
Abstract
Objective:
To assess the “body mass index” (BMI) (weight and length) of 12 flexible ureteroscopes (digital and fiber optic) along with the light cables and camera heads, to make the best use of our instruments.
Materials and Methods:
Twelve different brand-new flexible ureteroscopes from four different manufacturers, along with eight camera heads and three light cables were evaluated. Each ureteroscope, camera head, and light cable was weighted; the total length of each ureteroscope, shaft, handle, flexible end-tip, and cable were all measured.
Results:
According to our measurements (in grams [g]), the lightest ureteroscope was the LithoVue (277.5 g), while the heaviest was the URF-V2 (942.5 g). The lightest fiber optic endoscope was the Viper (309 g), while the heaviest was the Cobra (351.5 g).
Taking into account the entirety of the endoscopes, the lightest ureteroscope was the Lithovue and the heaviest was the Wolf Cobra with the Wolf camera “3 CHIP HD KAMERA KOPF ENDOCAM LOGIC HD” (1474 g). The longest ureteroscope was the URF-P6 (101.6 cm) and the shortest was the LithoVue (95.5 cm); whereas the Viper and Cobra had the longest shaft (69 cm) and URF-V had the shortest shaft (67.2 cm). The URF-V2 had the longest flexible end-tip (7.6 cm), while the LithoVue had the shortest end-tip (5.7 cm) in both directions (up/down), while the URF-V had the shortest upward deflection (3.7 cm).
Conclusions:
Newer more versatile digital endoscopes were lighter than their traditional fiber optic counterparts in their entirety, with disposable endoscope having a clear advantage over other reusable ureteroscopes. Knowing the “BMI” of our flexible ureteroscopes is an important information that every endourologist should always take into consideration.
Introduction
K
As the body mass index (BMI) is an important data to include into the collection of the medical history of the patient, similarly the BMI of flexible ureteroscopes is equally essential information for performing flexible ureteroscopy (fURS) for best outcomes with reduced user fatigue. 4 Minimally invasive surgery (MIS) and endoscopic surgery is attributed to physical discomfort and adequate ergonomic measures are prudent to minimize the risk of upper limb biomechanical overload. 5,6
Apart from a three-dimensional vision, ergonomics of movement and procedural comfort with minimal fatigue was one of the reasons for the rapid uptake and popularity of robotic surgery. 1 Although endourology especially ureteroscopic approach to treatment of kidney stone disease has seen a massive increase in uptake over the last two decades, still very little research is available on the weight of flexible ureteroscopes. It is well known that operating with heavier instruments leads to more discomfort and potentially increase the risk of committing errors for tasks that require precise hand movements over a prolonged duration. 5,6
A prevailing perception of the surgeons is that some instruments are lighter or longer than others; but, to date, studies that systematically evaluate the weight and the length of the flexible ureteroscopes have not been accomplished and the data reported by the manufacturers are sparse.
On the contrary, the diameters of each part of flexible ureteroscopes and the degrees of distal tip deflection (both ventral and dorsal) are very well known. 7
Moreover, it has already been demonstrated how manufacturing companies are not always precise and reliable in reporting features of their medical device. 8
With this in mind, we look at the weight of flexible ureteroscopes on its own and also when connected to the light cable and camera head as supplied by the manufacturers.
Consequently, the aim of this in vitro study was to assess the “BMI” (weight and length) of 12 flexible ureteroscopes (digital and fiber optic), to understand and make the best use of our instruments.
Materials and Methods
Twelve different brand-new flexible ureteroscopes from four manufacturers (Flex-XC, Flex-XC SPIES, Flex-X2 by Karl Storz [Tuttlingen, Germany]; URF-P5, URF-P6, URF-V, URF-V2 by Olympus [Hamburg, Germany]; Viper, Cobra, Cobra Vision, Boa by Richard Wolf [Knittlingen, Germany]; LithoVue by Boston Scientific [Massachusetts, MA]) (Figs. 1 and 2), eight cameras, and three light cables [Karl Storz, Olympus, Richard Wolf] were evaluated.
