
Abstract
Objective:
Laparoendoscopic single-site surgery (LESS) is increasingly popular in urology. However, data on LESS radical cystectomy (LESS-RC) are immature, and no adequate comparative study has assessed conventional laparoscopic radical cystectomy (CL-RC) vs LESS-RC. The primary aim of this study was to compare efficiency and safety of LESS-RC and CL-RC for patients with bladder urothelial carcinoma (BUC).
Materials and Methods:
A retrospective and case-matched control comparative analysis was performed of patients who underwent LESS-RC (n = 54) and CL-RC (n = 108) from January 2011 to June 2015. Oncologic, complication and perioperative outcomes were collected and evaluated.
Results:
LESS-RC vs CL-RC was associated with less estimated blood loss (EBL; median, 270 vs 337.5 mL; p = 0.014), postoperative pain (median, 4.0 vs 6.0 scores; p = 0.001), and shorter convalescence (time to ambulation and oral intake, median, 2.5 vs 3 days; p = 0.002 and 5 vs 6 days; p = 0.004, respectively). No significant differences were noted for LESS-RC and CL-RC regarding the lymph node yield (median: 18 vs 20; p = 0.101). Median follow-up time was 33.5 months (interquartile range [IQR]: 23–41.3 months) and 33 months (IQR: 23–43 months) for the LESS-RC and CL-RC groups, respectively. No significant differences were noted for LESS-RC and CL-RC regarding estimated 24-month overall survival (86.7% vs 88.1%, p = 0.703), cancer-specific survival (88.3% vs 90.9%, p = 0.539), and recurrence-free survival (80.2% vs 87.5%, p = 0.619), even when substratified according to tumor stage (pT3 or higher) and lymph node status (pN+). Early, late, and 90-day overall complication rates were similar. In multivariate analyses, LESS-RC was not associated with recurrence and worse survival rates, but was associated with 90-day overall complications.
Conclusions:
This study demonstrated that LESS-RC and CL-RC have comparable efficiency and safety for patients with BUC. Compared to CL-RC, LESS-RC was with less postoperative pain, lower EBL, and more rapid convalescence, but was associated with 90-day overall complications.
Introduction
R
In 2009, White and colleagues were the first to report laparoendoscopic single-site RC (LESS-RC), and the technique has garnered much attention since then. 6 In recent years, a number of investigators have begun to report case series of LESS-RC. Their landmark studies demonstrated the surgical feasibility of LESS-RC with the potential of less postoperative pain, lower estimated blood loss (EBL), more rapid convalescence, and better cosmesis. 6 –10 However, its actual role in the field of minimally invasive surgery remains to be determined because of absence of mature data on efficiency and safety. 11
To critically assess the efficiency and safety of LESS-RC, we conducted this matched case–control analysis. The primary aim was to evaluate and compare survival and complication rates for LESS-RC and conventional laparoscopic radical cystectomy (CL-RC). Our secondary objective was to show the association of LESS-RC with survival, recurrence, and complications and compare the perioperative outcomes of these techniques.
Materials and Methods
Study population
This study was approved by an institutional review board. Between January 2011 and June 2015, 54 consecutive patients with BUC received LESS-RC. To minimize potential confounding bias, 108 patients who underwent CL-RC (January 2011 to June 2015) were matched 2:1 with 54 LESS-RC patients based on clinical tumor stage. Data were obtained and gathered in a secured database for retrospective analysis. All surgeons in this study were experienced in performing RC.
Indications for surgery were identical in the LESS-RC and CL-RC groups. Inclusion criteria comprised patients with recurrent or high-grade nonmuscle-invasive or muscle-invasive BUC without evidence of extravesical spread or metastatic disease on preoperative imaging (chest radiographs and CT scans of the abdomen and pelvis).
Exclusion criteria were radiologically or clinically advanced (pT4) or metastatic disease, history of extensive prior abdominal or pelvic operations, pelvic radiotherapy, severe cardiopulmonary dysfunction, uncorrectable coagulopathy, any contraindication for Trendelenburg position, or unwillingness to undergo RC.
