
Abstract
Purpose:
To describe the technique of laparoscopic in situ dismembered pyeloplasty as a modified technique during which the alignment of ureter and renal pelvis remains intact during ureteropelvic junction (UPJ) anastomosis. We also assessed intraoperative and postoperative outcomes of this modification in comparison to standard laparoscopic dismembered pyeloplasty.
Patients and Methods:
Patients with significant primary UPJ obstruction without any history of abdominal surgery, high ureter insertion, or renal anomalies were considered. The patients were consecutively enrolled one after another into one of two study groups: classic laparoscopic dismembered pyeloplasty (Group I) or laparoscopic in situ dismembered pyeloplasty (Group II), however, those with aberrant vessels crossing the UPJ were allocated specifically to Group I because UPJ anastomosis should be done anterior to the aberrant vessels. Demographic data, intraoperative timings, and postoperative and follow-up outcomes were compared in the two groups.
Results:
Patients in Group I (n = 23) and Group II (n = 14) had similar demographic characteristics. Mean operative time was significantly longer in Group I (103.8 ± 19.95 minutes vs 89.5 ± 18.90 minutes, p = 0.038). Total duration of UPJ repair and anastomosis was also significantly longer in Group I (92.7 ± 15.82 minutes vs 78.4 ± 14.76 minutes, p = 0.021). The method of pyeloplasty significantly affected the time required to prepare ureter and renal pelvis (p = 0.017) and the duration of UPJ anastomosis (p = 0.014). Both were shorter in Group II. Mean follow-up period was 14.4 ± 7.42 months in Group I and 14.05 ± 7.93 months in Group II (p = 0.88). Success rate was 95.6% in Group I and 100% in Group II (p = 0.42).
Conclusion:
Laparoscopic in situ pyeloplasty is a safe and effective approach that can help simplify laparoscopic pyeloplasty, especially at teaching centers where surgeons with variable levels of experience perform laparoscopic procedures.
Introduction
S
In the present study, we describe the technique of laparoscopic in situ dismembered pyeloplasty. In this technique, alignment of the ureter and renal pelvis remains intact during ureteral spatulation and UPJ anastomosis, and the surgeon can remove the stenotic segment and reconfigure a dependent, funneled UPJ. We compared intraoperative and postoperative outcomes of this modification with a series of patients who underwent standard laparoscopic dismembered pyeloplasty.
Patients and Methods
Patients
Between June 2014 and March 2016, all patients with significant primary UPJ obstruction and with no history of abdominal surgery were considered for inclusion. The indications for LP were based on the patients' symptoms and preoperative imaging results, that is, ultrasonography (progressive hydronephrosis and increased anterior–posterior diameter [APD] of renal pelvis) and/or intravenous urography (hydronephrosis, parenchymal change, and delayed collecting system drainage) and/or Technetium-99m diethylene triamine pentaacetic acid (Tc-99m DTPA) diuretic renal scan (obstructive curve with delayed 50% drainage after 20 minutes and/or compromised renal function). Patients with high ureteral insertion and those with renal anomalies (e.g., horseshoe kidneys) were excluded.
The patients were consecutively enrolled one after another into one of two study groups: classic laparoscopic dismembered pyeloplasty (Group I) or laparoscopic in situ dismembered pyeloplasty (Group II), however, those with aberrant vessels crossing the UPJ were allocated specifically to Group I because UPJ anastomosis should be done anterior to the aberrant vessels.
All patients received a single dose of ceftriaxone before surgery, and all procedures were done by the same expert laparoscopic surgeon (A.A.).
Surgical techniques
Classic laparoscopic dismembered pyeloplasty (Group I)
Four-port transperitoneal laparoscopy was done with the patient in lateral decubitus position. After colon reflection, dissection, and mobilization of the proximal ureter, UPJ, and renal pelvis, classic dismembered pyeloplasty was done for patients in Group I. 7 Briefly, the UPJ was dismembered and the stenotic part was removed. In the presence of any aberrant vessels over the UPJ, the proximal ureter was repositioned anterior to these vessels. After spatulation of the lateral aspect of the ureter, the ureter was anastomosed to the renal pelvis over a Double-J stent with the Anderson–Hynes technique using 5-0 polyglactin sutures. The most dependent portion of the renal pelvis was first sutured to the distal end of the ureterotomy incision, and the posterior edges of the renal pelvis and the ureter were anastomosed from inside. After completion of the posterior layer, a Double-J stent was inserted and the anterior layer of anastomosis was completed. Then, the renal pelvis was closed, with trimming before closure if there was any redundancy (Fig. 1).