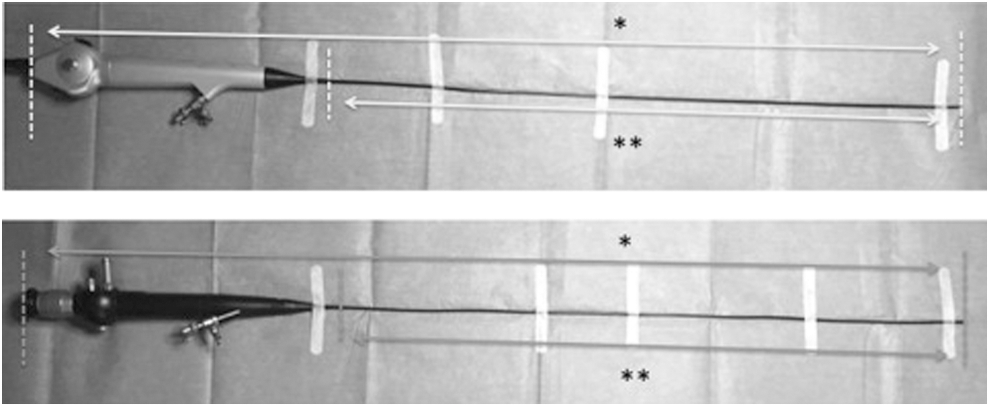
Measurement parameters for total length (*) and shaft length (**) of fiber optic and digital ureteroscope.
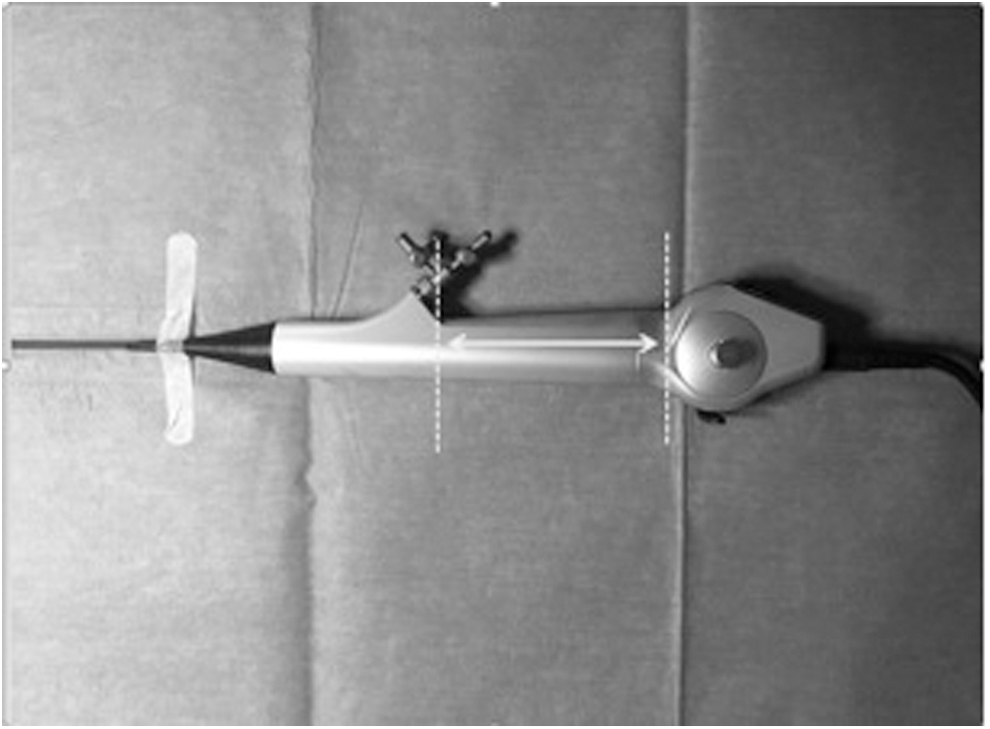
Measurement parameters for handle length.
Each ureteroscope, camera, and light cable were weighted (g) by using a precision digital balance (Serie CM, C.C.I.A.A., Milan, Italy).
The digital flexible ureteroscopes were weighted with their connecting cables.
Moreover, the following parts of the instruments were measured in length (cm) by using a metric digital ruler: the total length of the ureteroscope the shaft the handle the flexible end-tip the cable
Figures 1 to 4 show the measurement parameters including the weight and length of the endoscopes. The measurements were done independently by three different co-authors.
