
Abstract
Purpose:
To compare the efficiency (stone fragmentation and removal time) and complications of three models of intracorporeal lithotripters in percutaneous nephrolithotomy (PCNL).
Materials and Methods:
Prospective, randomized controlled trial at nine centers in North America from 2009 to 2016. Patients were randomized to one of three lithotripter devices: the Cyberwand, a dual-probe ultrasonic device; the Swiss Lithoclast Select, a combination pneumatic and ultrasonic device; and the StoneBreaker, a portable pneumatic device powered by CO2 cartridges. Since the StoneBreaker lacks an ultrasonic component, it was used with the LUS-II ultrasonic lithotripter to allow fair comparison with combination devices.
Results:
Two hundred seventy patients were enrolled, 69 were excluded after randomization. Two hundred one patients completed the study: 71 in the Cyberwand group, 66 in the Lithoclast Select group, and 64 in the StoneBreaker group. The baseline patient characteristics of the three groups were similar. Mean stone surface area was smaller in the StoneBreaker group at 407.8 mm2 vs 577.5 mm2 (Lithoclast Select) and 627.9 mm2 (Cyberwand). The stone clearance rate was slowest in the StoneBreaker group at 24.0 mm2/min vs 28.9 mm2/min and 32.3 mm2/min in the Lithoclast Select and Cyberwand groups, respectively. After statistically adjusting for the smaller mean stone in the StoneBreaker group, there was no difference in the stone clearance rate among the three groups (p = 0.249). Secondary outcomes, including complications and stone-free rates, were similar between the groups.
Conclusions:
The Cyberwand, Lithoclast Select, and the StoneBreaker lithotripters have similar adjusted stone clearance rates in PCNL for stones >2 cm. The safety and efficacy of these devices are comparable.
Introduction
P
The efficiency of the intracorporeal lithotripter device, the instrument used to remove the majority of the stone burden, is essential to successful stone clearance. For decades, ultrasonic devices have been a mainstay of percutaneous stone removal, utilizing reusable probes, thus minimizing disposable costs. More recently, manufacturers have introduced intracorporeal lithotripters to fragment stones with a variety of energy sources, including pneumatic, ultrasonic, and combination modalities. All of these newer devices utilize disposable probes. Each device features unique properties designed to improve the efficiency of stone clearance, yet few randomized comparison studies have been performed to assess the validity of such claims. 5
Prior studies comparing lithotripter models have yielded variable results. We sought to compare the efficiency (stone fragmentation and removal time) of three current generation lithotripters: the Cyberwand (ACMI/Olympus, Center Valley, PA), a dual-probe ultrasonic device; the Lithoclast Select (Boston Scientific, Marlborough, MA), a combination pneumatic/ultrasonic device; and the StoneBreaker™ (Cook Medical, Bloomington, IN), a portable pneumatic device powered by CO2 cartridges. Since the StoneBreaker lacks an ultrasonic component, it was combined with the LUS-II ultrasonic lithotripter to allow fair comparison with other devices. If a particular device offered superior stone clearance, this would help inform equipment utilization decisions.
Materials and Methods
Study design and participants
We conducted a prospective, multicenter, randomized controlled trial with nine participating sites across North America (Table 1). Each site obtained ethics approval from their respective Institutional Review Board (IRB). Study analysis and data management were conducted at Indiana University (IRB approval No. 1010002258). The study was registered in the
KUB = kidney, ureter, and bladder radiograph; PCNL = percutaneous nephrolithotomy; SWL = extracorporeal shockwave lithotripsy.
Randomization
Subjects were randomized to one of the three devices (Cyberwand, StoneBreaker, or Lithoclast Select) by the research coordinator at the central study site (Indiana University) to minimize allocation error and potential selection bias. Investigating sites contacted the lead site to obtain the randomization result for each patient as they were accrued. Subjects were assigned to study groups using a permuted-block randomization schedule developed by a biostatistician. This method was employed to ensure that the number of subjects assigned to each group was reasonably balanced throughout the study. A randomization log was maintained.
Procedures
Stone surface area (mm2) of the target stone was measured on preoperative CT scan or kidneys, ureter, and bladder radiograph (KUB) by the lead investigator at each study site. The shape of the target stone was outlined allowing standard radiology viewing software to calculate the surface area. This method has been previously shown to give excellent correlation to stone volume. 6 The percutaneous access was established by a urologist, in a prone position, and the target stone was visualized. The time (min) taken to clear the target stone was recorded by designated study personnel using a stopwatch. Clearance time included time spent using the graspers or basket to remove target stone fragments, but not pauses to replace broken probe, unclog the probe, or attend to patient care issues. Only the time taken to treat the target stone (typically the largest stone in the kidney) was measured. If other stones were present, they were subsequently treated, but not included in the study.
