
Abstract
Introduction:
In the era of minimally invasive surgery, endoscopic and percutaneous interventions for urinary tract stones have become a mainstay, and the need for open stone surgery (OSS) has decreased. We sought to determine the contemporary incidence of OSS among urologists in the United States.
Methods:
Case logs submitted for certification to the American Board of Urology from 2005 to 2015 were queried for Current Procedural Terminology codes relevant to OSS. Cases were analyzed for the associated practice type, practice area population, geographic region, provider subspecialty, and certifying status of the reporting urologist.
Results:
A total of 334 cases of OSS were identified, with 73.4% performed by urologists self-identified as generalists. The most common subspecialists performing OSS were endourologists (12.3%). Most cases were done in the private practice setting (80.4%), and in practice areas with populations exceeding 1,000,000 (43.2%). OSS was more commonly reported by urologists applying for recertification than initial certification. Thirty open stone cases were reported each year on average, and there was no decrease in stone cases over time based on linear regression analysis (R 2 = 0.06). OSS was most commonly performed in the Western Section of the American Urological Association (AUA) (25.1%) and least commonly performed in the Northeastern Section (1.5%). A chi-square analysis was performed, and the Western Section had a significantly higher number of OSSs than expected as its urologists represent only 17% of the total AUA membership (p < 0.01). The Northeastern Section comprises 7% of the AUA membership but only performed 1.5% of OSSs that were significantly lower than expected (p < 0.001).
Conclusions:
Domestic performance of OSS remains stable. It is unclear as to whether the majority of these cases could be served by less-invasive technologies or whether the volume represents a true nadir. Future work may be warranted to assess attitudes, training, and feasibility of minimally invasive stone management in areas where OSS is most common.
Introduction
M
Methods
Urologists seeking initial certification or recertification by the American Board of Urology (ABU) are required to submit case logs for procedures performed for a 6-month period. Deidentified data from case logs submitted from 2005 to 2015 were reviewed, specifically focusing on Current Procedural Terminology (CPT) codes relevant to open surgical procedures for upper urinary tract stone disease (50060, 50065, 50070, 50075). The data were further analyzed for information relevant to description of procedures, physician gender, initial vs recertification, self-reported urologic subspecialty (general, endourology, urolithiasis, female, oncology, pediatrics, or infertility), practice setting (private practice, academic, Veterans Administration/military, or mixed), full or part time employment, population of practice area, American Urological Association (AUA) section of practice location, and initial year of ABU certification if applicable.
Our aim was to determine the trend in performance of OSS and associated factors among urologists submitting case logs for ABU certification. Chi-square analysis was used to compare the volume of OSS performed in each AUA section relative to proportion of overall membership as of September 2016. Linear regression analysis was applied to assess the trend over time for OSS.
Results
A total of 334 cases of OSS were identified out of 107,277 cases in the ABU data set. Most OSS cases (73.4%) were performed by general urologists. A total of 12.3% of all cases were performed by endourologists. Complete breakdown by self-reported urologic subspecialty is shown in Figure 1. Most OSSs were done in the private practice setting (80.4%) followed by academic practices (9.5%). Figure 2 shows open stone case distribution by practice setting. In terms of population size of practice area, OSS was most commonly performed in large cities with populations >1 million. It was least common in cities with populations 250,001 to 500,000 (Fig. 3). There was no significant difference in CPT coding based on specialty (p = 0.67), practice type (p = 0.89), or practice area size (p = 0.92). Case breakdown by CPT code is listed in Table 1.

Open stone surgeries by subspecialty classification.