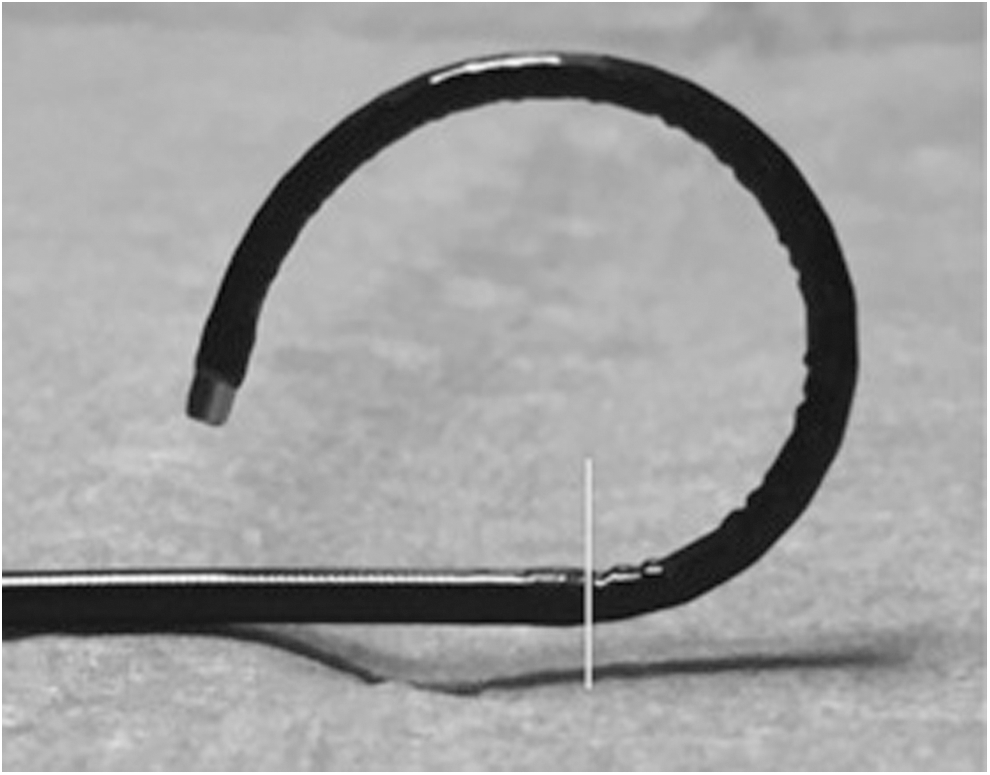
End-tip length for flexible ureteroscope (distal to the white line).
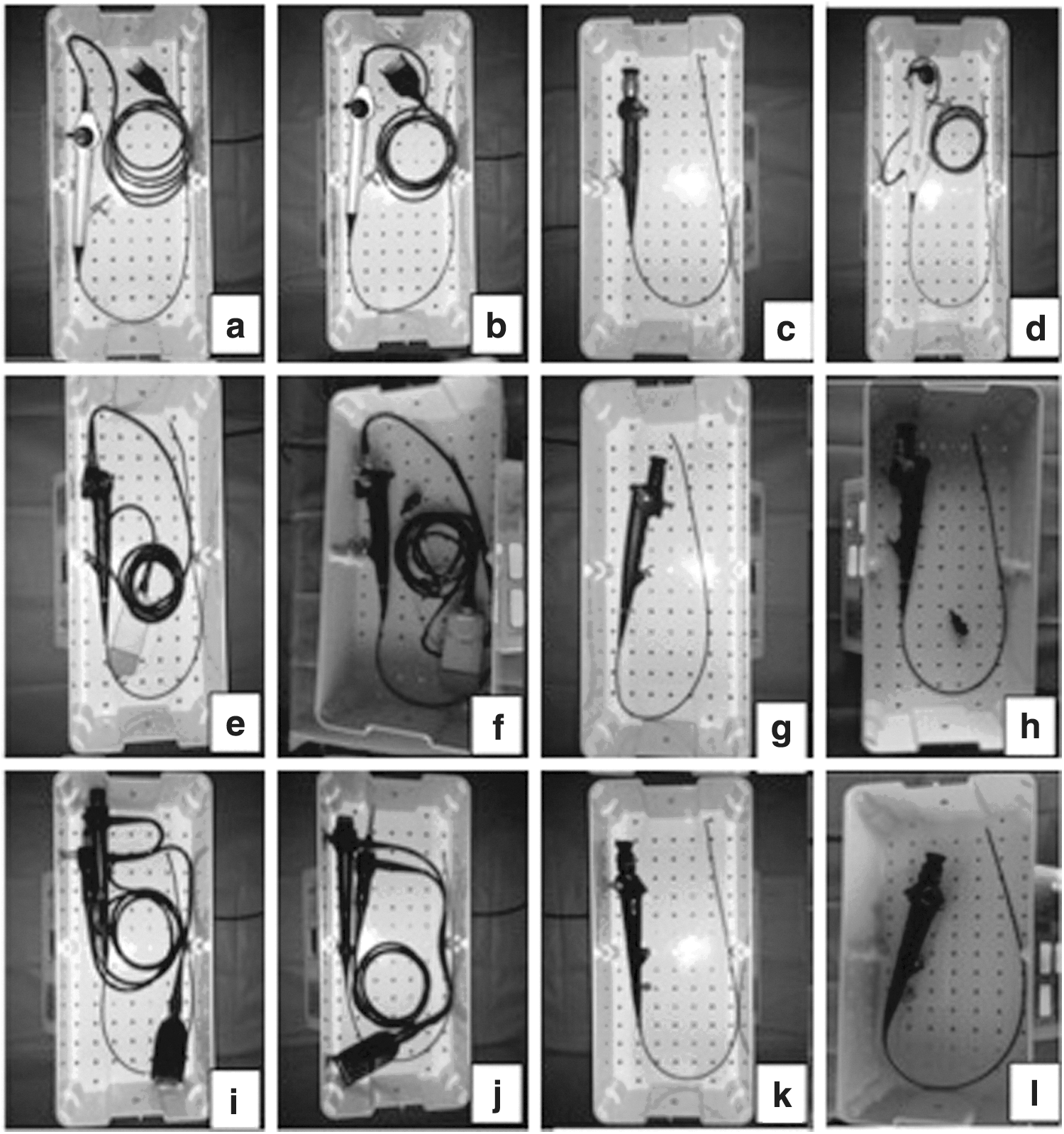
Flexible ureteroscope's weight. Each piece shows each ureteroscope weighted (
Results
According to our overall measurements, the lightest ureteroscope was the LithoVue (277.5 g), while the heaviest was the URF-V2 (942.5 g). The lightest fiber optic endoscope was the Viper (309 g), while the heaviest was the Cobra (351.5 g).
Overall, when we consider the fiber optic endoscopes with cameras and light cables, the lightest combination included the Flex-X2 fiber optic endoscope with the Olympus “OTV-S7 OTV-S7H-1D-L08E” camera (810 g), while the heaviest combination was the Cobra with the Wolf camera “3 CHIP HD KAMERA KOPF ENDOCAM LOGIC HD” (1474 g).
Taking into account the entirety of the endoscopes, the lightest ureteroscope was the Lithovue and the heaviest was the Wolf Cobra with the Wolf camera “3 CHIP HD KAMERA KOPF ENDOCAM LOGIC HD” (1474 g).
The longest ureteroscopes was the URF-P6 (101.6 cm) and the shortest was the LithoVue (95.5 cm); while the Viper and Cobra had the longest shaft (69 cm) the URF-V had the shortest shaft (67.2 cm).
The URF-V2 had the longest flexible end-tip (7.6 cm), while the LithoVue had the shortest end-tip (5.7 cm) in both directions (up/down), while the URF-V had the shortest upward deflection (3.7 cm).
All the measurements determined are reported in Tables 1 to 4. The different lengths of all flexible ureteroscopes are also reported in Figure 5.
