
Abstract
Introduction:
With the introduction of laparoscopy and now robotics, more patients are able to reap benefit from minimally invasive techniques during urologic surgery. With these advancing technologies, it is important to evaluate whether the outlay of hospital capital actually improves patient care. To date, there has been little literature regarding the impact of these advances on patient outcomes. In this article, we directly compare perioperative outcomes and hospital costs between the older da Vinci Standard/S/Si platform and the newer Xi robotic platform during nephroureterectomy.
Methods:
A review of our robotic nephroureterectomy database between April 2009 and December 2017 identified 87 patients, 30 in group 1 (Xi) and 57 in group 2 (Standard/S/Si). Preoperative, perioperative, and postoperative parameters as well as hospital costs were evaluated. Independent t-test was performed for continuous variables, while categorical variables were evaluated using chi-square tests or Fisher's exact test.
Results:
There were no significant differences between groups preoperatively. Operative time using the Xi was shorter, 184.4 vs 232.09 minutes (p = 0.0035). Other perioperative variables were similar. There was more lymphovascular invasion in group 2 (p = 0.0108), but there were higher stage tumors in group 1 (p < 0.0001). More patients underwent lymph node dissection in group 1 (p = 0.0186). Complications were similar between groups. Costs for anesthesia were less in group 1, which led to decreased total hospitalization costs (p < 0.001)
Conclusion:
Operative times were found to be less with the daVinci Xi, without any other significant difference in patient outcomes between the groups. Anesthesia and operating room cost were substantial factors in lowering the overall hospital costs. More multi-institutional studies with larger groups of patients are needed to determine if advancing technology really improves outcomes.
Introduction
W
Since first approved in 2000 by the Food and Drug Administration, the da Vinci robot (Intuitive Surgical, Inc., Sunnyvale, CA) has undergone numerous changes and advances. In 2014, the fourth generation platform, daVinci Xi, was introduced with the goals of easier docking, wider range of motion, and multiquadrant surgery. We were one of the first institutions to demonstrate a comprehensive port template for robotic nephroureterectomy utilizing the da Vinci standard, S, and Si platforms. 5 At our institution, we began operating with the da Vinci Xi in December 2014. Since then, we have been performing all nephroureterectomies with this platform as this procedure includes both an upper and lower tract component as well as an extirpative and reconstructive component.
With this advancing technology, it is important to evaluate whether the outlay of precious hospital capital actually improves patient care. To date, there has been little literature regarding the impact of these advances on patient outcomes. In this study, we directly compare perioperative outcomes and hospital costs between the older Standard/S/Si platforms and the newer Xi robotic platform during nephroureterectomy.
Methods
A retrospective review was performed of our prospectively maintained IRB approved database. Eighty-seven robotic nephroureterectomies were performed at the Wake Forest University Baptist Medical center between April 2009 and April 2017 by a single surgeon. Two groups were established based on robotic platform used, the da Vinci Xi platform (group 1) and the older standard/S/Si platform (group 2). All patients were evaluated with a preoperative physical examination, appropriate laboratories, and imaging (computed tomography urogram and/or magnetic resonance urogram). Preoperative, perioperative, and postoperative parameters were evaluated. Hospital costs were obtained directly from resource management administration at Wake Forest Baptist Medical Center. Independent t-test was performed for continuous variables, while categorical variables were evaluated using chi-square tests or Fisher's exact test. All statistics were performed by a biostatistician from the Wake Forest University School of Public health.
Operative Technique 6
Patient positioning
The patient is brought to the operating room and general anesthesia is induced. A Foley catheter is placed. The patient is placed in the full flank position with operative side up. The table is flexed to open up the space between the costal margin and the iliac crest. The patient is secured with all pressure points appropriately padded.
Port placement for the da Vinci S/standard/Si platform (Fig. 1)
Pneumoperitoneum is initially established to 20 mm Hg for port placement only and then decreased to 12–15 mm Hg during the procedure. The initial 12 mm camera port is placed just lateral to the rectus muscle and lateral and cranial to the umbilicus. The first 8 mm working port is placed lateral to the rectus muscle about 2 cm below the costal margin. The second working port is placed about 4–5 cm inferior to the camera port. The third working port is placed about 2 cm medial to the anterior superior iliac spine. A 12 mm Air Seal assistant port (if available) is placed in the midline about 3 cm superior to the umbilicus avoiding collision with camera port. The robot is docked over the back of the patient perpendicular to the table.