The Lithoclast Ultra was used with both ultrasound and pneumatic components. Since the StoneBreaker is unable to remove the stone fragments it creates, it was used in combination with the ultrasonic Olympus LUS-II (Olympus, Melville, NY) lithotripter in this trial. The LUS-II was used only after stone fragmentation by the StoneBreaker was achieved and larger pieces were already removed using graspers. It was used primarily to suction up smaller fragments rather than to fragment the main stone.
Clearance rate was calculated by dividing the surface area of the targeted stone (mm2) by the total clearance time (min). Other study parameters, including number and location of accesses, anesthesia type, blood loss, drainage type, length of stay, transfusion rates, secondary procedures, and complications, were also recorded.
Stone-free rate (a secondary study outcome) was defined as no visible fragments. It was determined either by visualization at secondary nephroscopy or a CT scan within 30 days of the initial procedure. Secondary nephroscopy was employed as a surrogate of stone-free rate since only patients who harbor residual stones on postoperative imaging (typically a CT scan) would be offered this procedure. Stone composition was recorded as the predominant component on stone analysis. Except for the use of a specific lithotripter that they were randomized to, management of the patients in this trial did not otherwise differ from the standard PCNL operation.
Outcomes
The primary study outcome was target stone clearance time in minutes. Stone size variability was larger than expected, so an additional outcome of clearance rate (mm2/min) was added. To calculate the stone clearance rate, the target stone surface area was divided by the stone clearance time. Secondary outcomes were stone-free rate (assessed as described above), secondary procedure rate, complications, and length of stay.
Statistical analysis
Sample size calculations were performed by a biostatistician using a two-sided, two-sample Student's t-test. Since comparisons were made between all three treatment groups, the significance level used to determine the sample size was adjusted. For simplicity, the Bonferroni method was employed (i.e., α = 0.05/3 = 0.017). The primary outcome of interest was the stone clearance time (min). From previous experience in a similar study at our institution, the mean clearance time for stones between 500 and 1000 mm3 using the Olympus LUS-II was found to be 13.7 ± 6.0 minutes. Similar results were expected in our trial. Assuming one of the other study groups has a true stone clearance time that is 25% different than the Olympus LUS-II, then 70 subjects in each group were required to provide 82% power to detect that difference. A total of 210 subjects were needed, 70 into each treatment group. Each arm of the study could enroll as many as 90 subjects for a total of 270 subjects across all sites to obtain 210 completed subjects. Each individual site was allowed to enroll as many as 75 subjects.
Statistical analysis was performed using Minitab 14.2 Statistical Software (Minitab, Inc., State College, PA;
Results
A total of 270 patients were enrolled and randomized at nine sites from October of 2009 to February of 2016. Patient enrolment by site is detailed in Figure 1. After randomization, 69 patients were excluded. The reasons for exclusion postrandomization by treatment group are detailed in Figure 2. The most common exclusion reasons were device not used (17/69 patients, 25%), data not available (16/69, 23%), absence of signed consent form (12/69, 17%), and inability to access the stone (10/69, 14%). The study was completed by 201 patients, 71 in the Cyberwand group, 66 in the Lithoclast Select group, and 64 in the StoneBreaker group. The study outline is detailed in Figure 3.