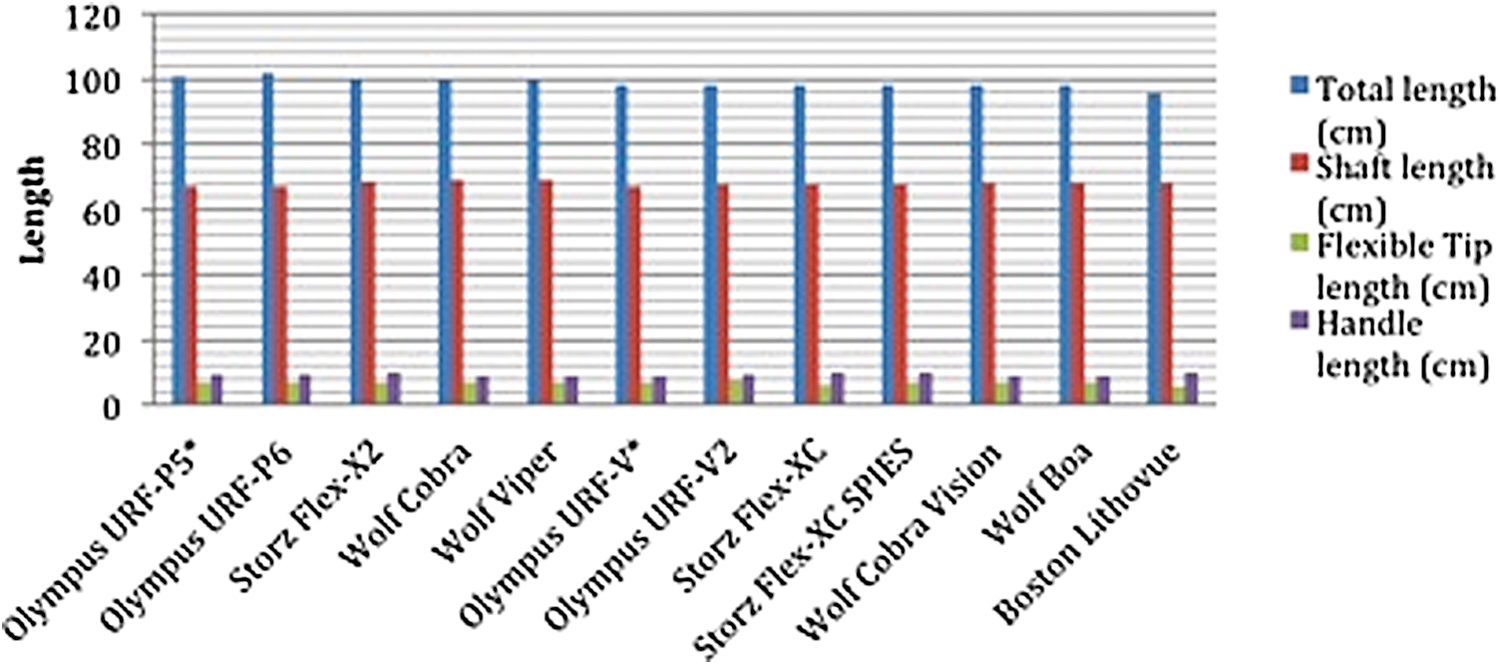
Lengths of flexible ureteroscopes (*down deflection).
Bold means the fibre-optic mean and digital for each parameter analyzed.
Statistically significant difference: p < 0.05.
When considering the weight of the ureteroscopes, this was significantly in favor of the fiber optic ureteroscope (0.006). However, when comparing the length of the endoscopes, the fiber optic endoscopes were statistically longer than digital endoscopes (p < 0.001).
Statistical analysis
Data were collated using Microsoft Excel (version 12.2.4) and analyzed with SPSS (version 21), with the statistical significance calculated using the independent-samples T-test.
Discussion
Despite the widespread application of fURS, no data exist about the weight of the individual endoscopes, camera heads, or light cables with only sparse information about the length of current flexible ureteroscopes.
Meaning of this study
Our study showed a wide variation in the weight of the flexible ureteroscopes, information that is not uniformly provided by the manufacturers or widely available to most endourologists. While the reusable fiber optic endoscopes tended to be the heaviest in their entirety with the camera head and light cable, their counterpart digital endoscopes from the same manufactures were comparatively lighter in weight, with the new digital disposable endoscope being the lightest of them all. A weight difference of 10% to more than 300% was seen between the lighter disposable endoscope and other endoscopes, which is very significant and is potentially of immense clinical relevance especially for prolonged complex procedures.
Moreover, knowing the ureteroscopes' length (both the shaft and the flexible end-tip), could represent an important information together with the maximum end-tip deflection. These data could help the surgeon in their selection of the best instrument according to pyelocaliceal anatomy and in particular to the length of the calyceal infundibulum and infundibulopelvic angle, helping to choose the best fURS for a particular case.
Clinical relevance of the study and areas of future research
It is well known that MIS and endoscopic surgery had a potential risk of upper limb biomechanical overload, 6 and recommendations are already in place to try and reduce this physical overload wherever possible. 9 This consensus document suggests identification of task-related risk factors; evaluation of work overload and methods to analyze and design more ergonomically designed instruments, improved training, and continued health surveillance of healthcare professionals. For ureteroscopy this might simply be ensuring a reduction in the overall procedural weight of the ureteroscope, a decision that will be helped by our article.
Hand and wrist problems are very common among endourologists. In fact, in a recent survey it has been reported that hand/wrist problems are reported in 32% of endourologists who routinely perform fURS compared with controls, in whom that problem was present in only 14% of cases. 10 In our opinion, by considering the weight of the ureteroscopes, these problems could be addressed, in addition to the continuous prone/supination movements associated with it.
