
Abstract
Introduction:
Reusable ureteroscope durability and need for repair are significant sources of expense and inefficiency for patients and urologists. Utilization of LithoVue™, a disposable flexible digital ureteroscope, may address some of these concerns. To identify its economic impact on clinical care, we performed a micro-cost comparison between flexible reusable fiberoptic ureteroscopes (URF-P6™) and LithoVue.
Patients and Methods:
For this prospective, single-center micro-costing study, all consecutive ureteroscopies performed during 1 week each in July and August 2016 utilized either URF-P6 or LithoVue ureteroscopes respectively. Workflow data were collected, including intraoperative events, postoperative reprocessing cycle timing, consumables usage, and ureteroscope cost data.
Results:
Intraoperative data analysis showed mean total operating room time for URF-P6 and LithoVue cases were 93.4 ± 32.3 and 73.6 ± 17.4 minutes, respectively (p = 0.093). Mean cost of operating room usage per case was calculated at $1618.72 ± 441.39 for URF-P6 and $1348.64 ± 237.40 for LithoVue based on institutional cost rates exclusive of disposables. Postoperative data analysis revealed costs of $107.27 for labor and consumables during reprocessing for URF-P6 cases. The costs of ureteroscope repair and capital acquisition for each URF-P6 case were $957.71 and $116.02, respectively. The total ureteroscope cost per case for URF-P6 and LithoVue were $2799.72 and $2852.29, respectively.
Conclusions:
Micro-cost analysis revealed that the cost of LithoVue acquisition is higher per case compared to reusable fiberoptic ureteroscopes, but savings are realized in labor, consumables, and repair. When accounting for these factors, the total cost per case utilizing these two ureteroscopes were comparable.
Introduction
F
LithoVue™ (Boston Scientific, Marlborough, MA), a single-use digital disposable flexible ureteroscope, was released in October 2015. 9 Cadaveric models 10 and kidney stone patient case studies 11,12 have demonstrated that LithoVue demonstrates image quality and maneuverability comparable to existing reusable ureteroscopes. Additionally, we previously showed that URS performed by LithoVue was associated with 13 minutes shorter procedure time and 13% less postoperative complication rate compared with reusable fiberoptic flexible ureteroscope. 13 One study has estimated that LithoVue cost-effectiveness might vary depending on case volume, suggesting need for detailed cost analysis. 14
Micro-costing is a cost analysis methodology that enables precise economic assessment of resources used for a given process. It has been applied successfully to measure cost-effectiveness for many medical treatments, including surgical and intensive care unit outcomes. 15 –17 Its bottom-up approach with time-motion analysis provides direct measurement of activity duration for relevant steps and assigns their cost per unit. 18
In this study, we conducted a prospective micro-costing analysis to compare the economic impact between disposable digital LithoVue and reusable flexible fiberoptic ureteroscopes.
Patients and Methods
Study design
This was a prospective, single-center, micro-costing study conducted at University of California, San Francisco (UCSF). Study design is outlined in Figure 1.