Surgical procedures and adjuvant therapy
LESS-RC was performed according to our previously described approach. 12,13 We used a home-made single-port device consisting of two stretchable rubber rings and a size 7.5 surgical glove. The device was inserted through a 4-cm midline incision below the umbilicus, and three 5-mm trocars (as assistant ports) and two 12-mm trocars (as camera port and assistant port) were introduced through the glove's fingers. A 10-mm, 30° laparoscope, prebent laparoscopic instruments (clamp and irrigation suction), and standard laparoscopic instruments were used during the procedure. The CL-RC technique has been described previously. 4 A five-port, fan-shaped transperitoneal approach was used, and subsequent procedures were same as in LESS-RC.
All patients underwent standard or extended (template up to the aortic bifurcation) LND based on frozen lymph node evaluation during the procedure. Men underwent cystoprostatectomy and women underwent cystectomy and pelvic exenteration. Once RC was completed, all urinary diversions were performed with an extracorporeal approach; types included orthotopic neobladder, Bricker ileal conduit, and cutaneous ureterostomy.
Indications for adjuvant therapy after operation included locally advanced disease (pT3 or higher), positive surgical margin, or evidence of lymph node metastases on final pathology with a gemcitabine–cisplatin combination chemotherapy regimen.
Data collection and assessment
The following outcomes were collected and analyzed from chart review by a clinical researcher with no association with the operations: patient baseline characteristics and perioperative outcomes such as operative time, EBL, blood transfusion, time to ambulation, time to oral intake, length of hospital stay, and visual analog pain score (VAPS). Oncologic outcomes such as pathologic stage, grade, surgical margin status, lymph node yield and status, and recurrence were also assessed.
Complications were classified as early (≤30 days) and late (31–90 days), depending on the date of onset, and were graded as minor (grade 1–2) or major (grade 3–5) according to the Clavien-Dindo classification system. 14
Tumors were staged and graded according to the 2002 American Joint Committee on Cancer TNM staging system and the 2004 World Health Organization/International Society of Urologic Pathology consensus classification, respectively.
Pathologic stage subgroups were defined as organ confined (pT2 or lower) and nonorgan confined (pT3 or higher) and as lymph node negative and positive (pN+).
Recurrence was defined as tumor relapse in the first local field, regional lymph nodes, and/or distant new lesion. Overall survival (OS) was defined as the time from the beginning of the treatment until death related to tumor or other cause. Cancer-specific survival (CSS) was defined as the time to death caused by tumor, and recurrence-free survival (RFS) was defined as time from date of treatment to recurrence, based on pathologic or radiologic evidence.
Follow-up
Patients were followed postoperatively at least every 3 to 4 months for the first year, biannually for the second year, and annually thereafter. Follow-up data were obtained by either chart review or telephone contact. Follow-up visits consisted of physical examination, serum biochemical evaluation, abdominal ultrasonography, intravenous pyelography, and chest X-rays. CT scanning of abdomen and pelvis was performed 6 months postoperatively and annually thereafter. Bone scans, magnetic resonance imaging, or cystoscopy were performed if clinically indicated.
Statistical analysis
The Kaplan-Meier method was used to estimate survival for the two groups and within subgroups, and the log-rank test was used for comparison. Multivariate Cox and logistic regression analyses were used to identify the association of LESS-RC with survival, recurrence, and complications. In multivariate analysis, results were reported as hazard ratio (HR) or odds ratio (OR) with their 95% confidence intervals (CIs).
Categorical variables were reported as percentages, and continuous variables were reported as median and interquartile range (IQR). Differences between groups were compared by chi-square or the Mann-Whitney U test. For all statistical analyses, two-sided p < 0.05 was considered statistically significant. Statistical analyses were performed using SPSS v.21 software (IBM Corp., Armonk, NY).
Results
Patient characteristics
Patient characteristics are summarized in Table 1. The LESS-RC group had more men and lower body mass index. There were no statistically significant differences in other baseline characteristics between groups.
