
Abstract
Introduction:
Removal of embolization coils eroded into the renal collecting system poses a risk of hemorrhage, which may need to be addressed with arteriography and embolization at the time of treatment. The purpose of this report is to describe a novel approach, by which prone percutaneous nephroscopic coil retrieval is coupled with simultaneous prone transradial renal arterial access to mitigate this potential complication.
Methods:
A retrospective chart review of the electronic medical record systems was performed from January 2008 to May 2017 to identify patients who had undergone percutaneous removal of embolization coils eroded into the renal collecting system. Patients who had migration of embolization coils into the renal collecting system who were symptomatic with pain, hydronephrosis, or infection were considered for inclusion. Patients who had coil migration, but were asymptomatic were not offered removal. Patient demographics and case characteristics were examined as were operative outcomes.
Results:
A total of three patients fulfilled the study criteria. Migrated embolization coils were able to be effectively removed in all patients. Of the patients, two underwent simultaneous prone transradial renal arteriography with placement of an occlusion balloon catheter into the segmental artery of interest. In one patient, significant arterial bleeding was encountered after coil removal, which was effectively addressed with simultaneous arteriography and glue embolization.
Conclusion:
Erosion of embolization coils into the renal collecting system, while rare, may be a significant long-term complication of coil embolization. Combining nephroscopy with prone transradial arteriography in preparation for procedure-associated hemorrhage may make removal of migrated coils safer.
Introduction
C
Although scattered reports are available in the literature, there is little consensus on standardized, safe management of coil erosion sequelae. Furthermore, the risk of hemorrhage posed by removal of the embolization coils has yet to be addressed. One potential challenge in managing potential arterial hemorrhage following coil removal is patient positioning. In particular, percutaneous retrieval is typically performed in the prone position, while renal arteriography is typically performed with the patient in the supine position via femoral arterial puncture. Delays in repositioning during an active arterial hemorrhage may result in deleterious patient outcomes.
The purpose of this report is to describe performing simultaneous prone transradial renal arteriography in anticipation of possible treatment of hemorrhage at the time of percutaneous nephroscopy-guided removal of embolization coils with erosion into the renal collecting system.
Materials and Methods
Patient selection
This study was conducted with institutional review board approval and complied with the Health Insurance Portability and Accountability Act. Informed consent was obtained from all patients. Patients were identified via retrospective review of the electronic medical record (EPIC; Epic Systems Corporation, Verona, WI) and (CareWeb, International Business Machine Corporation [IBM], Armonk, NY) in conjunction with the department's prospectively maintained database (EMERSE v3.1). The search terms “prone,” “transradial access,” “migration of renal embolization coil,” “erosion of renal embolization coil,” “renal embolization,” “coil retrieval,” “nephroscopy,” “interventional radiology,” “urology,” “renal angiography,” and “prone angiogram” were used to identify patients. Three patients matched the inclusion criteria. One of these patients has been previously described. 7
Inclusion/exclusion criteria
Patients with renal arterial embolization with coils and subsequent migration of the coils into the renal collecting system with symptoms (hydronephrosis, pain, or recurrent infection) were included. Patients who had migration of coils, but were asymptomatic were excluded. Included patients are shown in Table 1.