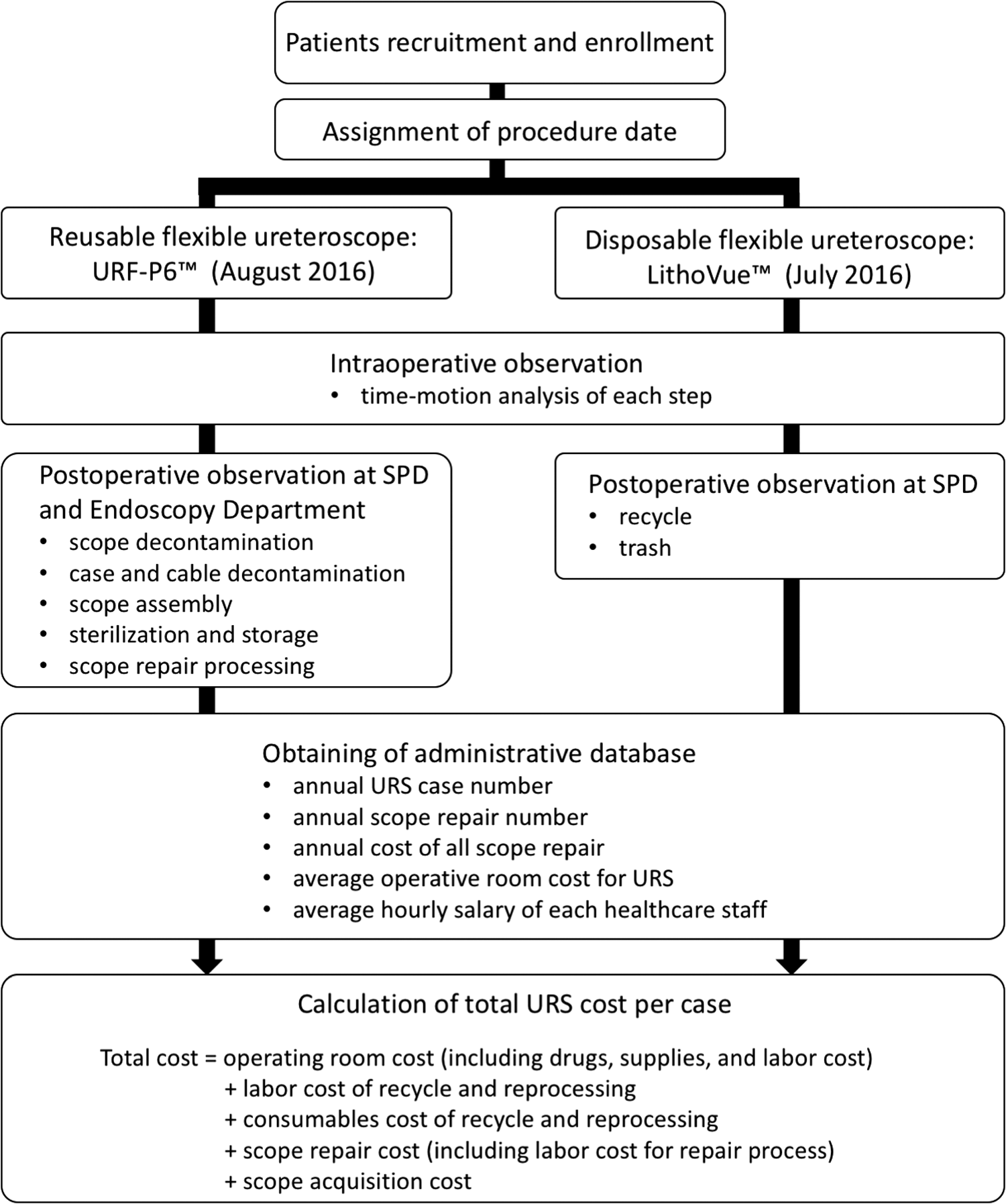
Micro-costing study design. For cases performed using either reusable or disposable flexible ureteroscopes, intra- and postoperative observation was performed by three engineers experienced in process measurement. Additional data were provided by institutional databases. Total cost per case consisted of operating room cost, labor and consumables cost for disposal and reprocessing, ureteroscope repair cost, and ureteroscope acquisition cost. SPD = sterile processing department; URS = ureteroscopy.
After approval by the Institutional Review Board (CHR 14-14533), consecutive flexible URS procedures were enrolled for this study during 1 week each of July and August 2016. Two endourologists (M.L.S. and T.C.) performed all procedures with either disposable digital LithoVue or reusable flexible fiberoptic (URF-P6™; Olympus, Tokyo, Japan) ureteroscopes. Included were patients older than 18 years with upper urinary stones of any size. Excluded were antegrade and staged URS procedures, and URS concurrently performed with other procedures.
Patients, time-motion, and micro-costing data collection
LithoVue cases were conducted during 1 week in July 2016 and URF-P6 cases were conducted during 1 week in August 2016. During each week, flexible URS was performed on two nonconsecutive days. Intraoperative data collection included duration of each surgical step in addition to other clinical parameters. Postoperative data collection included details regarding reprocessing and disposal cycles, accounting for labor duration, and consumable and supply data from the sterile processing and requisition departments. Clinical information from all patients was prospectively captured in ReSKU™—Registry for Stones of the Kidney and Ureter, 19 which is an automated stone registry tied to electronic medical records and Research Electronic Data Capture (REDCap) 20 primarily based at UCSF.
