
Abstract
Objective:
To evaluate the impact of the specialty (urologist vs radiologist) of the physician obtaining percutaneous renal access (RA) on perioperative outcomes, complications, and costs of percutaneous nephrolithotomy (PCNL).
Materials and Methods:
We used data from a national hospital discharge database to identify patients undergoing PCNL between 2003 and 2015. Procedure codes related to RA were linked to physician specialty. We examined patient demographics, Charlson comorbidity index, postoperative complications, length of stay (LOS), and direct hospital costs, as well as hospital and surgeon characteristics stratified by specialty of the physician obtaining RA. A multivariable regression model was created adjusting for potential confounders.
Results:
We identified 40,501 patients undergoing PCNL between 2003 and 2015. Urologists obtained access in 17.0% of cases. RA by urologists was associated with a lower 90-day complication rate (5.0% vs 8.3%, p < 0.001) and lower rates of prolonged hospitalization ≥4 days (22.5% vs 42.1%, p < 0.001). On multivariable analysis, RA by urologists was associated with lower rates of any complication (Clavien 1–5) (odds ratios [OR] 0.70, p ≤ 0.001), shorter LOS (OR 0.67, p < 0.001), and lower direct hospital costs (OR 0.65, p < 0.001).
Conclusion:
In the United States, radiologists obtain percutaneous RA in the majority of PCNLs. Access by urologists is associated with lower overall complications, shorter hospitalizations, and lower direct hospital costs. Coding errors and absence of stone complexity information may limit the cogency of our findings and requires further investigation.
Introduction
T
The initial, and often most challenging step in the procedure, is access to the renal caliceal system through a percutaneous approach. Historically, radiologists have obtained RA; however, urologist-acquired access is feasible and appropriate in most cases. Urologists' comfort level with this procedure varies by training, resources, and case volume. Lashley and Fuchs reported the first large series documenting the feasibility and safety of urologist-acquired RA in 1998. 4 They described the use of a ureteral catheter to opacify the collecting system. Complications rates were similar in their series when compared to historical rates with radiologist access.
Few large studies to date compare outcomes and implications of radiologist-acquired vs urologist-acquired RA, 5 –9 and even fewer analyze differences in length of stay (LOS) 6 and cost. These parameters are increasingly important in the present era of cost consciousness. We hypothesize that well-trained urologists with adequate case volume, who obtain their own access, may be able to substantially decrease hospital costs while achieving similar perioperative outcomes (i.e., complication rates and LOS) because a single-stage procedure by a urologist likely reduces redundant use of equipment and staff resources. The aim of this study is to compare the complication rates, LOS, and cost of PCNL between patients who undergo RA acquired by a urologist vs a radiologist.
Subjects and Methods
Population
We used data from the Premier Healthcare Database, a national hospital discharge database, which collects data from over 700 nonfederal hospitals throughout the United States and represents ∼20% of all hospitalizations in the United States. We identified patients undergoing PCNL during the years 2003–2015 using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD9-CM) code 55.03 (Percutaneous nephrostomy without fragmentation) and 55.04 (Percutaneous nephrostomy with fragmentation) with a corresponding ICD9 diagnosis code for nephrolithiasis (592.x). To identify specialty of the physician obtaining RA, we performed a review of the charge description master to identify codes specific to percutaneous access using methodology previously described. 10 Specialty of the physician obtaining RA was then confirmed by linking procedure codes for RA (55.02, 59.8, 55.92, 87.73, and 87.75) within 30 days of index procedure (PCNL), with profession codes of the physician obtaining access. If professional code corresponded to code for nonurologic specialty such as radiology or interventional radiology, then RA by nonurologist was assumed. Current procedural terminology (CPT) codes were used, when available, to identify patients with stones ≤2 cm (50080) and >2 cm (50081), respectively.