No patients received neoadjuvant chemotherapy. Bolded text indicates statistical significance.
ASA = American Society of Anesthesiologists; CL-RC = conventional laparoscopic radical cystectomy; IQR = interquartile range; LESS-RC = laparoendoscopic single-site radical cystectomy.
Perioperative outcomes
Perioperative outcomes are summarized in Table 2. No patient required conversion to open surgery.
No nerve-sparing procedures were performed. Bolded text indicates statistical significance.
LND = lymph node dissection; VAPS = visual analog pain score.
We observed significantly longer operative time for LESS-RC vs CL-RC (median: 384 vs 298 minutes, p < 0.001). Statistically significant EBL was observed in the CL-RC group compared with LESS-RC (median: 337.5 vs 270 mL; p = 0.014). LESS-RC patients had lower VAPS during the first 3 days after operation (median score: 4 vs 6; p = 0.001) time to ambulation [median: 2.5 vs 3.0 days; p = 0.002] and time to oral intake [median: 5.0 vs 6.0 days; p = 0.004] were significantly shorter for the LESS-RC group than the CL-RC group.
Complications
Early, late, and 90-day complications are summarized in Table 3.
Patient with more than a single complication, only the highest grade was considered for statistical analysis. Bolded text indicates statistical significance.
Overall, 32 LESS-RC patients (59.3%) and 47 CL-RC patients (43.5%) experienced a complication within 90 days of surgery, with no significant differences observed between groups for major complications (16.7% vs 20.4%; p = 0.572), overall complications (59.3% vs 43.5%; p = 0.059), and readmission rate (16.7% vs 17.6%; p = 0.883). Infectious and gastrointestinal complications were the most common complications for the two groups.
Multivariate logistic regression analysis identified an association of LESS-RC with 90-day overall complications (OR: 0.327 [95% CI: 0.133, 0.807]; p = 0.015) after controlling for patient and tumor characteristics and intervention confounders (Table 4).
Data are for 162 patients with bladder urothelial carcinoma treated with LESS-RC and conventional laparoscopic radical cystectomy. Bolded text indicates statistical significance.
ASA = American Society of Anesthesiologists classification; BMI = body mass index; CI = confidence interval; OR = odds ratio; PSM = positive surgical margin.
Oncologic outcomes
The final pathologic data are shown in Table 5.
CIS = carcinoma in situ; PCa = prostate cancer.
Median follow-up time was 33.5 months (IQR: 23–41.3 months) and 33 months (IQR: 23–43 months) for the LESS-RC and CL-RC groups, respectively. At last follow-up, 29 patients had experienced a recurrence, 11 (20.4%) in the LESS-RC group and 18 (16.7%) in the CL-RC group. In total, 30 patients had died from various causes, 11 in LESS-RC group (8 from tumor and 3 from causes unrelated to the tumor) and 19 in CL-RC group (12 from tumor and 7 from causes unrelated to the tumor). No patient died of coexisting prostate cancer, and no patient experienced a port-site recurrence.
Multivariate logistic regression analysis showed that LESS-RC was not associated with recurrence (OR: 0.562 [95% CI: 0.185, 1.709]; p = 0.310) after controlling for patient and tumor characteristics and intervention confounders (Table 6).
Data are for 162 patients with bladder urothelial carcinoma treated with LESS-RC and conventional laparoscopic radical cystectomy. Bolded text indicates statistical significance.
ASA = American Society of Anesthesiologists classification; BMI = body mass index; CSS = cancer-specific survival; HR = hazard ratio; OS = overall survival; RFS = recurrence-free survival.
Survival
Kaplan-Meier curves show OS, CSS, and RFS after LESS-RC and CL-RC for all patients (Fig. 1) and after stratification by tumor stage (pT3 or higher) and lymph nodal stage (pN+) (Fig. 2).