Each ureteroscope cost per case was calculated as follows: (operating room cost) + (labor costs related to reprocessing) + (consumable costs for reprocessing) + (ureteroscope repair costs) + (ureteroscope acquisition cost). Operating room cost was calculated based on institutional data specific to URS and included labor and consumable costs. Labor cost was calculated based on average hourly salaries provided by our institution, accounting for both employee salary and benefits. Ureteroscope repair cost per case was calculated from the total annual repair expenses of the previous 12 months preceding the study period divided by the number of flexible URS cases done during that time period. Ureteroscope acquisition costs were derived from the actual capital cost spent to acquire the current fleet of 12 ureteroscopes owned by the institution divided by the number of procedures performed with each ureteroscope during a three-year period, which reflected the average ureteroscope lifespan. All costs were described in U.S. dollars.
Statistical analysis
Continuous, normally distributed variables were expressed with means (standard deviation) whereas non-normally distributed variables were expressed with medians (25% interquartile range [IQR], 75% IQR). Categorical variables were presented with frequency (percentage). Two sample t tests and Mann-Whitney U tests were used to identify differences between groups. Categorical variables were compared using Fisher's exact test. Differences were considered statistically significant at α < 0.05. All statistical analyses were performed using EZR for R (R project). 21
Results
A total of 23 URS cases were enrolled into this study: 14 cases utilized URF-P6 and 9 cases utilized LithoVue. Table 1 details patient and intraoperative characteristics and operative surgeons' evaluation comparing their experience using reusable vs disposable flexible ureteroscopes. There were no statistically significant differences between URF-P6 and LithoVue cases with regard to demographics. Twelve cases were performed to treat upper urinary tract stones while eleven cases were performed for diagnostic purposes. Ureteral access sheathes were used in 12 cases (52%). For stone treatment procedures, six were renal stone (41%), four of which were lower pole stones. Five cases were ureteral stones (34%), and four cases had stones in both the kidney and ureter (27%). Median overall stone burden was 10.0 mm [8.0, 12.0]. For nineteen cases (83%) supervised urological residents were the primary ureteroscope handlers.
Only cases performed for treatment of urinary stones are included for these measures.
BMI = body mass index; SD = standard deviation; IQR = interquartile range.
The duration of each procedure step is compared and described in Table 2. The mean duration of ureteroscope setup in the LithoVue group was 2.5 ± 2.0 minutes; significantly shorter than 5.0 ± 2.4 minutes in the URF-P6 group (p = 0.013). Mean ureteroscope utilization time (24.8 ± 7.5 vs 33.7 ± 26.5 minutes, p = 0.31), mean operating room time (73.6 ± 17.4 vs 93.4 ± 32.3, p = 0.09), and total procedure time (43.2 ± 14.8 vs 52.2 ± 32.3 minutes, p = 0.42) were shorter in the LithoVue compared to the URF-P6 group though the differences did not reach statistical significance.
Table 3 outlines the differences in reprocessing and disposal cycles between the URF-P6 and LithoVue groups. The average labor time needed for URF-P6 reprocessing cycles was 20.9 minutes for cable/ureteroscope decontamination, 19.6 minutes for ureteroscope cleaning and quality check, 6.5 minutes for cable/ureteroscope assembly, and 10.3 minutes for cable/ureteroscope sterilization. In addition, an average of 265.6 minutes of time was needed for automated machine processes to finish during each ureteroscope reprocessing cycle. Based on these times, total labor cost for each URF-P6 reprocessing cycle was calculated at $44.23. In contrast, the average labor time for LithoVue disposal was 4.4 minutes for recycling and 0.3 minutes direct trash disposal. Total labor cost to dispose of a LithoVue was therefore calculated to be $3.65. The supplies and consumables costs related to each cycle of URF-P6 reprocessing were gathered from each department where the activities took place (Table 3). Supplies (defined as disposable products usable for multiple activities) and consumables (defined as disposable items discarded after each processing cycle) are detailed in Supplementary Table S1 (Supplementary Data are available online at
Costs ($) are shown in U.S. dollars.