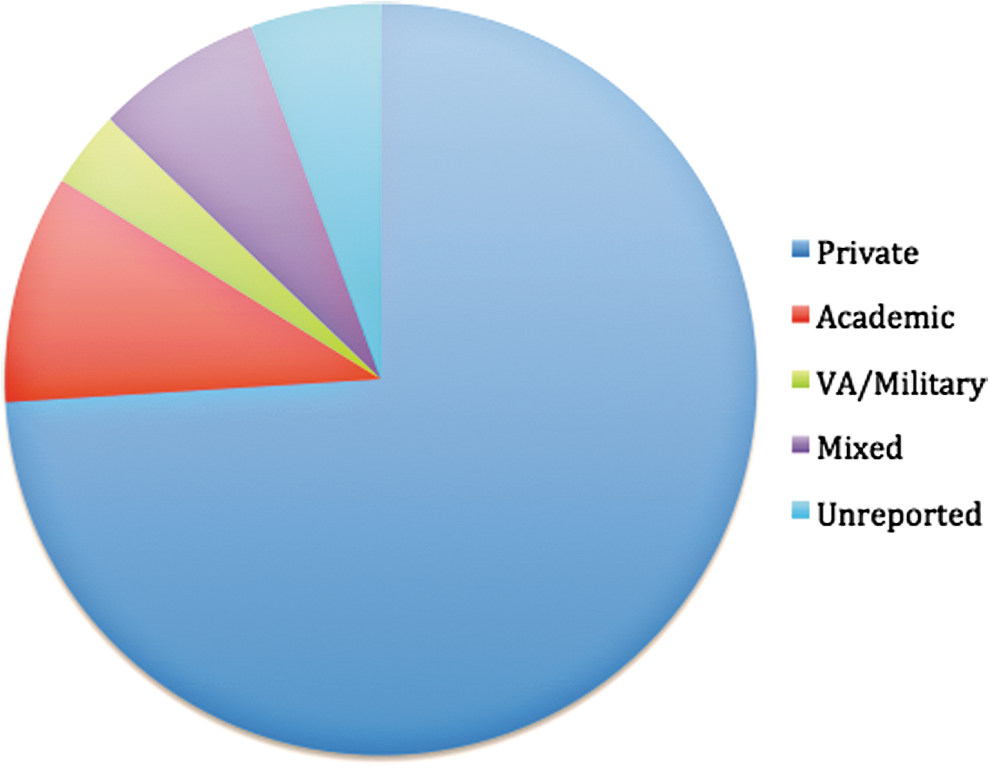
Open stone surgeries by practice type.
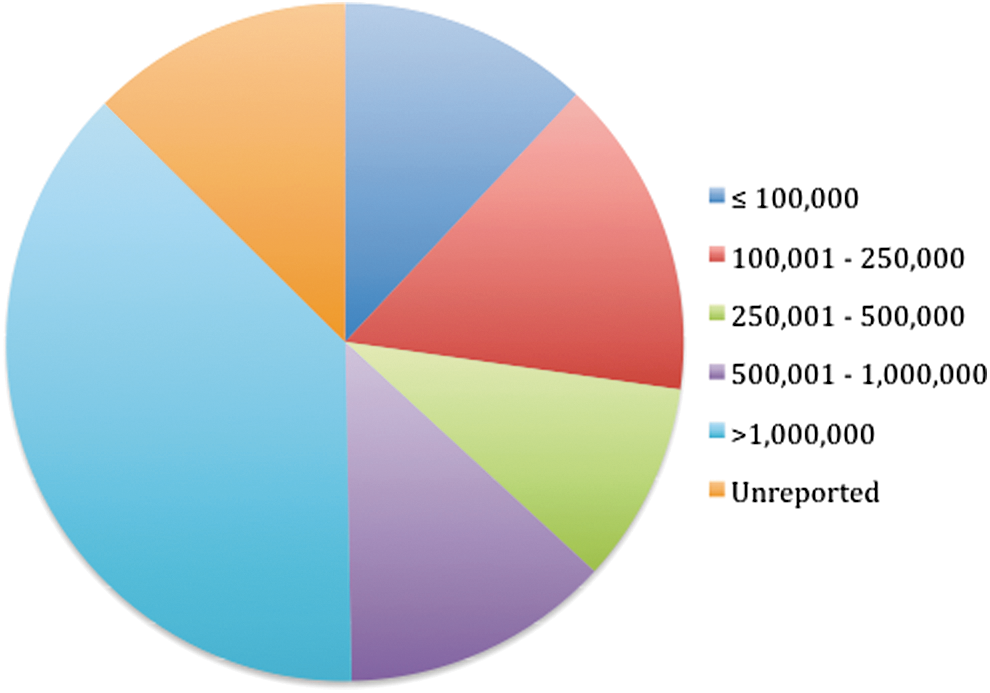
Open stone surgeries by population size of town/city.
CPT = Current Procedural Terminology.
OSS was more often reported by urologists applying for ABU recertification (55%) than for initial certification (45%). Thirty OSS cases were reported each year on average during the study period of 2005 to 2015. This is shown in Figure 4. Based on linear regression analysis, the number of OSS cases per year remained consistent over time (R 2 = 0.062).