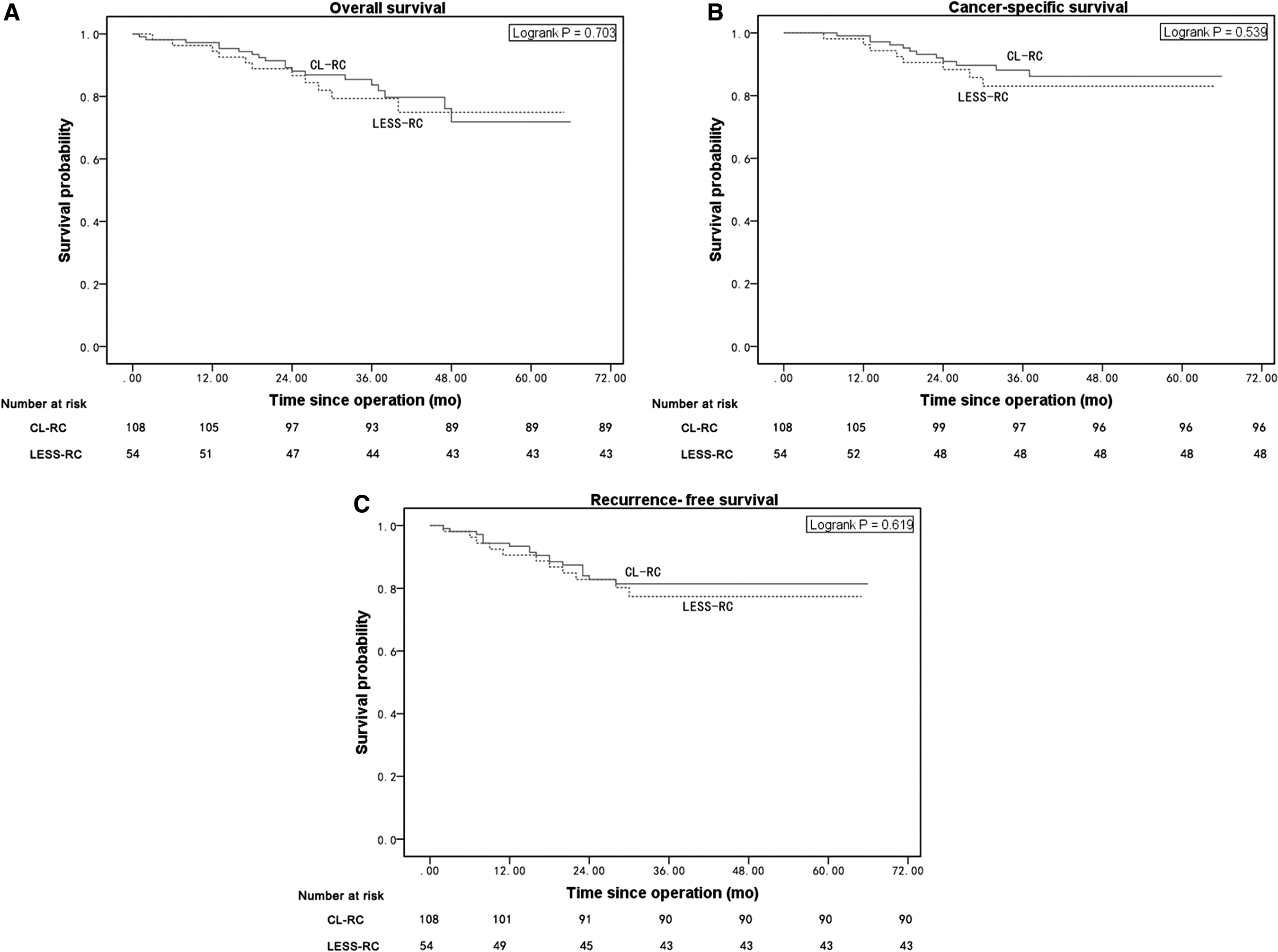
Kaplan-Meier curves for 24-month survival of LESS-RC vs CL-RC:
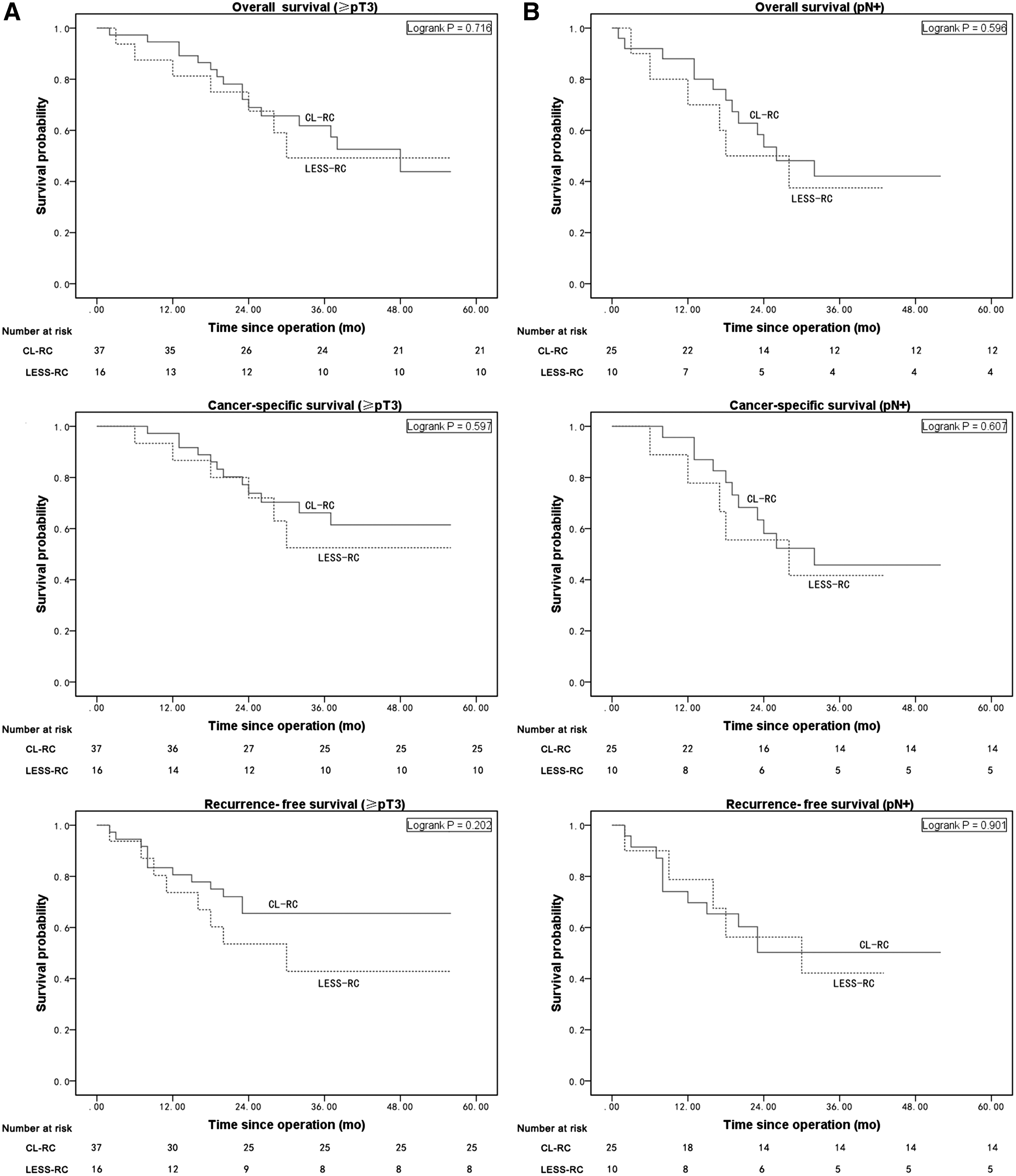
Kaplan-Meier curves for 24-month overall survival, cancer-specific survival, and recurrence-free survival of LESS-RC vs CL-RC: stratified for
The estimated 24-month OS for LESS-RC and CL-RC was 86.7% and 88.1%, respectively (log-rank test, p = 0.703); CSS was 88.3% and 90.9%, respectively (log-rank test, p = 0.539); and RFS was 80.2% and 87.5%, respectively (log-rank test, p = 0.619). When substratified by tumor stage (pT3 or higher) and lymph node stage (pN+), no significant differences in OS (log-rank test, p = 0.716 and p = 0.596, respectively), CSS (log-rank test, p = 0.597 and p = 0.607, respectively), and RFS (log-rank test, p = 0.202 and p = 0.901, respectively) at 24 months were observed in the two groups.