Procedure details
Prone transradial access and renal arteriography
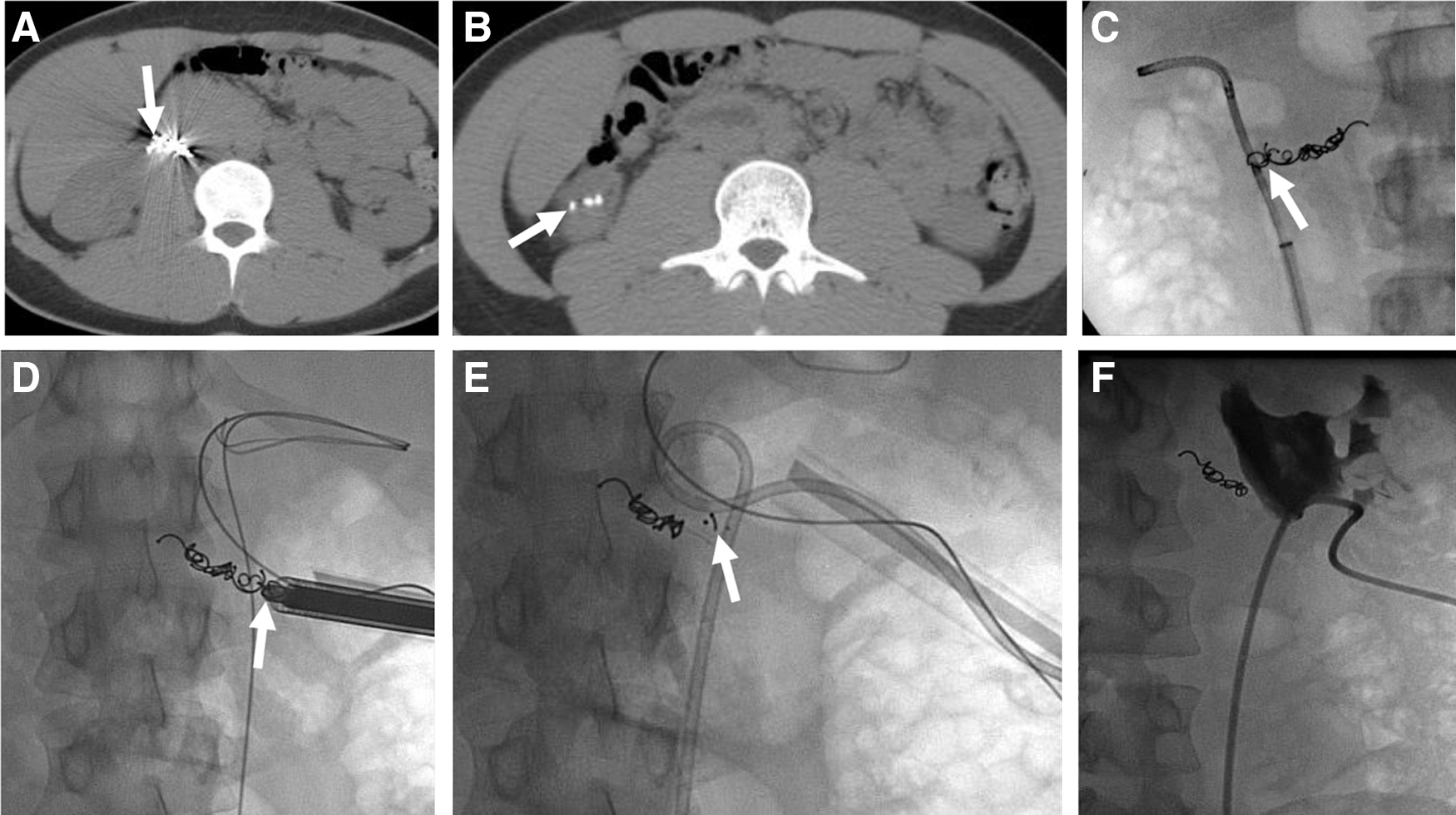
All procedures were performed under general anesthesia. The patient was placed prone on the angiographic table with the left arm extended. Half an inch of nitropaste was placed on the left forearm one-half hour before intervention. A Barbeau test was performed before access with a type IV Barbeau test considered a contraindication to use of the radial artery for access. The left forearm, hand and flank were prepped and draped in a sterile manner. The radial artery was accessed under ultrasound guidance, using the Terumo Radial Access Kit (Terumo Medical Corporation, Somerset, NJ) and a 5F sheath placed (Fig. 1A). Two hundred micrograms of nitroglycerin, 2.5 mg of verapamil, and 3000 units of heparin were then infused through the sheath. A 100 cm 5F MPC guide catheter (Codman Neurovascular, Raynham, MA) was placed into the renal artery. Renal arteriography was performed in two projections. A 4-mm diameter by 11-mm length Scepter XC balloon (MicroVention, Tustin, CA) was advanced over a 0.014" Synchro wire (Stryker Neurovascular, Fremont, CA) into the segmental artery involved. Selective arteriography was performed through the microcatheter to confirm appropriate positioning of the catheter. The balloon was inflated during the percutaneous removal of embolization coils to prevent possible bleeding. Once the coils were removed, repeat arteriography was performed to identify any vessel injury. If vessel injury was identified, the artery was occluded with n-butyl cyanoacrylate (n-BCA) (Codman Neurovascular). The catheters were removed, and hemostasis was obtained with manual compression using the radial arm band (Terumo Medical Corporation).