The overall URS cost per case is summarized in Figure 2. The overall operating room cost of using URF-P6 vs LithoVue was $1618.72 ± 441.39 and $1348.64 ± 237.40, respectively, based on institutional operating room cost per minute and procedure times described above (p = 0.093). The total labor cost related to URF-P6 was $49.99, including an amortized cost for reprocessing an additional, unusable ureteroscope on 13% of cases due to ureteroscope damage or breaches in sterility. The costs of consumables, repairs, and ureteroscope acquisition per URF-P6 case were $57.28, $957.71, and $116.02, respectively whereas the cost per ureteroscope was $1500 and labor cost for disposal was $3.65 in the LithoVue group. Compiling these costs, the total URF-P6 and LithoVue cost for use per case were $2799.72 and $2852.29, respectively.
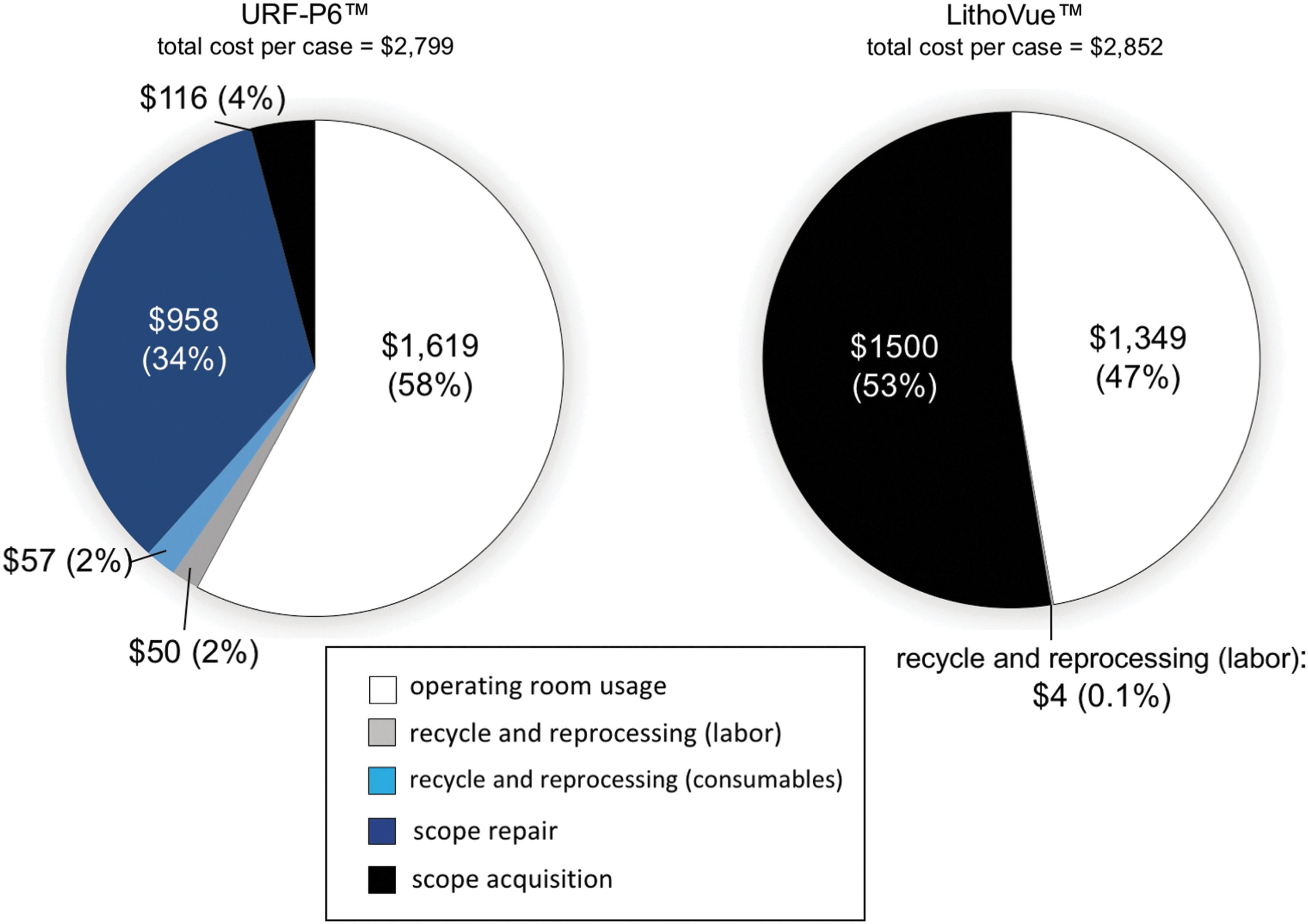
Comparison of total cost per case utilizing reusable fiberoptic to disposable digital flexible ureteroscopes. Total cost per case for URF-P6™ and LithoVue™ were $2799 and $2739, respectively. The breakdown costs for each step are shown using both average actual costs and percentage of total cost. URF-P6 = reusable fiberoptic flexible ureteroscope; LithoVue = disposable digital flexible ureteroscope.
