures was estimated to be €212,880.02. The average cost per fURS procedure was €503.26. A detailed summary of the costs is presented in Table 3. The assumed price per LithoVue™ device was €1000.
Discussion
Our study, conducted without subgroup analysis, confirmed general higher cost-effectiveness of reusable fURS for high-volume stone therapy centers.
In many urologic centers that schedule surgeries for stone treatment, the OR capacity is strongly dependent on the availability of the limited number of fURS devices. Unplanned fURS application (e.g., push-back stones scheduled for semirigid URS without an fURS device on standby) also diminishes the capacity of fURS. As observed in clinical practice, prolonged waiting time for surgery may be associated with unnecessary stress and dissatisfaction for some patients, 19 as well as economic losses for the department.
Single-use devices could represent an alternative to limited availability of reusable fURS by shortening waiting lists and providing more options for the surgeon in cases where the indication for fURS occurs intraoperatively.
Despite any possible inaccuracies of our analysis, we have shown that the economic difference between single-use (€1000 per LithoVue™) and reusable (€503.26 per case) fURS is substantial. Therefore, our reusable fURS program is more cost-efficient, despite some of the advantages of LithoVue™ such as better visibility and maneuverability, best possible brand new device availability 20 and a reduced risk of infection transmission. Disposable fURS can be considered a good option for endourologic treatment in developing countries, where the resources necessary to service and maintain reusable devices are limited.
Beginning in 2016, procedures were performed with two types of fURS devices. Only one case performed with an Olympus URF-V resulted in instrument damage at that time. No procedures were performed using the Olympus URF-V between 2013 and 2015. Thus, we were unable to make any conclusions regarding differences in durability between the two available reusable fURS devices.
Most of the fURS defects occurred in complex cases of kidney stone disease characterized by multiple, large, dense stones, especially those located in the lower kidney pole, that required laser disintegration with application of laser fiber through the fURS working channel. In the majority of cases, the patients were recurrent stone-formers, and stone-free status was not achieved during the usually time-consuming procedure. This group of patients could be an interesting target for application of single-use fURS to prevent future damage.
Detailed analysis of the risk factors for fURS damage identified not only fURS applied for kidney stone therapy but also a proportional number of diagnostic procedures (9/102; 8.82%). The working channel was used for biopsy in only two out of nine cases. Hence, there must be another device damage mechanism that is not directly associated with the use of the working channel with tools such as laser fibers, baskets, or biopsy forceps. A steep IPA ≤50° was confirmed in intraoperative retrograde pyelography in over half of the analyzed cases. Our data and experience suggest that extreme flexion of the tip to reach the lower kidney pole, especially when trying to reach a ventral calyx, could play a role in the fURS damage mechanism.
Almost 50% of arising costs (€102,189.02) were due to the repair of 32 damaged devices. If these cases had been recognized preoperatively and conducted with LithoVue™, our department could have saved enough to cover 70 additional LithoVue™ procedures. The improved fURS capacity by this means could have reduced the number of new Olympus URF-V devices that were purchased in 2016 and, consequently, resulted in further savings.
The pre- and intraoperative risk factors of fURS damage proposed in this article should be confirmed in future comparative studies. Thus, cases in which application of single-use fURS is a cost-effective alternative can be identified.
The retrospective nature of our study can be considered a limitation. Aside from solid data regarding the purchase cost of new devices and the reprocessing and repair costs, additional internal costs that are difficult to quantify should also be taken into consideration. A lack of precise financial data regarding factors such as cleaning materials, storage, and labor, in particular, has led to cost estimation only. For instance, the labor costs to maintain and disinfect already used fURS should not only be considered expenses for wages proportional to time but also as a loss due to the inability of workers to fulfill other clinical tasks during that time. It should be noted that the presented costs are specific to our department, and variability between institutions with regard to processing protocol or personnel is likely.
The cost of the seven Karl Storz Flex-X2 devices that were already in use at the beginning of 2013 was purposefully not included in our analysis. Our study was designed to analyze the expenses associated with a theoretical shift from reusable to single-use devices, not to assess the cost of commencing single-use fURS programs in centers with no fURS equipment. In summary, the low cost of our reusable fURS program is consistent with previously published results showing economic superiority of fURS programs based on reusable devices over the application of single-use instruments only. 17
Conclusions
Shifting from reusable fURS to disposable fURS only may be a more expensive option for high-volume centers. The treatment of multiple, large stones in the lower kidney pole of recurrent stone-formers with laser disintegration, as well as a steep IPA, appears to be the main risk factor for fURS damage. For these cases in particular, disposable fURS may be a more cost-effective alternative. A better understanding of the damage mechanisms is key for a proper indication to use the more expensive single-use device. Prospective comparison between disposable and reusable fURS in regard to economic outcomes, together with confirmation of damage risk factors, is needed.
Footnotes
Acknowledgments
The authors express their gratitude to the coworkers from the University Hospital Schleswig-Holstein in Lübeck, specifically Petra Schwarz and Lothar Lasarzewski, for providing technical data and expertise regarding the processing of fURS devices, and to Andreas Schulz and Sascha Radeke for their help in study group selection.
Author Disclosure Statement
No competing financial interests exist.