Multivariate Cox regression analysis showed that LESS-RC was not associated with worse OS (HR: 0.409 [95% CI: 0.162, 1.035]; p = 0.059), CCS (HR: 0.321 [95% CI: 0.103, 1.006]; p = 0.051), and RFS (HR: 0.618 [95% CI: 0.255, 1.501]; p = 0.288) after controlling for patient and tumor characteristics and intervention confounders (Table 6).
Discussion
LESS has evolved with the aims of minimizing bleeding and postoperative pain and expediting postoperative recovery, and this novel technique has been applied to a wide variety of urologic procedures. 15,16 According to the European Association of Urology (EAU) guidelines, LESS is considered feasible in selected patients with bladder cancer, but only as part of a properly designed clinical trial because of absence of mature data on its use. 11 To our knowledge, this study is the first to compare LESS-RC with CL-RC in the era of oncologic efficiency and safety outcomes.
Many previous studies showed that LESS-RC had less blood loss and decreased pain compared with conventional laparoscopy. 17,18 In this study, we found that LESS-RC had lower EBL and VAPS during the first 3 days after operation, although we did not observe any statistical differences in blood transfusion between groups. These findings might be explained by less tissue trauma with the LESS technique. In addition, LESS-RC had shorter times to ambulation and oral intake after operation than CL-RC, indicating that LESS-RC could achieve more rapid postoperative convalescence, although median EBL difference of approximate 60 mL and time to ambulation difference of a half day were not clinically “significant.”
Oncologic efficiency
Although our oncologic follow-up was not mature, the short-term results were encouraging, and we had several noteworthy findings. First, we identified that LESS-RC had short-term oncologic control similar to that of CL-RC for recurrence and survival outcomes, and that had a major impact on determining the oncologic efficiency of RC. The EAU guidelines have shown that most recurrences of BUC occurred in the first 24 months after operation, often between 6 and 18 months. 19 Furthermore, Tyritzis and colleagues demonstrated that the main oncologic end point was cancer recurrence or cancer-specific death at 24 months after RC. 20 Consequently, our median follow-up of 33.5 and 33 months for the LESS-RC and CL-RC groups were robust endpoints when evaluating and comparing the oncologic efficiency of these two techniques. The recurrence rates of the two groups were comparable to those reported in the literature. 4,20 On survival analysis, we found that the estimated 24-month OS, CSS, and RFS rates were not significantly different for LESS-RC and CL-RC and were consistent with previously published reports. 5,20 This finding led us to assume that LESS-RC would not be inferior to CL-RC as a short-term oncologic management strategy for patients with BUC, although long-term follow-up is needed.
Second, we confirmed that extended LND could be performed with the LESS technique and achieve an adequate lymph node yield during RC. This finding was in keeping with the report of Kaouk and colleagues. 7 Measures of surgical quality for RC include LND method and lymph node yield, both of which are surrogates for oncologic efficiency. In this study, 13% of LESS-RC patients received the extended LND, and the median number of lymph nodes removed did not differ significantly between the LESS-RC and CL-RC groups. The LESS technique seemed feasible in most patients and had a lymph node yield similar to the conventional laparoscopic approach. In addition, our LESS and CL-RC techniques adhered to the same oncologic standards and anatomic boundaries. That could be a very important factor related to the oncologic efficiency of these two techniques, and possibly be responsible for the similar findings for survival.