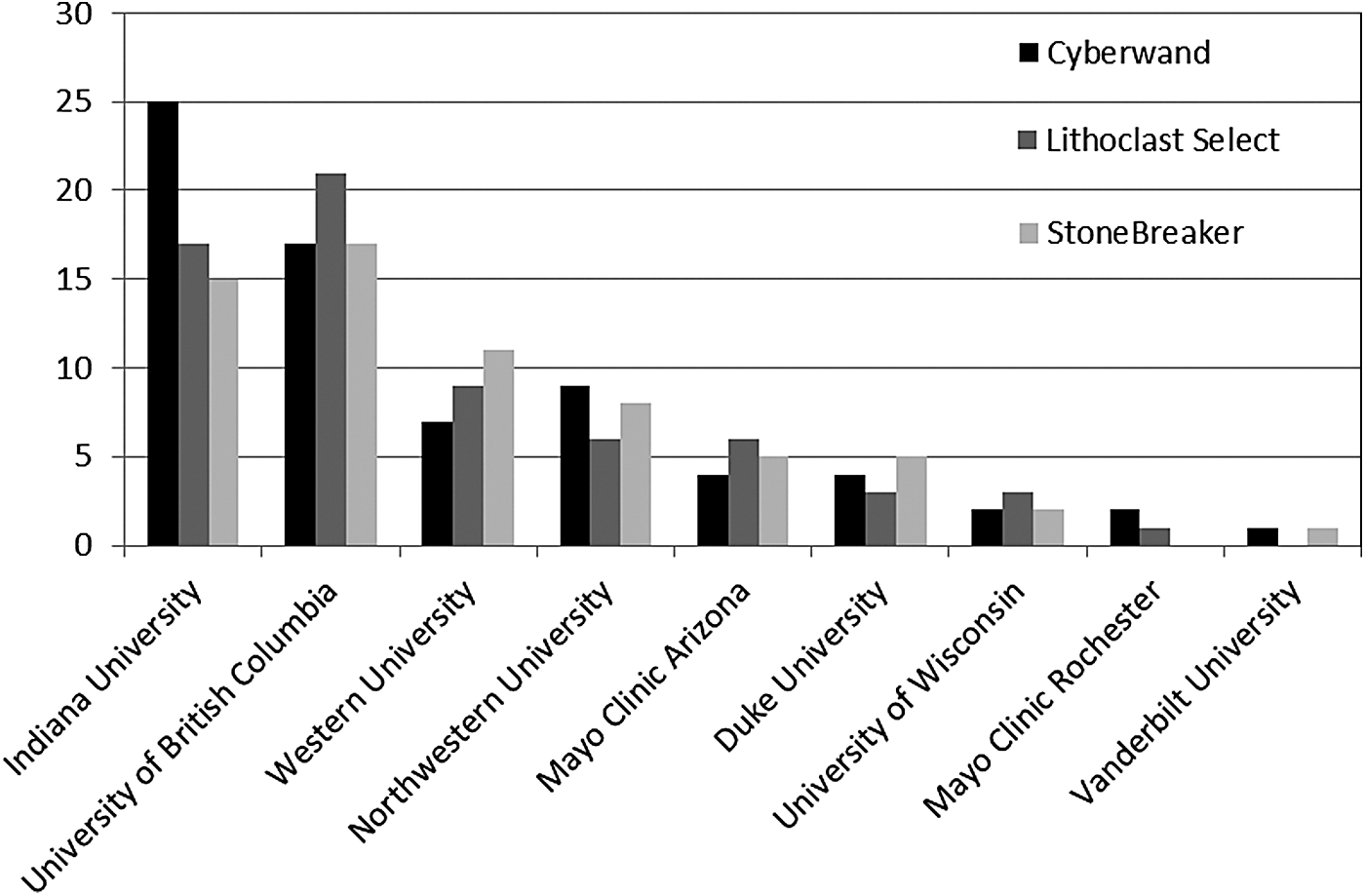
Patient enrollment by study site.

Reasons for patient exclusion (n = 69).
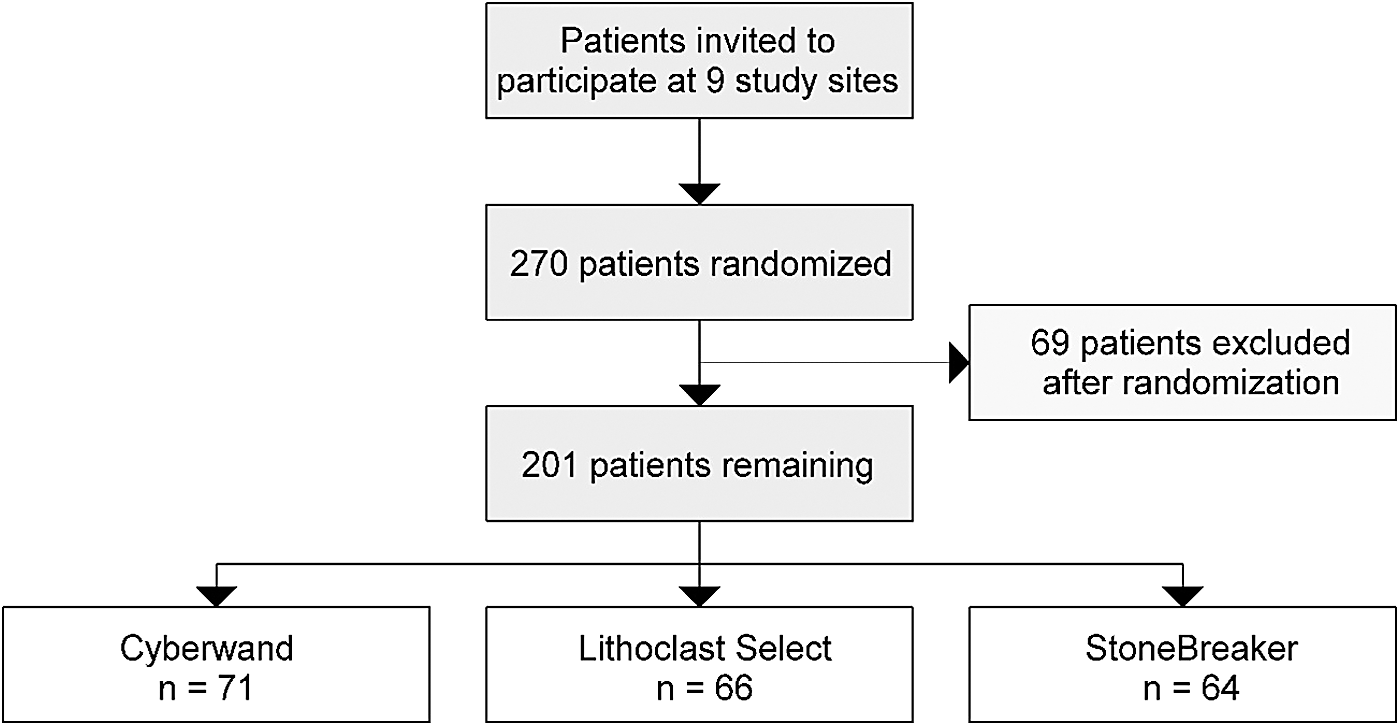
Study outline.
The mean patient age was 57 years (range 20–89 years) and 104/201 (52%) were female. Patients were well matched on baseline characteristics in the three treatment groups, as detailed in Table 3. However, the stone surface area was significantly lower in the StoneBreaker group at 407.8 mm2 compared with 627.9 mm2 in the Cyberwand group and 577.5 mm2 in the Lithoclast Select group, respectively (p = 0.005). The stone clearance time did not differ significantly between the three comparison groups at 28.9 minutes (Cyberwand) vs 26.6 minutes (Lithoclast Select) and 23.4 minutes (StoneBreaker) (p = 0.473). The stone clearance rate (stone surface area divided by the total clearance time) varied from 24.0 mm2/min in the StoneBreaker group to 28.9 mm2/min in the Lithoclast Select group and 32.3 mm2/min in the Cyberwand group, making the Cyberwand appear to be the most effective (p = 0.036). As the stone clearance rate could be affected by stone size, analysis of covariance (ANCOVA) was used to compare the rates across groups while adjusting for stone size. After adjusting for smaller average stone size in the StoneBreaker cohort, there was no significant difference in stone clearance rates between the three devices (p = 0.249, Table 4).
BMI = body mass index.
SD = standard deviation.
Secondary outcomes, including intraoperative or postoperative complications and stone-free rates, were similar between the groups. There were no statistically significant differences in the rates of stent placement, nephrostomy tube placement, use of other devices, reported intraoperative complications, estimated blood loss >400 mL, red blood cell transfusion rates, and the average length of stay. Of the intraoperative complications reported, bleeding (six patients, 3%) and collecting system perforation (seven patients, 3.5%) were the most common. Postoperatively, fever (six patients, 3%), pleural effusion or pneumothorax (five patients, 2.5%), and sepsis (three patients, 1.5%) were the most commonly reported complications. Secondary outcomes are further detailed in Table 5.
EBL = estimated blood loss; RBC = red blood cell.
The stone-free rate following the primary PCNL procedure, defined as no visible stones on postoperative CT scan, averaged 58% with no significant difference between the three groups (p = 0.277). Stone composition was similar in the three groups. The clearance rate of hard stones (defined as brushite, cystine, and uric acid stones) was comparable across the three groups: 25.7 mm2/min in the Cyberwand group, 24.0 mm2/min in the Lithoclast group, and 20.1 mm2/min in the StoneBreaker group (p = 0.671).