Patient characteristics and outcomes
Patient demographics, including age, sex, race/ethnicity, Charlson comorbidity index (CCI), and insurance status were collected. We also examined hospital and surgeon characteristics, including hospital size (≤299 beds vs 300–499 beds vs >499 beds), hospital region and location (urban vs rural), hospital type (teaching vs community), and surgeon volume. Median volume of PCNLs with access obtained by a urologist was five per year. Surgeon volume was analyzed as a continuous variable for the multivariable analysis and a categorical variable in the univariate analysis with high-volume urologists performing at least 10 cases per year. 11 Patients were stratified by whether RA was obtained by a urologist or an interventional radiologist. Direct hospital costs were defined as the total cost of the surgical procedure and inpatient stay, and were inflated to 2015 U.S. Dollars.
Main outcomes included LOS, analyzed as a continuous variable for the multivariable analysis and categorical for the univariate analysis, defined as prolonged if greater or equal to four nights, direct hospital cost for the admission (high cost defined as >75th percentile), and presence of complications. Complications were graded by the Clavien-Dindo classification score. 12 Major complications were defined as complications with a Clavien-Dindo score of 3–5.
Statistical analysis
Demographic characteristics of the patient cohort were described using percentages and medians/interquartile ranges (IQR). Mann–Whitney U tests were used for comparison of continuous variables and Chi-square tests were used for categorical variables. Multivariate logistic regression was performed and odds ratios (OR) were calculated to identify independent risk factors for the primary outcomes, although controlling for covariates. All tests were two-tailed, with p < 0.05 considered significant. Statistical analysis was performed using STATA 14 (StataCorp. 2015, College Station, TX).
Results
We identified 40,501 patients undergoing a PCNL between 2003 and 2015. Baseline characteristics of the cohort stratified by urologist-obtained vs radiologist-obtained access are shown in Table 1. Access by a urologist was performed in 17.0% of patients. The median age was 56 in the urologist access group and 57 in the radiologist access group. 15.7% of patients had a CCI of at least 2. Patients who underwent access by a urologist were more likely to be younger, male, and healthier than patients in the radiologist access group.
IQR = interquartile ranges.
Hospital and surgeon characteristics in patients with access obtained by urologists vs interventional radiologists are shown in Table 2. Notably, patients at hospitals with >499 beds are more likely to have the procedure done by a urologist (18.7%) than patients at small hospitals (15.0% at hospitals with both ≤299 and 300–499 beds) (p < 0.001). RA by a urologist was also more likely to be obtained at teaching hospitals (19.2%) than nonteaching hospitals (14.6%) (p < 0.001). In addition, a higher percentage of RA is acquired by urologists in the northeast (21.6%) compared to the Midwest (15.9%), South (17.0%), and West (11.3%) (p < 0.001), which may reflect regional variations in practice.
Patients with access acquired by interventional radiologists were more likely to have any complication than patients with RA obtained by urologists (8.3% vs 5.0%, respectively, p < 0.001), and more likely to have a prolonged LOS (LOS ≥4 is 42.1% in radiology group vs 22.5% in urologist group, p < 0.0001) (Table 3). The rate of major complications remains low (1.7%) and are more associated with radiologist access (1.8% vs 1.2%) (p < 0.001). The median cost of an admission when RA is achieved by a urologist was $10,173 (IQR $7450–$14,215) compared to the cost of admission when radiologists obtain RA ($11,287; IQR $7736–$17,162).
LOS = length of stay.
On a multivariable analysis, RA by urologists remains an independent predictor of fewer complications (OR 0.70, 95% CI 0.62–0.78, p < 0.001) when controlling for age, gender, race, comorbidities, surgeon volume, hospital size, hospital teaching status, payer status, and location of hospital in an urban setting (Fig. 1). In addition, RA by urologists was an independent predictor of shorter LOS (OR 0.67, 95% CI 0.65–0.69, p < 0.001) and decreased direct hospital cost (OR 0.65, 95% CI 0.61–0.70, p < 0.001).