Percutaneous nephroscopy and embolization coil retrieval
Retrograde ureteral access was obtained in two patients with the aid of flexible cystoscopy. A catheter was placed into the proximal renal collecting system and contrast was injected to provide opacification of the collecting system. Fluoroscopic-guided access into an appropriate renal calyx was performed in two patients and ultrasound-guided access in one patient. In two patients the tract was then dilated using a 24F Bard® X-Force Dilatation Balloon, and then the plastic sheath was placed. In one patient the 30F Bard X-Force system was utilized. A 22.5F rigid endoscope (Olympus Medical, Center Valley, PA) was then used to perform nephroscopy with removal of the coils performed with 3 mm rigid grasping forceps (Fig. 1B).
Outcomes
Outcomes are shown in Table 1. Prone transradial technical success was defined as effective cannulation of the radial artery. Renal arteriography technical success was defined as effective renal artery arteriography. Percutaneous renal access technical success was defined as percutaneous access into the kidney with placement for the nephroscope. Embolization coil removal technical success was defined as removal of all migrated embolization coils by fluoroscopy. Clinical success was defined as resolution of presenting systems.
Statistics
Calculations of percentages, means, and ranges were performed on the data using spreadsheet software (Excel 2017; Microsoft Corporation, Redmond, WA).
Results
Patients
Patient 1
A 21-year-old man presented with right flank pain and nephrolithiasis (Table 1 and Fig. 2). The patient previously had a ureteropelvic junction obstruction, which was treated with Acucise incision. This was complicated by pseudoaneurysm formation, which was treated with renal embolization with coils. Fifteen months after the embolization, the patient complained of flank pain and underwent ureteroscopy revealing a large stone burden overlying the embolization coils, which had eroded through the renal pelvis. Due to the inability to adequately access the calcifications and embolization coils via a retrograde approach, the patient underwent subsequent percutaneous coil removal. Access was obtained in a lower pole calyx, and a rigid grasper was used to manually extract visible embolization coils. This case was conducted before widespread use of a prone transradial renal arteriography approach, thus simultaneous arterial access was not performed. At conclusion of the stone removal, an 8F nephroureteral catheter was placed and remained for 48 hours. The patient had resolution of his pain, but did develop a symptomatic, right lower pole caliceal stone 12 months later, which was effectively treated ureteroscopically. At 4-year clinical follow-up the patient was doing well without flank pain.
Patient 1. Twenty-one-year-old male with left flank pain.
Patient 2
A 65-year-old man presented with chronic left flank pain, hydronephrosis, and recurrent infections 56 months after coil embolization of a traumatic left lower pole segmental renal artery pseudoaneurysm (Table 1 and Fig. 3). Contrast-enhanced CT of the abdomen and pelvis showed erosion of the embolization coils from the left lower pole renal artery into the left lower pole renal infundibulum and proximal left ureter along with moderate hydronephrosis and periureteral inflammatory changes. Ureteroscopy demonstrated urothelial overgrowth, and the coils could not be removed from this approach. Due to concerns for acute bleeding during coil removal, a decision was made to perform simultaneous prone transradial access renal angiography and possible embolization with percutaneous embolization coil removal.