Schematic drawing of classic dismembered pyeloplasty. After the UPJ was dismembered
Laparoscopic in situ dismembered pyeloplasty (Group II)
After dissection and mobilization of the UPJ, a 1-cm longitudinal incision was made over the lateral aspect of the proximal ureter distal to the site of obstruction. Another 2-cm oblique incision was made on the lateral aspect of the renal pelvis at its most dependent portion to divide the posterior and anterior walls of the renal pelvis. The most dependent part of the incised renal pelvis was sutured to the distal end of the ureterotomy incision. Then, both anterior and posterior suture lines were completed cephalad over a Double-J stent. Once the dependent funnel-shaped anastomosis was completed, the ureter was divided above the site of anastomosis and the stenotic UPJ segment was removed. Again if required, pelvic trimming was done and the renal pelvis was then closed (Fig. 2).

Schematic (upper panels) and intraoperative views (lower panels) of laparoscopic in situ pyeloplasty. A 1-cm longitudinal incision was made over the lateral aspect of the proximal ureter distal to the site of obstruction. Another 2-cm oblique incision was made on the lateral aspect of the renal pelvis at its most dependent portion to divide the posterior and anterior walls of the renal pelvis
Study outcomes
Patients' demographic and preoperative characteristics were recorded. To accurately investigate how each pyeloplasty method affected the time of UPJ repair and anastomosis, this critical part of the operation was divided into three procedural milestones, and the time spent on each phase was recorded as follows: Phase 1: Ureter and pelvis preparation consisting of ureteral division (Group I), spatulation, renal pelvis incision (Group II), and preparation. Phase 2: UPJ anastomosis and stenting. Phase 3: Renal pelvis trimming (if applicable) and closure.
Postoperative complications and length of hospital stay were also documented. The patency of anastomosis was verified by evaluating the degree of hydronephrosis and APD with ultrasonography and Tc-99m-DTPA scans done every 3 months for the first year and then once yearly. Success was defined as the absence of symptoms, negative urine culture, improvements in hydronephrosis severity, APD, and drainage patterns in renal scans. Demographic data, intraoperative timings, postoperative complications, and follow-up outcomes were compared in the two groups.
Statistical analyses
All statistical analyses were done with SPSS v.17 (SPSS, Inc., Chicago, IL). We used Student's t-test to compare continuous variables and the chi-squared test for categorical variables.
Results
During the study period, a total of 37 patients (17 men, 46%) were enrolled in Group I (classic laparoscopic dismembered pyeloplasty, n = 23) or Group II (laparoscopic in situ dismembered pyeloplasty, n = 14). The patients' preoperative demographic characteristics were similar in both groups (Table 1). In eight patients (21.6%), crossing vessels were observed during laparoscopic dissection of the UPJ; and all were included in Group I. Three patients in each group had malrotated kidneys. The redundant pelvis was trimmed in 10 of 37 patients (6 [26%] in Group I vs 4 [28.5%] in Group II).
SD = standard deviation.
Mean operative time was significantly longer for classic LP (Group I) (103.8 ± 19.95 minutes vs 89.5 ± 18.90 minutes, p = 0.038, 95% confidence interval [CI] = 0.85, 27.8). Mean operative time for eight cases with aberrant vessels was 105.6 ± 20.4 minutes. Total time needed for UPJ repair and anastomosis was also significantly longer in Group I (Phases 1 + 2 + 3, 92.7 ± 15.82 minutes vs 78.4 ± 14.76 minutes, p = 0.021, 95% CI = 2.44, 28.32). Figure 3 shows the time needed for each phase of UPJ repair and anastomosis. Interestingly, the pyeloplasty method significantly influenced the time required for Phase 1 (preparation of the ureter and renal pelvis) (p = 0.017, 95% CI = 1.15, 11.15) and Phase 2 (UPJ anastomosis) (p = 0.014, 95% CI = 1.83, 15.01). Both were shorter in Group II (laparoscopic in situ dismembered pyeloplasty). There were no intraoperative complications or conversions to open surgery in either group.