Moreover, it has been demonstrated that the surgeon performance and stone-free rate (SFR) during fURS could be related to the surgeons' operating time and consequentially the fatigue associated with it. 4 In this scenario, certainly, a lighter endoscope could be more helpful in decreasing operating time and muscular fatigue than a comparatively heavier one.
Further in vivo studies are needed to better establish the real impact of fURSs weight on muscular fatigue during an endoscopic procedures and consequently on surgeons' performance. These data could be very useful to maximize the efficacy and minimize procedure related injury to the endourologists. Therefore, knowing all the features of our flexible ureteroscope armamentarium, including the “BMI” of the instruments is fundamental information that endourologists should be familiar with. Selectively, it might be helpful before endoscopic approach to choose the most performing endoscope based on stone location and anatomical factors.
As a matter of fact, this is the first study that evaluates the endoscope weight in totality along with the length of the instruments and in particular of their flexible end-tip. It has been demonstrated that in patients with lower pole stones and a length of inferior caliceal infundibulum over 3 cm, the SFR is related to its length. 11,12 In addition to this, it has been shown in an in vitro study that the digital fURS are less successful in accessing a sharp angled calyx and they have less end-tip deflection compared to the fiber optic counterparts. 13 Considering all this information, perhaps further studies on renal anatomy and the success to access to a difficult calyx, could also take into account the length of the end-tip deflection.
As a matter of fact, to date, we do not know whether a longer flexible end-tip could be more helpful or not in complex cases; interestingly in this issue, it is that the Lithovue, even though it is the lightest ureteroscope with its aforementioned advantages for the surgeons' fatigue, has the shortest flexible end-tip (5.7 cm); but further studies are needed to establish whether this feature could affect its use in difficult scenarios, especially in lower calyx.
Moreover, while the fiber optic endoscopes were statistically significant longer in the total length than the digital endoscopes, probably due to the optic part where the camera head is connected to the endoscope, no statistical significant differences were found in the other lengths considered.
It is also interesting to note that the shaft length of all flexible ureteroscopes is between 67 and 69 cm that corresponds approximately to the total length of the kidney, ureter, bladder, and male urethra; and it is probable that the manufacturers had this in mind while establishing the best working length for the flexible ureteroscopes.
Strengths and weakness of our study
The strength of our study is the unbiased evaluation of all available endoscopes as supplied by the manufacturers, including the fiber optic, digital, and disposable endoscopes. With no previous research done in this area, we show objectively the real time weights of the flexible ureteroscopes when it is being used by the endourologist.
Nevertheless, our study outcomes cannot be completely translated in real life weight of the devices because the weight of the plugs and the cables are not all supposed to be borne by the surgeon. They are partly hanging and thus weighting on surgeon's upper limb, while the rest is usually leaned against the patient. Therefore, in this study they were weighted all together with the endoscopes and the cameras, as it was difficult to segregate them.
Although we demonstrate the differences in weight, our study did not look at the impact this has on the ergonomics of movement, image quality, user fatigue, or clinical outcomes. These factors are dependent on other variables during the procedure such as the position of the surgeon, stone location, duration of the procedure, and image quality obtained. Endoscope weight is an important aspect of fURS and for prolonged procedures or high volume centers, this might be an important consideration for purchasing the endoscopes.
With continuing advancement of technology, as endoscope performance improves it is essential to ensure the overall weight of the endoscope decreases, to improve the end-user experience. Ideally, prospective comparative studies using these endoscopes need to be done to ensure that ureteroscopes with most flexibility, portability, and user-friendliness in terms of their performance, weight, and cost will evolve and gain clinical acceptability.
Conclusion
Newer more versatile digital endoscopes were lighter than their traditional fiber optic counterparts in their entirety, with disposable endoscope having a clear advantage over other reusable ureteroscopes.
Knowing the “BMI” of our flexible ureteroscopes is an important information that every endourologist should always take into consideration.
Footnotes
Author Disclosure Statement
S.P., B.S., M.S., A.P., M.R., G.S., F.G.: nothing to disclose. O.T.: consultant for Coloplast, Rocamed, Olympus, Lumenis, Boston Scientific, Biohealth, EMS. G.G.: consultant for Coloplast, Rocamed, Olympus, Lumenis, Boston Scientific, Karl Storz, Cook Medical.