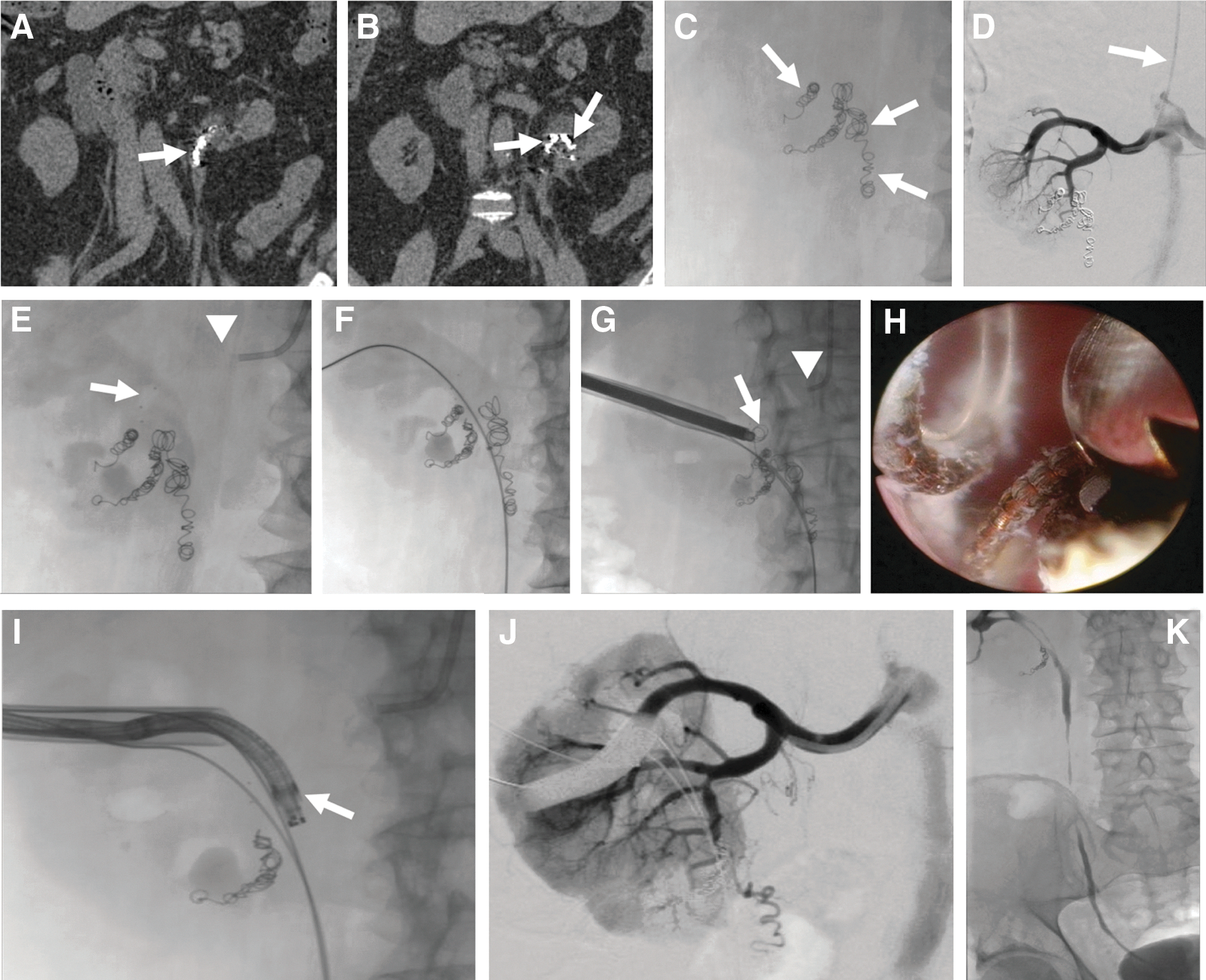
Patient 2. Sixty-five-year-old male with chronic left flank pain, hydronephrosis, and recurrent infections.
Details of prone transradial renal arteriography and percutaneous coil removal are described in the methods. In brief, from a prone transradial approach, an occlusion balloon was positioned within the segmental renal artery and the eroded embolization coils were removed in their entirety without any significant bleeding via a lower pole caliceal access. Some embolization coils were preserved within the lower pole segmental arterial branch thus maintaining hemostasis. A 10.2F × 28 cm nephroureteral stent was placed and subsequently removed 2 weeks following the procedure after a nephrostogram was performed showing no hydronephrosis. At 5 weeks, the patient reported resolution of left flank pain. Ultrasound showed resolution of the hydronephrosis. The patient remained asymptomatic at 14 weeks clinical follow-up.