Discussion
Based on a micro-costing analysis, our study has demonstrated a comparable overall cost per case between reusable and disposable flexible ureteroscopes. Factors in using disposable ureteroscopes that impacted this cost analysis were the shorter ureteroscope setup and disposal time in addition to shorter operating room times compared to reusable ureteroscopes. Additionally, using disposable ureteroscopes eliminated reprocessing time and costs. Reprocessing a URF-P6 took an average of 57.2 minutes in direct labor time and 265.6 minutes in automated machinery time with a resultant cost of $107.27 per ureteroscope. LithoVue disposal cost was $3.65 by comparison. Comparison of the total cost breakdown for each type of ureteroscope used revealed that repair cost for URF-P6 and ureteroscope acquisition cost for LithoVue comprised the majority total ureteroscope cost per case. And while the repair cost per case for reusable ureteroscopes was less than ureteroscope acquisition cost per case for disposable ureteroscopes, when accounting for the differences in operating room time and recycling and reprocessing, use of each ureteroscope type appeared cost equivalent at our institution. Keeping these differences in mind, accounting for each of these factors can help in making institutional decisions about which ureteroscope is most cost effective for use.
While this study only showed a statistically nonsignificant difference in operating room time and cost between URF-P6 and LithoVue cases, this difference may be of clinical significance. It is possible that this difference was due to factors such as ureteral access sheath use or stone location. This study demonstrated a nonstatistically significant impact of these two factors on procedure time, but our study was underpowered to identify etiologies for operative time differences. Based on previous publications, we might expect the use of access sheaths to reduce operative times. 22,23 We previously demonstrated that in a matched pair cohort study of 115 cases utilizing LithoVue, these procedural time differences were magnified and preserved. LithoVue utilization was associated with a 15.5 minute shorter operating room duration. 13 Given the smaller stone burden and larger proportion of diagnostic URS in this study, we would have expected to find a smaller difference in operating room time between the two types of ureteroscopes. A 20 minute difference was larger than what we anticipated. While this time difference was in a similar range to previous studies, our case numbers may have been underpowered to demonstrate statistical significance. However, given the similarity to previously published studies, we felt it reasonable to calculate the overall operative room costs using this time difference.
One key consideration for any cost analysis is that many factors are institution-specific and therefore should be weighed to understand how applicable our results are for other institutions. One example is our reusable ureteroscope repair cost per case. This cost of $957.71 was calculated using the total annual ureteroscope repair cost divided by the annual number of URS cases. These data were provided from our institutional records. Total annual ureteroscope repair cost reflected a sum of average ureteroscope repair cost, and pre- and postrepair processing labor costs. At our institution we do not use a manufacturer's warranty, but rather utilize a third party repair service. This might have increased our ureteroscope repair cost per case compared to other institutions as others have demonstrated the potential cost difference between third party and original equipment manufacturer repairs. 24
Reusable flexible ureteroscope repair costs will vary among institutions, depending on how costs are amortized and what repair contracts exist between institutions and vendors. Previously published studies report a wide range in repair costs, from as low as $121 to as high as $8477 per ureteroscope per case. 7,25 –27 Our repair cost per case was within range compared to other studies. Notably, we included labor costs related to ureteroscope repair. We included it to identify a comprehensive reflection of actual repair costs. Likewise, the calculation of ureteroscope acquisition cost per case was based on institutional amortization characteristics. We delivered it as $116.02 based on initial purchase cost for 12 URF-P6 ureteroscopes, divided by the total number of URS cases during a lifespan of a ureteroscope estimated by 3 years based on our institutional data. Ureteroscope lifespan and amortization would certainly change depending on institutional volume and ureteroscope care protocols.