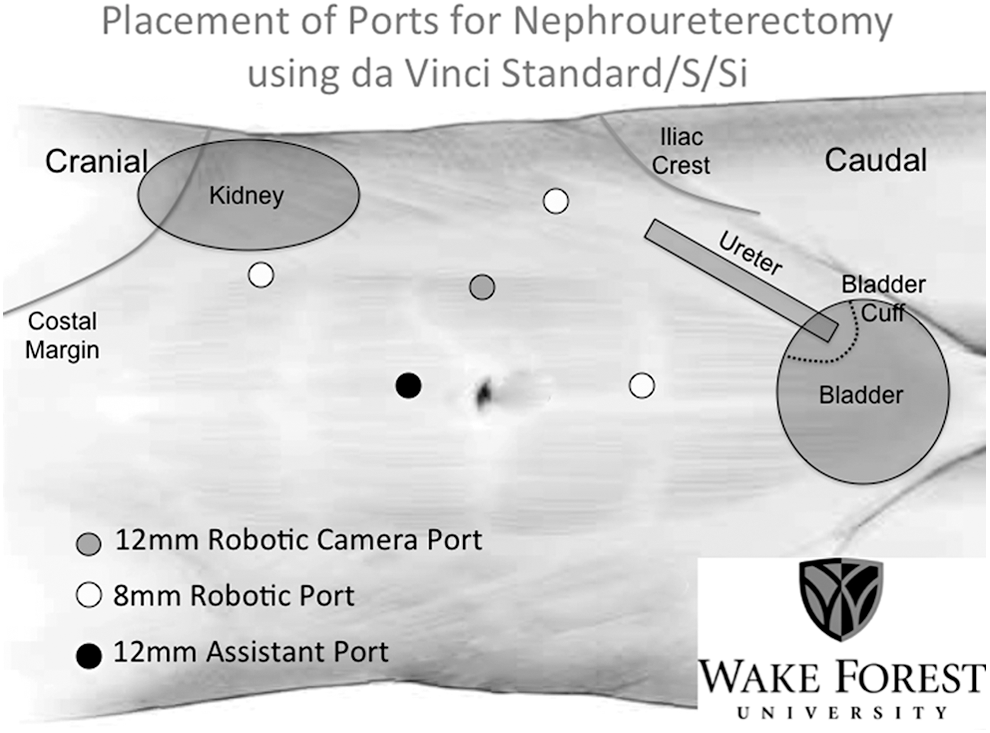
Port placement for da Vinci Standard/S/Si.
Port placement for the da Vinci Xi platform (Fig. 2)
Pneumoperitoneum is initially established to 20 mm Hg for port placement only and then decreased to 12–15 mm Hg during the procedure. All ports are placed in a straight line just lateral to the rectus muscle. The initial 8 mm port is placed just lateral and superior to the umbilicus. The second port is placed in line about 2 cm inferior to the costal margin. The third robotic port is placed about 5–6 cm inferior to the camera port. The final port is placed about 5–6 cm inferior to the third port or somewhere in the midline. A 12 mm Airseal port is placed in the midline about 3 cm superior to the umbilicus avoiding collision with camera port. The robot is docked over the back of the patient perpendicular to the bed.
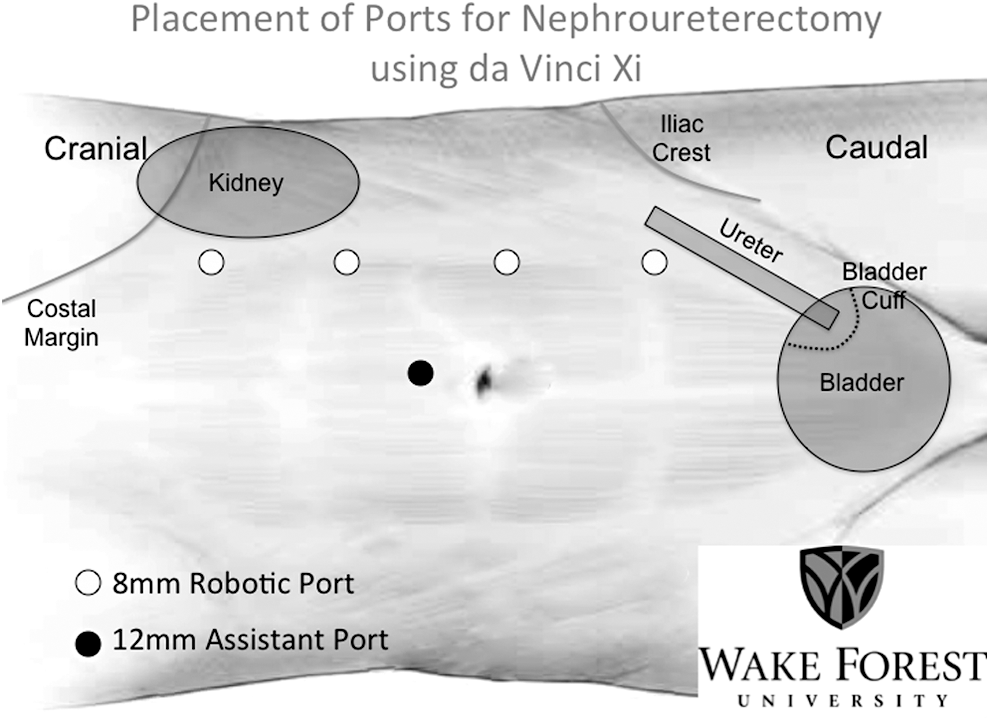
Port placement for da Vinci Xi.