Third, we showed that LESS-RC was not associated with recurrence and worse survival after adjusting for confounders. In this context, selection criteria for LESS-RC might be broader, although the EAU guidelines suggest that LESS-RC is considered feasible only in carefully selected patients. 11
Complications
We had some important findings regarding complications. First, we confirmed that LESS-RC could achieve early and late complication rates similar to those of CL-RC. As expected, the first 30 days after RC were the most crucial, and active surveillance of patients during this period is strongly recommended. 21 Early (≤30 days) overall complication rates were 42.6% in the LESS-RC group and 32.4% in CL-RC group. Infectious and gastrointestinal complications were the most common complications for the two groups. These findings appeared compatible with results from the International Robotic Cystectomy Consortium, 22 the largest report of complications of robot-assisted RC (RARC) available to date. Moreover, we found late overall complication rates of 24.1% and 18.5% in the LESS-RC and CL-RC groups, respectively. Notably, no significant differences were found between groups for major complications and readmission rates during the early and late surveillance periods. These findings demonstrate that LESS-RC was a safe treatment alternative to CL-RC or other minimally invasive surgery.
Second, our findings confirmed similar rates of overall and major complications for LESS-RC and CL-RC, but a higher rate of minor complications at 90 days with LESS-RC. We reviewed the 90-day postoperative period, during which the overall complication rate was 59.3% for LESS-RC and 43.5% for CL-RC. These findings were in accordance with the acceptable range of the current largest ORC, LRC, and RARC series. 22 –26 Most complications were low grade when stratified by Clavien-Dindo classification. We previously reported a 31% 90-day overall complication rate in 210 consecutive RC patients at a single institution, 27 a rate lower than that in this study. The different results might be related to differences in study populations and surgical techniques. Again, no significant differences were found between groups for major complications and readmission rates during this surveillance period, although the 90-day minor complication rate for LESS-RC was higher than that for CL-RC.
Third, although we found no significant difference between LESS-RC and CL-RC for overall complications rates, multivariate analysis showed that LESS-RC was associated with 90-day overall complications. Some factors could result in this difference. From a statistical standpoint, the impact of LESS-RC on complication outcomes could be reflected more clearly after controlling for potential confounders, which could play important roles in differential outcomes and introduce interpretation biases in comparing LESS-RC and CL-RC. This could possibly result in significant association between LESS-RC with 90-day overall complications in multivariate analysis. From a clinical standpoint, this difference could be ascribed to higher rate of 90-day minor complications for LESS-RC that resulted in a higher overall complication rate for LESS-RC vs CL-RC (59.3% vs 43.5%), although it did not reach statistical significance. Nonetheless, we believe that LESS-RC is a safe alternative for patients with BUC because we found that LESS-RC was not associated with 90-day major complications. Major complications should play an important role in assessment of a new and innovative procedure's safety, whereas minor complications in most patients typically represent only a small clinical impact on the postoperative recovery course. 20
Limitations
This study had several limitations. First, although this was a case-matched control study, the retrospective and nonrandomized design could introduce some potential biases for patient selection and outcome analysis, which could result in low power to draw definitive conclusions. Second, the small sample size and short-term follow-up of this study might have limited the power for comparison of oncologic efficiency. Finally, the validated questionnaire for cosmesis was not implemented to compare benefits of LESS-RC and CL-RC.
Conclusions
This study demonstrates that LESS-RC and CL-RC have comparable safety and efficiency for patients with BUC. Compared to CL-RC, LESS-RC was with less postoperative pain, lower EBL, and more rapid convalescence, but was associated with 90-day overall complications.
Footnotes
Acknowledgment
This study was supported by grant 2017A030313499 from the Natural Science Foundation of Guangdong Province, People's Republic of China.
Author Disclosure Statement
All authors certify that all conflicts of interest, including specific financial interests and relationships, and affiliations relevant to the subject matter or materials discussed in the article (e.g., employment/affiliation, grants or funding, consultancies, honoraria, stock ownership or options, expert testimony, royalties, or patents filed, received, or pending), are the following: none.