Patient 3
A 54-year-old woman presented with right-sided flank pain (Table 1 and Fig. 4). One hundred and six months before presentation the patient had underwent embolization of a right lower pole segmental artery with coils for pseudoaneurysm due to complications from a nephrostomy tube placement. Ureteroscopy revealed erosion of several embolization coils through the anterior wall of the renal pelvis. Due to the extensive coil burden and inability to remove them satisfactorily via a retrograde approach, a percutaneous approach was undertaken with concurrent prone transradial renal arteriography with embolization in the event of significant bleeding.
Details of prone transradial renal arteriography with embolization and percutaneous coil removal are described in the methods. In brief, after obtaining lower pole caliceal access, the coils were identified in the renal pelvis. They were removed with rigid grasping forceps. The width and depth of coil erosion was extensive. Midway through coil removal, significant arterial bleeding was encountered. The occlusion balloon in the immediately adjacent segmental artery was inflated and visualization improved. The remainder of the coils were removed. Repeat segmental renal arteriography demonstrated persistent arterial bleeding with retroperitoneal extravasation. Large particle embolization with 900 to 1200 μm particles could have been considered, but only 700 to 900 μm particles were available. Due to the authors' extensive experience with glue embolization, n-BCA embolization of the bleeding vessel was performed with follow-up arteriogram demonstrating no further bleeding. Care was taken to make sure no glue entered the arterial defect. Repeat nephroscopy demonstrated no glue within the collecting system. A 10.2F × 24 cm nephroureteral stent was placed at the conclusion of the procedure. The patient underwent antegrade nephrostogram 6 weeks after coil removal, demonstrating a widely patent collecting system and the tube was removed. The patient remained symptom free with stable hemoglobin 10 weeks after the procedure.
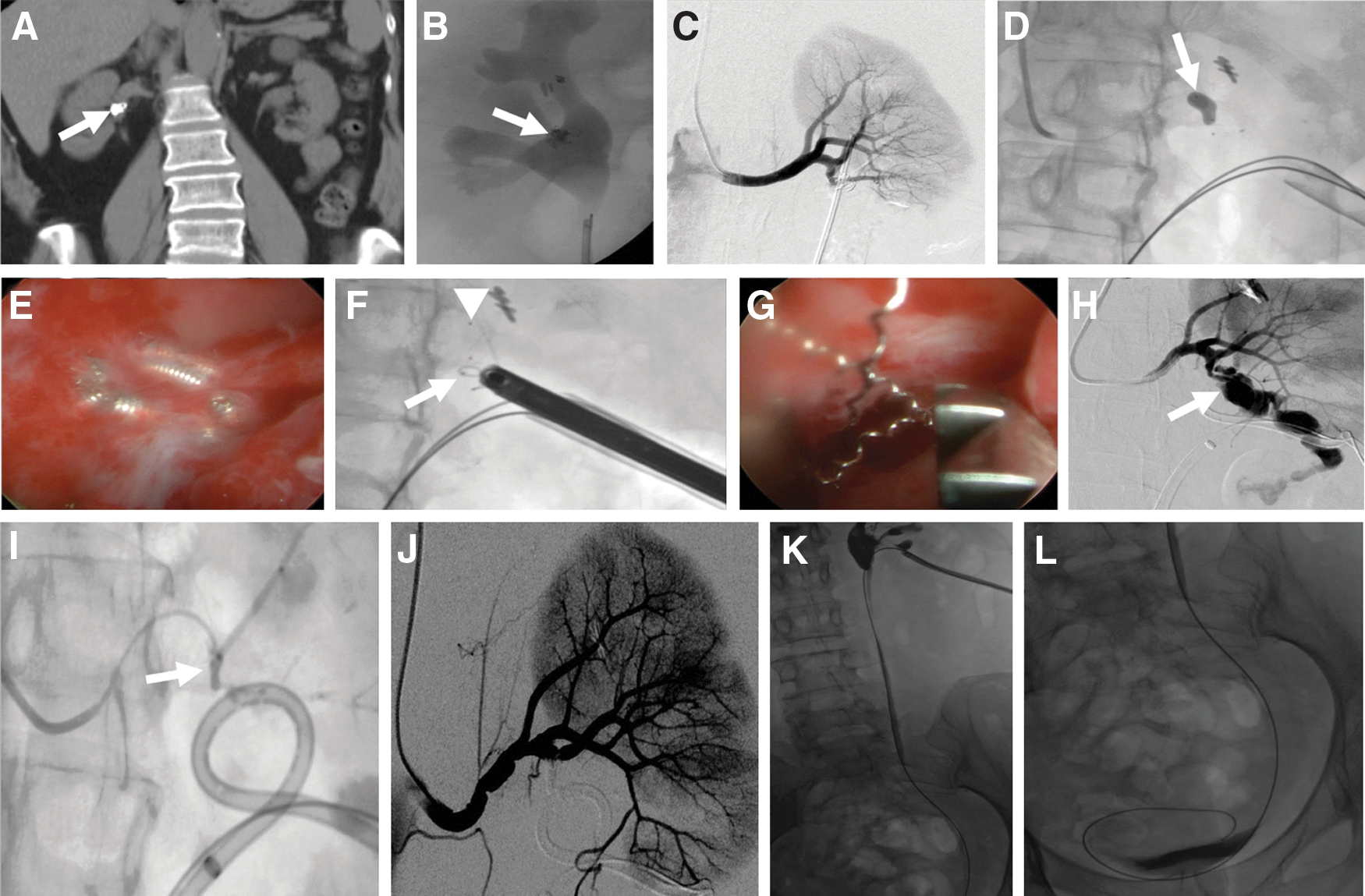
Patient 3. Fifty-four-year-old female with right flank pain.
Outcomes
Outcomes are shown in Table 1. Patients presented with coil erosion into the renal collecting system between 15 and 106 months (mean 59 months) after renal artery coil embolization. Of the three patients, two underwent prone transradial access, one of whom had intraprocedural bleeding requiring occlusion balloon inflation and subsequent glue embolization. The other patient who underwent prone transradial access had effective arteriography after coil extraction demonstrating hemostasis. The remaining patient did not undergo prone transradial access and had no evidence of bleeding. All three patients had effective complete extraction of eroded embolization coils with complete