Regardless of the robotic platform used, we always use the forth arm and long robotic cannulas, which help prevent collisions between the robotic arms and the assistant port.
Nephrectomy
The nephrectomy portion of the procedure is performed first in a standard manner. We typically clip the ureter under the location of the tumor immediately after ligating the renal artery to prevent urine build up before taking the hilum. This also helps prevent any tumor migration during mobilization of the kidney.
Lymph node dissection
All patients with evidence of lymph node enlargement on preoperative imaging are subject to lymph node dissection. For patients with high-grade tumors and T3 disease in the mid ureter or higher or for patients with bulky disease, we typically perform retroperitoneal lymphadenectomy as a standard template. For patients with disease in the distal ureter, we typically perform a pelvic lymph node dissection as a standard template.
Transition from upper to lower tract
Traditionally, the transition from upper tract to lower tract is the largest consideration when using the robotic platform for nephroureterectomy as many surgeons believe it necessary to dedock and reposition the patient-side cart. If docked perpendicular to the patient, it is unnecessary to reposition the base, and only minimal arm movements are required.
When using the XI platform, the camera is “hopped” from the second most cranial port to the third most cranial port for distal ureter and bladder cuff excision and reconstruction. The fourth arm is switched from the most caudal port to the most cranial port. The right arm port is switched from the third most cranial port to the fourth most cranial port. The left arm is switched from the most cranial port to the second most cranial port.
When using the S/Standard/Si platform, the camera remains in same position and the arms are switched. The fourth arm goes to the most cranial port. The left arm goes to the most lateral port and the right arm goes to the most inferior port.
Bladder cuff excision
Once the kidney is mobilized, the ureter is dissected distally toward the ureterovesical junction (UVJ). Using the Foley catheter, about 200 mL of distilled water is instilled to help distend the bladder to make dissection of the UVJ easier. Also, more recently, in select cases, we are instilling mitomycin just before cystotomy creation, the bladder is drained to help provide additional surgical space. During cystotomy the Foley is connected to intermittent suction (which is not a problem due to airseal) to prevent the chance of tumor spillage while the bladder is open. Before cystotomy, a stay suture is placed lateral to the UVJ using a barbed suture. This helps prevent retraction of the bladder mucosa once the specimen is removed. A cystotomy is performed ensuring a wide excision around the UVJ and the resulting defect is closed with the previously placed barbed suture in a running manner. After completion of the reconstruction, about 200 mL of saline is instilled to ensure the closure is watertight. 7
Results
Eighty-seven patients underwent robotic nephroureterectomy with bladder cuff excision and regional lymphadenectomy during the study period, 30 in group 1 and 57 in group 2. Preoperative variables are described in Table 1. Mean age was 70.3 vs 71.2 years for groups 1 and 2 (p = 0.79). Body mass index was 26.9 vs 27.3 kg/m2 for each group (0.91). American society of Anesthesiologists scores were also not significantly different between groups (0.0806). The procedure side, gender distribution, evidence of hydronephrosis on preoperative imaging, and smoking history were also not significantly different between groups (p values 0.1059, 0.5654, 0.7017, and 0.2588, respectively).
ASA = American Society of Anesthesiology; SD = standard deviation.
Perioperative variables are described in Table 2. Operative time was about 48 minutes shorter using the Xi platform (184.4 vs 232.09 minutes, p = 0.0035). Estimated blood loss (122.5 vs 156.5 mL, p = 0.87) and length of hospital stay (2.3 vs 2.6 days, p = 0.32) were similar between groups.