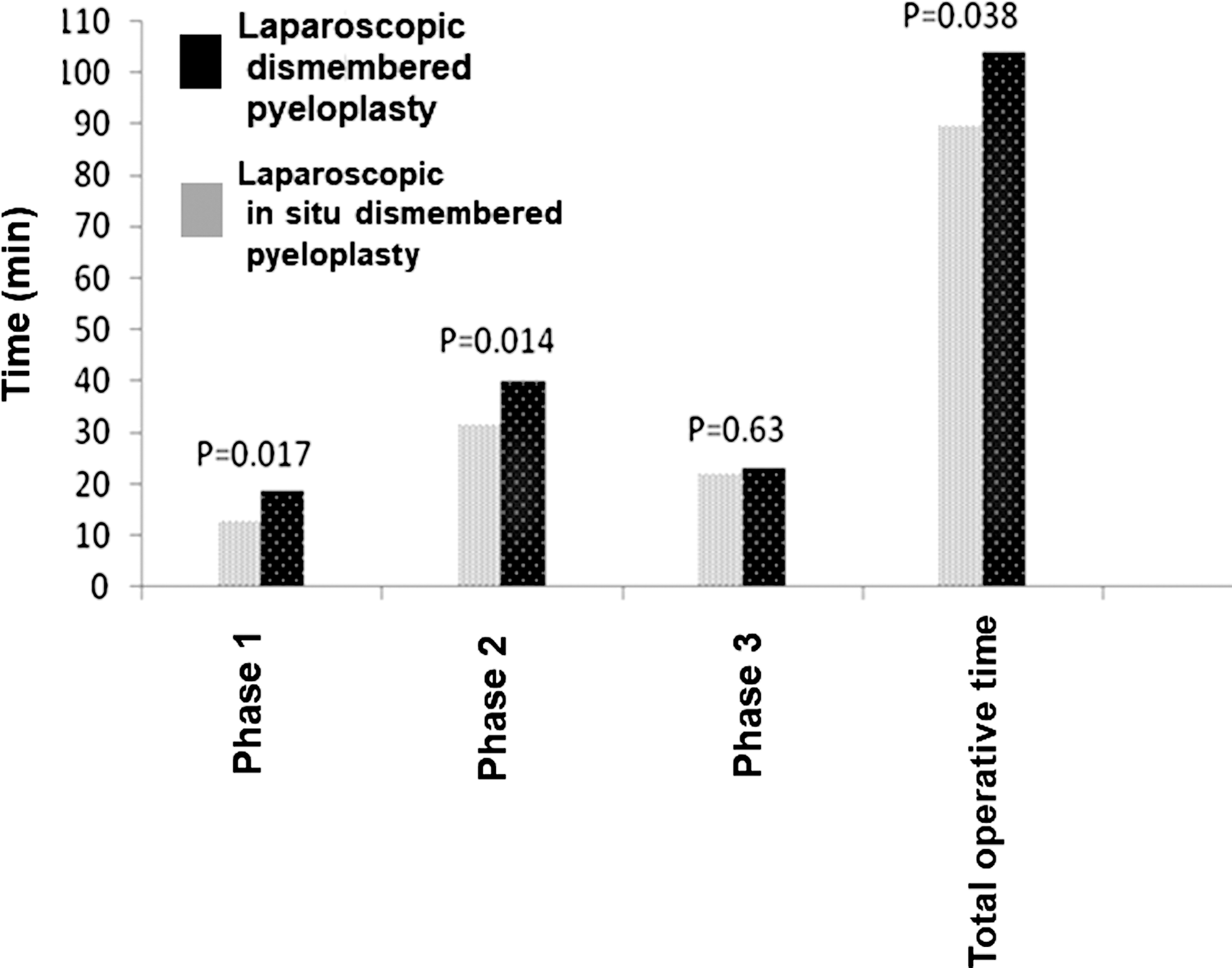
Total operative time and the timing of each phase of UPJ repair and anastomosis during classic laparoscopic dismembered pyeloplasty vs in situ dismembered laparoscopic pyeloplasty. Phase 1: Preparation of the ureter and renal pelvis; Phase 2: UPJ anastomosis; Phase 3: Renal pelvis trimming (if needed) and closure.
One patient in Group I had continuous bloody discharge from the Penrose drain site a few hours after surgery. Laparoscopic exploration revealed blood oozing from the tiny vessels around the renal pelvis, which was controlled.
The Double-J stent was removed 4 weeks after surgery. Mean follow-up period was 14.4 ± 7.42 months in Group I and 14.05 ± 7.93 months in Group II (p = 0.88). The success rate was 95.6% in Group I and 100% in Group II (p = 0.42). One patient in the classic LP group developed recurrent flank pain 6 months after the Double-J stent was removed, with no resolution of hydronephrosis in imaging studies. A fibrotic band at the site of anastomosis was found during ureteroscopy, and was managed by retrograde endopyelotomy and stenting.