resolution of clinical symptoms and no recurrence of bleeding between 10 and 208 weeks (mean 77 weeks) follow-up. Postoperatively, patients 2 and 3 had nephroureteral stents in place for 2 and 6 weeks, respectively. Patient 2 lived a long distance away from the hospital and was unable to come in for tube removal sooner. Patient 3 had their tube left in place for a longer period of time due to the presence of life-threatening hemorrhage intraprocedurally. Double-J stents may have been an alternative option.
Discussion
This series describes a spectrum of three patients with erosion of embolization coils into the renal collecting system. The embolization coils were removed from a percutaneous access with nephroscopy. Ureteroscopy was performed in all three patients; however, ureteroscopic coil removal was not effective due to urothelial overgrowth. In two patients, prone transradial access with arteriography was performed due to potential risk for massive hemorrhage. In one patient, acute arterial bleeding was encountered and was able to be rapidly temporized to allow completion of coil retrieval and ultimately stopped permanently at the conclusion of the case (Fig. 1). The benefit of this technique is that it does not require repositioning of the patient to perform arteriography and embolization. Furthermore, it allows the positioning of a precautionary occlusion balloon in the artery before coil extraction in the event that life-threatening bleeding should occur (Fig. 1B). Radial access is beneficial because the forearm may be rotated at the elbow and accessed even with the patient in the prone position. 3
Owing to the relative rarity of embolization coil erosion into the urinary collecting system, there is limited data on the topic. While the incidence of coil erosion remains unclear, it has been described in the urologic literature. In a 2002 report, Rutchik et al. reported a case of stone formation on an eroded embolization coil in a 36-year-old female presenting with flank pain and microhematuria. 8 The stones were able to be removed via a retrograde approach and the embolization coil was extracted using a grasper. Poyet et al. 9 described a similar case in which a large stone formed on an eroded embolization coil placed after massive bleeding following open pyelolithotomy. In this instance, retrograde stone removal and coil retrieval were also accomplished. Unlike the previous two reports, Kumar et al. 10 described a percutaneous approach to coil and stone removal in the setting of a 2.7 cm renal pelvic stone growing attached to an eroded coil. Patients with eroded coils still partially embedded within the urothelium may be at higher risk for complications, such as hemorrhage. It's for these more complex presentations that percutaneous coil extraction with nephroscopy and prone transradial arteriography likely hold the most promise.