Pathologic variables are described in Table 3. Tumor size, tumor location, positive margin rates, evidence of tumor necrosis, rates of concomitant carcinoma in situ, and percent of patients with high-grade pathology were similar between groups (p values 0.93, 0.2080, 0.3116, 0-.3515, 0.3480, and 0.3571, respectively). Rates of lymphovascular invasion (LVI) were significantly higher in group 2 (p = 0.0108) with 29.85% of patients noted to have LVI on final pathology vs 10% in group 1. Pathologic stage was also different with patients in group 1 having more pT3 disease.
CIS = carcinoma in situ.
Lymphadenectomy data are presented in Table 4. More patients in group 1 underwent regional lymphadenectomy per our indications mentioned previously (84.21% vs 54.41%, p = 0.0186). Lymph node positivity was similar between groups (p = 0.8129). Complication rates were similar between groups and are described in Table 5. The complication rate for group 1 was 13.33%, while in group 2 it was 17.85% (p = 0.5057). The distribution of Clavien grade complications was also similar between groups (p = 0.1861).
LND = lymph node dissection.
Cost Data are presented in Table 6. Anesthesia costs (the costs of personnel, anesthesia medications, and equipment) were lower in group 1 ($669.8 vs $1920, p = 0.00019). operating room (OR) time cost was lower as well, but not statistically significant (p = 0.0971). Post anaesthesia care unit costs and other costs (costs of inpatient stay, pharmacy, imaging, etc.) were similar between groups (p = 0.0747 and 0.724, respectively). Total costs were significantly less for group 1 ($4022 vs $5420.3, p = 0.00076).
OR = operating room; PACU = post anaesthesia care unit.
Discussion
The introduction of the robotic platform has transformed the technique of nephroureterectomy, allowing this extremely complex procedure to be performed by many more surgeons. Our team was the first to describe technique for single positioning during robotic nephroureterectomy. 5 Since then, a number of groups have described their modifications to this approach. 8 –10 Intuitive Surgical released its most recent fourth generation Xi robot in 2014. At this time, data are still sparse regarding the use of this new platform. Our group was also the first to describe the use of Xi for robotic nephrouretectomy, demonstrating modification in technique with initial results. 7 Darwiche and colleagues 11 have described their early results using the Xi platform in 10 patients, demonstrating reasonable operative times, blood loss, and length of stay. Argun et al. 12 described their initial experience with the Xi in two patients, demonstrating a modified flank position. To the best of our knowledge, this is the first study comparing the da Vinci Si to the Xi for use during robotic nephroureterectomy.
The present study did identify one significant advantage of the Xi over the previous robotic platforms. Operative time was found to be nearly 48 minutes shorter using the Xi, which is likely due to some of the enhancements of the system, including the ability to port “hop” the camera making it seamless transition from the upper tract to the lower tract, the ability to easily retarget the bladder cuff when transitioning to the lower tract. As with both platforms, we use a single docking technique, thus, physically moving the patient-side cart is not a