Our study demonstrates a comparable cost between reusable and disposable ureteroscopes and should be contextualized with other published literature. One study has estimated that the cost-benefit ratio of LithoVue is favorable compared with reusable ureteroscopes during the first 98 cases, but this cost effectiveness decreases after the 99th case. 14 This analysis was based on projected estimates. Our institution performed 331 URS procedures during the year before the study period, and our analysis was based on annual use amortized to performance during two study weeks and not projected estimates. Similar to the previous report, our relatively high case volume might underestimate costs for reusable ureteroscope utilization. Reusable ureteroscope cost would increase in institutions with smaller case volume.
One important design characteristic of our study that should be considered is the fact that we compared LithoVue, a disposable digital ureteroscope, to a reusable fiberoptic ureteroscope. While some studies have addressed the comparability of LithoVue's image quality with conventional reusable ureteroscopes, 9,11 previous studies comparing digital to fiberoptic reusable ureteroscopes have shown a 9-minute shorter fragmentation time with digital ureteroscope use. 28 This time difference may be explained by different optic sensors in the two ureteroscopes. Therefore, an institution considering whether a disposable ureteroscope would maintain a cost equivalency compared to their current ureteroscope fleet should consider whether they are switching from a digital or a fiberoptic reusable ureteroscope to the disposable digital ureteroscope.
Additionally, although we detailed the breakdown cost data between reusable and disposable ureteroscopes, one limitation of this study was our inability to perform statistical analysis on procedural costs comparing the two groups due to heterogeneity among observing a limited number of procedures. We elected to collect a greater granularity of detail on timing and cost for a fewer number of case observations to provide a micro-costing approach to cost analysis. The tradeoff was that while we obtained high levels of detail on timing, supplies, and disposables necessary for ureteroscope use, case volume in both groups might be too small to achieve statistical significance in the difference for breakdown costs. Also, we obtained cost data for ancillary equipment utilized during the procedures as averaged values and combined them with operative room costs. Although the two groups were comparable with respect to patient and stone characteristics, a potential bias in ancillary device usage might affect our estimates. In addition, we elected to not include costs that were negligible (such as stocking, ordering, or shelving of the disposable ureteroscopes) or the green footprint costs into our micro-costing analysis. The impact of cleaning solutions and disposables disposal on the environment are complex to tease apart and not well characterized in any setting. Given our inability to accurately quantify them, we chose to forego their inclusion. We did not amortize cost for machinery used in reprocessing since this equipment was used for many years and across multiple services before the study period. Lastly, our study was based on data from a single institution, and our findings may not be applicable to all sites in different communities.
To our knowledge, this is the first micro-costing study carried out incorporating time-motion analysis to examine the impact of disposable ureteroscopes. Micro-costing is a useful approach to understand comprehensively the impact of new interventions on both total cost and cost per each step of a procedure. 15,29 There are several methods for carrying out micro-costing studies, 29 and our recent study successfully demonstrated feasibility of time driven activity based cost analysis without the need for a specialized engineering firm to collect data. 30 However, we performed direct observation by a third party engineering firm unrelated to any ureteroscope vendor to avoid potential observation bias. Our goal was to better understand the cost effectiveness of a disposable ureteroscope compared to the current paradigm of reusable ureteroscopes and provide a context to understand how they might be best utilized.
Conclusions
Our micro-costing analysis revealed comparable total cost per case between reusable and disposable flexible ureteroscopes. For reusable ureteroscopes, reprocessing and repairs require significant resources. While individual institutions vary with regards to case volume and cost control strategies, our study demonstrates that disposable ureteroscopes are a cost-effective alternative to reusable fiberoptic ureteroscopes.
Footnotes
Acknowledgment
This work was supported by an investigator-initiated educational grant from the Boston Scientific Foundation (T.C.). The sponsor played no direct role in the study planning, implementation, or data analysis.
Author Disclosure Statement
M.L.S. and T.C. serve as paid speakers and consultants for Boston Scientific Corporation and have received educational grant funding from Richard Wolf. M.L.S. has served as a paid speaker for the Karl Storz Company.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.