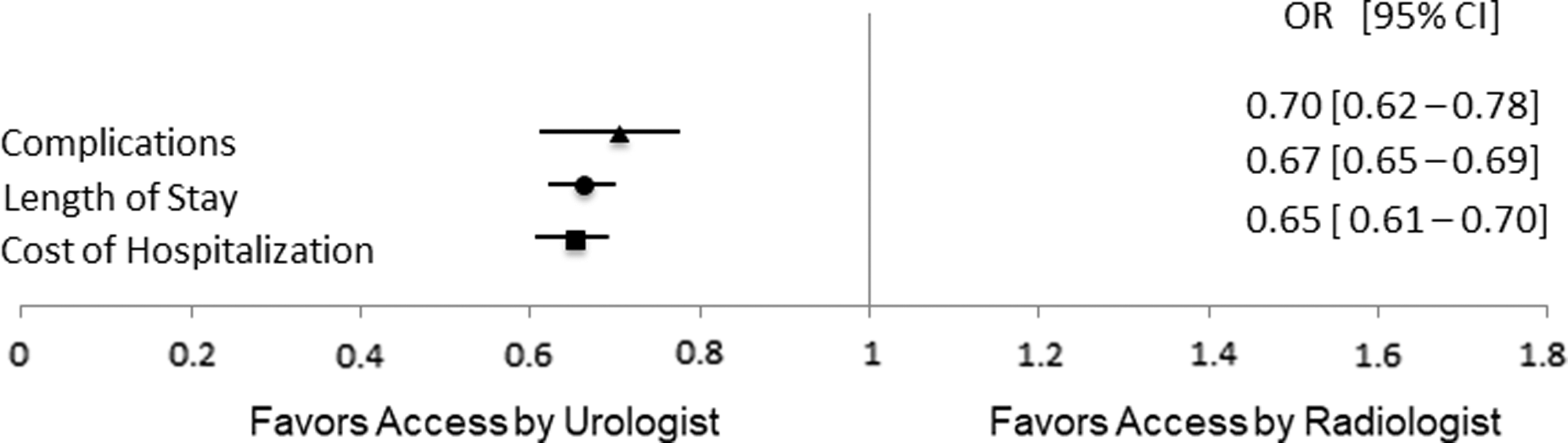
The association between physician specialty and length of stay, direct hospital costs, and complications controlling for age, gender, race, Charlson comorbidity index, insurance, hospital size, hospital type, and surgeon volume.
CPT codes identifying stone size were available in 13% of our cohort (5210 patients). Of these, 57.6% of patients had a stone size ≤2 cm, and 42.4% had a stone size >2 cm. Stone size had no impact on rates of RA by physician specialty with similar proportion of urologists obtaining percutaneous access in both stone size groups (26% and 25%, p = 0.18).
Discussion
We found that urologists obtain their own access in the minority of cases in the United States and urologist-obtained RA is associated with shorter hospitalizations, fewer complications, and lower direct hospital costs, even when controlling for age and comorbidities. Our study is one of the first to examine the implications on healthcare costs of urologist vs interventional radiologist-obtained RA for patients undergoing PCNL. This is also the largest study to date comparing LOS and complications based on which specialty obtains RA.
In the United States, urologists obtain access in less than 20% of PCNL cases. This is in contrast to practices in Europe where urologists obtain their own access more routinely. Aslam and colleagues surveyed the National Health Services hospitals in the United Kingdom and found that 45% had radiologist-obtained tracts, 44% used urologist-obtained tracts, and 11% used both. 5
Reasons for lower rates of urologist-obtained access in United States were assessed in a study by Lee and colleagues. 13 The authors surveyed former University of Minnesota urology residents regarding their management of large renal stones. They noted that urologists who were trained to obtain percutaneous access were more likely to perform PCNLs than those with less experience (92% vs 33%, p < 0.001), but only 33% of trained urologists obtained their own access. 13 Reasons for not obtaining access more frequently among urologists trained in percutaneous access included that the radiologists had better equipment (61%), the radiologists had superior skill (44%), the politics of the hospital favored radiology access (28%), that there is inadequate reimbursement (17%), or that the access required extra time (50%). 13
Although U.S. urologists are not obtaining access as frequently as United Kingdom urologists, there is a trend toward increased urologist-acquired access in the United States. In a survey of all American Urological Association members in the North Central Section in 2002, just 11% of urologists responded that they routinely obtained their own access. 14 Jayram and Matlaga examined case logs of certifying and recertifying urologists between 2004 and 2013. 11 They found that urologist-obtained access increased from 14.5% in 2004 to 20.4% in 2012. In addition, although all urologists increased their usage of PCNLs, initially certifying urologists performed more PCNLs than recertifying urologists (53% vs 29% in the oldest recertifying group). On examination of our data, we also found that there has been a trend toward a higher percentage of urologists acquiring their own access (17.0% in 2003 to 20.5% in 2015, p for trend <0.001).