Open stone cases per year.
OSS was most commonly performed in the Western Section of the AUA (25.1%) and least commonly performed in the Northeastern Section (1.5%). A chi-square analysis was performed comparing the number of OSSs performed in each section vs the number expected based on AUA sectional membership. The Western Section not only had the highest number of cases reported but it also had a significantly higher number than expected as its urologists represent only 17% of the total AUA membership (p < 0.05). The Northeastern Section comprises 7% of the AUA membership but only performed 1.5% of OSSs, which was significantly lower than anticipated (p < 0.05). Full results are listed in Table 2.
AUA = American Urological Association.
Discussion
Our study demonstrates that, contrary to our hypothesis, the number of OSS cases performed annually in the United States is stable (Fig. 4). Most OSSs are performed by general urologists in private practice. Plausible explanations for this finding may include a lack of subspecialty training to perform complex percutaneous nephrolithotomy (PCNL) as well as inadequate access to necessary instrumentation, imaging, interventional radiology assistance, or other patient care resources. We found it surprising that OSS was more common in more populated areas. In a review of ABU data by Jayram and Matlaga, as of 2012 only 20.4% of urologists reported self-performance of percutaneous access. 5 The same report noted that PCNL was more often performed by initially certifying urologists (53%) than by recertifying urologists (29%), potentially because of increased residency training in techniques of percutaneous access. In a 2006 survey of member urologists within the North Central Section of the AUA, 61% reported having been trained to perform OSS during urology residency. 6 We acknowledge that the use of data that is self-reported to the ABU may show selection bias since urologists can choose which consecutive 6 months of data to report. This could artificially increase or decrease the number of open stone cases reported and represents a weakness of this particular data set.
Literature regarding the pseudo-contemporary practice of OSS is sparse, with two seemingly relevant publications, both from the same institution. 1,7 The first reviewed data from 1989 to 1990, just after the introduction of the Dornier HM3 lithotripter. In that report, 893 procedures were performed to treat upper tract stones, 37 (4.1%) of which were done through an open approach. Surgical indications in those cases included failure of endoscopic management, infundibular stenosis, ureteropelvic junction obstruction, obstructed megaureter, large volume of ureteral stone(s), struvite calculus in a poorly functioning segment, morbid obesity, severe renal malrotation, and stone removal in tandem with another open procedure. Surgical procedures included ureterolithotomy, anatrophic nephrolithotomy, pyelolithotomy, partial nephrectomy, and nephrolithotomy with bowel segment interposition. 1 The second publication described OSS performed from 1998 to 2001. By that time, only 7 of 986 stone-removing procedures (0.7%) were performed in an open manner. Indications included symptomatic calculi in anterior caliceal diverticula, large volume of stone in a nonfunctional lower pole, large volume staghorn calculi associated with infundibular stenosis and massive dilation of pelvicaliceal system, and multiple failed endoscopic attempts at a referring institution. Variants of open surgery performed included anatrophic nephrolithotomy with or without ablation of caliceal diverticula and lower pole heminephrectomy. 7 These publications demonstrated that the incidence of OSS at a single high-volume, tertiary care institution decreased from 1990 to 2001.
Data from 1989 to 1999 reported rates of OSS as 2% to 5%, 2 –4 whereas a review of Medicare data from 2001, 2004, 2007, and 2010 revealed a rate of 9%, with no significant change between 2001 and 2010. 8 Thus, Medicare data and our current review suggest that although individual institutions may note a decline in OSS, national data suggest a stable rate of performance. Internationally, however, trends may be different. In the United Kingdom, for example, Turney and colleagues noted a decline in reported OSSs from 278 cases in 2000 to 47 cases in 2010. 9 It is unknown whether this represents a true decrease, rather than an artifact of reporting.
Conclusions
Domestic performance of OSS remains stable, and it is most commonly performed by recertifying general urologists in the western United States. It is unclear as to whether the majority of these cases could be served by less-invasive technologies or whether the volume represents a justified nadir. Future work may be warranted to assess attitudes, training, and feasibility of minimally invasive stone management in areas where OSS is most common. Data from such efforts may be used to optimally allocate educational resources for improved delivery of care.
Footnotes
Acknowledgments
This work was made possible by a grant from the American Urological Association Leadership Program, and the data were obtained from the American Board of Urology.
Author Disclosure Statement
No competing financial interests exist.