Discussion
In the era of minimally invasive surgery, LP has been considered a standard technique for patients with UPJ obstruction. This widespread acceptance is a result of the minimal postoperative morbidity along with reliable and durable outcomes in comparison to open pyeloplasty. 2 –4 Both open and LP are technically challenging procedures. LP requires extensive experience with intracorporeal suturing and knot-tying techniques. Moreover, care must be taken during all steps of repair and anastomosis to ensure correct alignment of the ureter and renal pelvis, and the directions of the suture lines. Nondismembered LP techniques, in which alignment of the ureter and renal pelvis remains intact during anastomosis, are generally less challenging, but according to some studies, their success rates were lower than classic dismembered LP. Casale and colleagues compared the outcome of dismembered vs nondismembered LP in 26 pediatric patients. Operative time was significantly shorter with the nondismembered technique, whereas the success rate was higher with dismembered LP (94% vs 43%; p = 0.002). 5 Szydełko and colleagues retrospectively compared these two methods and again reported a longer operative time for dismembered LP but similar success rates (91.8% vs 91.2%). Further work by this group prospectively compared the outcome of laparoscopic dismembered pyeloplasty vs laparoscopic Y-V pyeloplasty. They reported similar operative times, but the success rate was higher with the dismembered method (95% vs 86%). 6,8
Several modifications of LP techniques have been proposed to prevent ureteral twisting during spatulation and anastomosis, avoid UPJ misalignment, and simplify the anastomosis. Neulander and colleagues transected the UPJ with an ellipsoid portion of the renal pelvis. The pelvic flap was helpful in correcting ureteral spatulation and obviated the need for stay suture placement. 9 Ou and colleagues studied their modified technique for laparoscopic dismembered pyeloplasty in 46 patients. In their technique, the anterior aspect of the renal pelvis was dismembered from the ureter, and the posterior aspect of the ureter was spatulated. They believed that this configuration made suturing easier, given that the two suture lines were on the right and left sides of a single laparoscopic plane. 10 Their mean operative time was 108 minutes, with a success rate of 97.8%. 10 Ahlawat and colleagues showed the feasibility of the “postanastomotic dismemberment” technique, which is based on principles similar to our technical modification: the ureter is attached to the renal pelvis during all steps of spatulation, stenting, and anastomosis. Their success rate was 95.1% and their operative time was much shorter (97.3 minutes) than previous series. 11 Recently, Yang and colleagues reported their experience with this approach in 28 patients. They obtained promising outcomes, with mean operative and suturing times of 137.3 and 37.3 minutes, respectively, and a success rate of 96.1%. 12
We designed this prospective study to carefully evaluate laparoscopic in situ dismembered pyeloplasty; to our knowledge, this is the first attempt to compare the outcomes of classic vs in situ laparoscopic techniques for this operation. To obtain accurate, detailed evidence on the duration of UPJ repair and anastomosis, we specifically focused on the timing of each phase. We found that in comparison to the classic laparoscopic technique, in situ dismembered pyeloplasty reduced total operative time by 13.8% and the total time of UPJ repair and anastomosis by 15.4%. Understandably, these improvements originated mainly from the first and second phases of UPJ repair (Fig. 3). When the alignment of UPJ is preserved, the process of spatulation and anastomosis would be easier without the risk of UPJ twisting (Fig. 2). The surgeon can easily identify and incise the lateral border of the ureter and the dependent part of the renal pelvis. Moreover, in laparoscopic in situ dismembered pyeloplasty, throughout UPJ preparation and anastomosis (Phases 1 and 2), the ureter and renal pelvis are still kept attached, and therefore, they remain close to each other and anastomosis can proceed without any tension. Furthermore, the reduction in operative time (and in procedure difficulty) did not compromise the success rate or postoperative outcomes.
All procedures in this trial were carried out by the same experienced laparoscopic surgeon (A.A.). Therefore, one may postulate that the differences in procedural timings might have been more prominent if a less experienced surgeon had been involved.
In conclusion, laparoscopic in situ pyeloplasty is a safe and effective approach that can help simplify LP, especially at teaching centers where surgeons with variable levels of experience perform this procedure.
Footnotes
Acknowledgments
The present article is based on the thesis by Dr. Afshin Molaie for the specialty degree in Urology awarded by Shiraz University of Medical Sciences (No. 95-01-01-12322). The work was supported by Shiraz University of Medical Sciences, Shiraz, Iran. We thank K. Shashok (AuthorAID in the Eastern Mediterranean) for improving the English language usage in this article and Dr. Mehdi Edalati for drawing the schematic figures.
Author Disclosure Statement
No competing financial interests exist.