Previous studies have noted similar complication rates in patients with radiologist-acquired vs urologist-acquired access, concluding that it is safe for urologists to obtain access. 6 –8 In a single-center study with 103 patients, Watterson and colleagues found that access-related complications were lower when urologists obtained access (8.3% vs 27.8% in radiologist group, p = 0.02). 9 Aslam and colleagues also found higher complication rates in patients with radiologist-acquired tracts (6.8% vs 22.6%, p = 0.0029), but there was a selection bias for more complex anatomy in the radiology group. 5 Notably, we found that when urologists obtained access, there was a 3.0% decrease in overall complication rate and a 0.6% decrease in major complication rates. This reinforces prior findings of the safety of urologist-obtained access.
In addition, we demonstrated that urologist-obtained access is associated with a 9.9% cost reduction in direct hospital cost when compared to interventional radiologist-obtained access. Urologist access remained an independent predictor of lower cost when controlling for complications, CCI, age, surgeon volume, race, hospital volume, hospital teaching status, payer status, and location of hospital in an urban setting. There are likely multiple factors driving the higher cost, including higher procedural costs with a two-stage procedure, longer LOS, and the potential for duplicate billing. Tomaszewski and colleagues in their single-institution study comparing access between radiologists and urologists found that 36.8% of tracts made by radiologists were unusable, necessitating new urologist-acquired RA. 8
Similar to cost of procedure, we found that urologist access is associated with a decreased LOS. Chen and colleagues also studied LOS comparing patients with urologist-obtained vs radiologist-obtained access. They noted that the patients with a one-step PCNL had a shorter LOS, but that their postoperative stay was similar, as many patients had the radiologist access obtained the day before the PCNL. 6 We did not assess whether access was obtained on the day of the PCNL vs the day before the PCNL. This may also explain our finding that urologist access patients have a shorter LOS.
In a subgroup analysis of patients with known stone size based on CPT codes, we found that there was no significant difference between the distribution of urologists and radiologists obtaining access for patients with renal stones less than or greater than 2 cm. Furthermore, we saw similar findings with regard to primary outcomes in this group of patients, suggesting that the interspecialty differences that were observed in the study were not related to stone size.
There are several limitations to our study. In particular, the Premier database is an administrative dataset that is not collected for study purposes. There is the potential for coding errors. Readmission and complication rates may not be fully captured as the patient may present to another hospital. The groups did differ significantly in their baseline characteristics, with patients with radiologist-acquired RA being slightly older and having a higher CCI, but this was controlled for in the multivariate analysis. In addition, we were not able to account for joint access; cases with joint access may have been designated as radiologist access due to coding limitations. Details on radiation exposure dose and stone-free rates would be useful as they may vary between the specialists obtaining access and are pertinent to patient outcomes. Stone-free rates are of particular importance as they are a marker of the success of the PCNL. Notably, Tomaszewski and colleagues found that in a cohort with similar stone complexity, the stone-free rate was 6.9% better when urologists obtained access (99% vs 92.1%, p = 0.033). 8 Additional information on location of puncture site and need for multiple punctures would also be useful and may influence the stone clearance rate, complication rate, and LOS.
Conclusion
Urologist-obtained access for PCNL is a safe practice and appears to be associated with decreased cost and LOS without an increase in complication rate. In the United States, radiologists obtain the majority of RA for PCNL, with an increasing trend toward urologists obtaining their own access. Although our study is limited by lack of information regarding stone complexity and stone-free-rates, as well as coding errors associated with use of a large administrative database, our findings suggest that for well-trained urologists, it is safe and cost-effective, to obtain RA.
Footnotes
Author Disclosure Statement
No competing financial interests exist.