Discussion
Lithotripter efficiency is a crucial component of a rapid and successful PCNL procedure. We studied three modern lithotripters to determine stone clearance efficiency in a clinical setting using a randomized controlled trial design to minimize the risk of bias. To allow for fair comparison of devices, StoneBreaker was used in combination with an ultrasonic lithotripter (LUS-II) since the StoneBreaker lacks ultrasonic capability of its own. We included time spent retrieving target stone fragments in the overall treatment time to ensure assessment of true stone clearance and not just the fragmentation time alone. While there appeared to be differences in the clearance rate between groups, after taking into account the variation in stone sizes between groups, we did not find a statistically significant difference between the three devices. The study demonstrated equivalent safety and efficacy of the three devices. There were no significant differences in stone-free status and intraoperative or postoperative complications.
Our findings should be taken into account when considering the purchase of costly lithotripter equipment. Since the device efficiency, as assessed by stone clearance rates, is similar, other factors become more important in choosing a specific lithotripter device. These factors include ergonomics, durability, cost of disposable pieces, and contracts with vendors (Table 6). For example, a strategy to reduce cost might be to use an ultrasonic device such as LUS-II lithotripter initially (reusable parts) for the majority of stones, with the addition of the StoneBreaker for pneumatic fragmentation of particularly hard stones only. In most situations, this would eliminate the need for the routine use of expensive disposables.
Previous studies have compared several lithotripters. Krambeck and colleagues found no difference in the stone clearance rate between the Olympus LUS-II and Cyberwand lithotripters in a randomized trial. 7 In another trial, Chew and colleagues found StoneBreaker to be superior to the Swiss Lithoclast. 8 The Lithoclast Ultra was found to be significantly faster than the LUS-II in a study by Pietrow and colleagues. 9 El-Nahas and colleagues compared an ultrasonic lithotripter (Calcuson/Endomat by Karl Storz) with holmium laser lithotripsy, noting comparable efficacy. 10 Radfar and colleagues found comparable stone clearance with the EMS Swiss Lithoclast and EMS Swiss lithotripter. 11
We incorporated nine high-volume sites across North America to make this study the largest randomized controlled trial to date on this subject and the first comparing Cyberwand, Lithoclast Select, and StoneBreaker directly. The outcomes we report may not be reproducible in a lower volume smaller center without the same operating room resources and staff experience in lithotripsy.
One unexpected finding in our study is the significantly smaller mean stone surface area in the StoneBreaker group. This result is difficult to explain as our study protocol included randomization, thereby controlling for the stone size variable. We carefully reviewed our primary data to identify possible reasons for this finding. Study authors checked individual patient data with regard to stone size. No obvious systemic data entry error existed to explain the smaller stone size in the StoneBreaker group. The patients were randomized from a central location, making bias from one of the treatment sites to use a particular device for smaller stones unlikely. The reasons for patient exclusion after randomization were similar across the three study groups (Fig. 4). Given the smaller average stone size in the StoneBreaker group, statistical adjustments were necessary to compare efficacy of treatment. We used ANCOVA to adjust for stone size and found no significant difference in clearance rate between the three groups (p = 0.249, Table 4). Despite the differences in average surface area, we feel this adjustment would make for a fair comparison between the devices.

Excluded patients by treatment group.
Another limitation of our study is that it is slightly underpowered. A total of 201 patients with 71, 66, and 64 patients in the Cyberwand, Lithoclast Select, and StoneBreaker treatment groups, respectively, completed the study. Our study was powered for 70 patients in each arm. To allow for possible exclusions, 270 patients were randomized. Slightly more than anticipated patients were excluded after randomization resulting in a marginally underpowered study. As detailed in Table 4, clearance time and adjusted clearance rate were not significantly different between the treatment groups. It is possible (but unlikely) that the underpowered sample size is responsible for the finding of no difference between the study groups. A larger target stone size might also have helped differentiate lithotripters, although at the expense of reduced study participant numbers.
Conclusions
This large, multicenter, randomized controlled trial compared three commonly utilized lithotripter devices. Although the StoneBreaker appeared to have a slower clearance rate, this may be due to a smaller average stone size in that group. When adjusted for the difference in stone size between groups, the Cyberwand, Lithoclast Select, and StoneBreaker (in combination with ultrasonic LUS-II) lithotripters have similar stone clearance rates during PCNL for stones greater than 2 cm. The safety and efficacy of these devices are comparable.
Footnotes
Acknowledgments
Cook Medical (StoneBreaker), Boston Scientific Corporation (Lithoclast Select), and ACMI/Olympus (Cyberwand) supplied the lithotripsy test equipment to each study site. No company funding was utilized for study analysis and result reporting.
Author Disclosure Statement
No competing financial interests exist.