factor. The finding of more patients undergoing regional lymphadenectomy in the Xi group is interesting, but partly due to biology of the disease, as more patients had T3 disease. Yet, despite the added step in nearly 30% of cases, the overall time was still less. In addition, while our team is experienced, we look at the possibility of a continuing learning curve being the possible cause for shorter times in more recent cases (Fig. 3). A scatter plot of operative times over time was made with no indication of continuing learning curve. Other than operative time, there were no significant intraoperative or perioperative differences noted between groups.
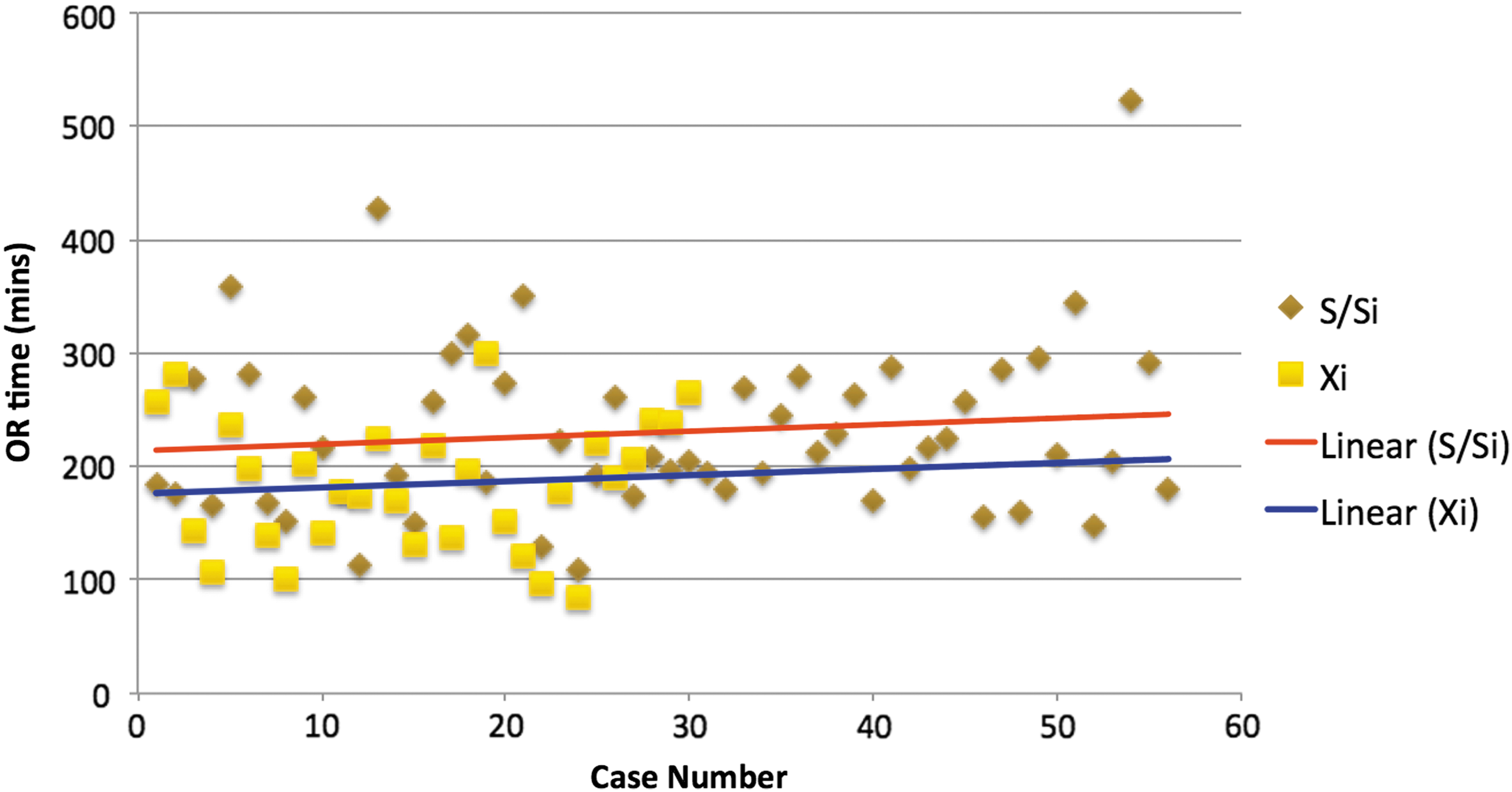
Operating time trends in the Xi and S/Si groups.
The overall complication rates were also similar between groups. There was a slight difference in the distribution of Clavien 13 classification complications, but this was not significant. In group 1, there were three Clavien II complications (chronic obstructive pulmonary disease [COPD] exacerbation, ileus requiring nasogastric tube placement, and acute renal failure not requiring intervention). There was also one Clavien IV complication in a patient who had an unrecognized duodenal injury requiring intensive care unit admission and total parenteral nutrition, but did not require surgical exploration. In group 2, there were three Clavien I complications (ileus without need for intervention), five Clavien 2 compilations (severe hyperglycemia requiring insulin drip, deep venous thrombosis requiring anticoagulation, COPD, exacerbation, non-ST elevation myocardial infarction requiring medical therapy, and an ileus requiring nasogastric tube placement), and two Clavien V complications (both found deceased and presumed to be postoperative myocardial infarctions given their medical comorbidities without autopsy per families).
Overall there was the finding of decreased costs for group 1 that is attributed to the cost of anesthesia. There was a significant difference in anesthesia costs of almost $1250, which is attributable to changes in supplier and equipment used by the Department of Anesthesia over the past 2 years. While this may account for some of the difference, it likely does not account for all of it. There is a trend toward significance with regard to OR time costs, which is likely related to the decreased surgical time using the Xi platform. Other costs were similar between groups.
The main limitation of this study is the retrospective nature of the study and the nonrandomization of the patients between groups. Although, the sample sizes were not large, this is a preliminary study and describes our preliminary perioperative outcomes with both the da Vinci Si and Xi robotic platforms.
Conclusions
In conclusion, this initial comparison of the older da Vinci platforms with Xi robotic platform does demonstrate shorter operative times, but without any immediate perioperative advantages. This study also reveals a trend toward lower overall hospital costs due to less OR cost because of shorter operative time and anesthesia costs at our center at the time of study. Larger studies with randomization involving multiple institutions are necessary to determine if this advancing technology truly does improve the outcomes.
Footnotes
Author Disclosure Statement
No competing financial interests exist.