Fortunately, acute hemorrhage at the time of percutaneous nephrolithotomy requiring arteriography and embolization is rare, with an incidence of 0.3% to 0.8%. Although none of the aforementioned reports indicate that bleeding was encountered, the possibility for massive hemorrhage intuitively exists if coils are disrupted that are actively tamponading adjacent renal vasculature. 11,12 Should this occur during prone stone removal, rapid access for arteriography and embolization typically requires repositioning the patient supine for access to the femoral artery, thus effectively terminating the percutaneous procedure. To circumvent this issue related to positioning, transradial access may be used. First described in 1989 for coronary artery catheterization, 13 this technique has been widely implemented and studied in the interventional cardiology and interventional radiology literature. It has been shown to be both safe and effective for a range of interventional procedures, including coronary artery catheterization and vascular and visceral angiography. 14,15 In addition, access-related complications via a transradial approach are lower than a traditional femoral arterial puncture. 16 Prone transradial access and arteriography have also been described to perform simultaneous tumor ablation and transarterial embolization. 3 Rassweiler et al. have also previously described the use of transarterial embolization to effectively manage hematuria associated with renal malignancies. 17
This series suggests that prone transradial access may have a role in selected cases, namely complex percutaneous renal surgery where acute bleeding is expected. Certainly, in the rare event when a surgeon is removing embolization coils with erosion into the renal collecting system, this report showed that significant bleeding may occur in up to 33% of patients. In addition, this approach should be considered in situations where acute bleeding is either encountered during or shortly after percutaneous intervention as an alternative to repositioning with femoral arterial access, assuming institutional expertise is available. This allows the urologist to monitor bleeding in real time either by directly visualizing cessation of hemorrhage endoscopically or monitoring rate of bleeding from a nephrostomy tube. This approach involving the collaborative and simultaneous involvement of both interventional radiology and urology may make these challenging cases safer.
While this study offers a promising new technique to control hemorrhage at the time of complex percutaneous renal intervention, the findings must be viewed in the context of several limitations. First, this is a retrospective study and the sample size was small, evaluating only three patients at a single institution. Of the three patients, only two cases utilized prone transradial access, and of these two, only one patient experienced arterial bleeding requiring balloon occlusion and subsequent glue embolization of the segmental renal artery. However, the incidence of embolization coil erosion into the collecting system is rare, thus accumulating more patients would almost certainly need to occur in the context of multicenter study. In addition, the length of follow-up is limited, thus some of the patients may present later with bleeding complications. Furthermore, a physician with experience performing radial artery access and with access to the associated catheters required for transarterial interventions is necessary; therefore, this approach may not be generalizable to all physicians performing percutaneous renal interventions. Another benefit of the prone transradial technique is occlusion balloon inflation within the segmental renal artery can minimize bleeding and improve visualization should bleeding occur during prone nephroscopic removal. Transfemoral arterial access may also be performed if removal can be achieved from a supine percutaneous or ureteroscopic approach; however, requires patient repositioning if nephroscopy is performed from a prone percutaneous approach.
Conclusions
Erosion of embolization coils into the renal collecting system, while rare, may be a long-term complication of renal artery coil embolization. Prone transradial renal arteriography with placement of an occlusion balloon may minimize hemorrhagic risk during percutaneous nephroscopy-guided removal of eroded embolization coils. Additional studies are warranted.
Footnotes
Author Disclosure Statement
No competing financial interests exist.