
Abstract
Purpose:
The study sought to compare the procedural and clinical results of super-mini-percutaneous nephrolithotomy (SMP) with the use of first- and new-generation devices.
Methods:
A prospective, comparative cohort study was carried out between February 2013 and January 2017. Patients who underwent either first- or new-generation SMP were eligible for the study. Inclusion criteria were adult patients with renal stone <4 cm, or in pediatric patients with renal stone <2.5 cm with a history of failed extracorporeal shockwave lithotripsy. The primary outcome of the present study was the operating time, which was calculated from the starting of percutaneous puncture to the wound closure. Secondary outcomes were the stone-free rate (SFR), blood loss (hemoglobin decrease), hospital stay, and postoperative complications.
Results:
One hundred fifty-six consecutive patients who underwent SMP for treatment of renal stones were eligible for the study, with the first 85 patients undergoing SMP with the first-generation device, and the remaining 71 consecutive patients being treated with the new-generation SMP system. The two groups of patients had comparable demographic data, including age, BMI, stone size, Guy's score, stone location, comorbidities, grade of hydronephrosis, and history of urinary tract infection. The new-generation SMP had a shorter operation time (39.3 vs 50.5 min, p = 0.016) and shorter postoperative hospitalization time (2.1 vs 3.0 days, p < 0.001) than the first-generation SMP. No significant difference existed between the two groups for SFR, hemoglobin decrease, and tubeless rate. The overall operative complication rates using the Clavien-Dindo grading system were similar between the two cohorts of patients.
Conclusion:
The clinical outcomes of the new-generation SMP in patients with moderate-sized renal stone were comparable when compared with the first-generation SMP. New-generation SMP system using an irrigation/suction sheath improved intraoperative irrigation, a more efficient hydrodynamic mechanism for retrieval of fragments. This may account for the shorter operative time than the first-generation SMP system demonstrated in this study.
Introduction
P
SMP is a recent addition to the options for miniaturized PCNL, using an access sheath size of 10F to 14F. The first-generation SMP system was first introduced in 2012. 7 Despite obvious advantages such as reduced invasiveness and shorter hospitalization but equivalent SFR in correctly selected patients, the problem of restricted irrigation via a miniature nephroscope still exists. The operation is therefore associated with, at times, suboptimal visualization and longer operative time. To overcome these deficiencies, we adopted a new-generation SMP system with a newly designed irrigation/suction sheath to improve intraoperative irrigation and stone extraction. We have previously reported the SMP technique using the new-generation SMP system, 9 which appeared safe and feasible. In the present study, we sought to compare the procedural and clinical results of SMP with the use of the first- and new-generation devices.
Methods
A prospective, comparative cohort study on patients who underwent SMP for treatment of renal stones was conducted between February 2013 and January 2017 at a single tertiary unit by a single surgeon who, with an experience of more than 5000 cases of mini-PCNL, carried out all procedures. Consecutive patients who underwent both first-generation and new-generation SMP were included in the study. The inclusion criteria for the study were (1) adult patients with stone <4 cm, with or without previously failed extracorporeal shockwave lithotripsy (SWL) or retrograde intrarenal surgery and (2) pediatric patients with stone <2.5 cm with a history of failed SWL. The study protocol was reviewed and approved by the institutional review board. Informed consents were signed by all enrolled patients or patients' parents.
Devices
The first-generation SMP system consists of a 7F miniaturized nephroscope and a modified 10F to 14F plastic sheath with a suction/evacuation function. The nephroscope has a 3.3F working and irrigation channel that can accommodate a 0.8-mm pneumatic lithotripter probe, a laser fiber up to 365 μm, a 2.5F stone basket, or forceps. The modified access sheath consists of a straight sheath and a bifurcated proximal segment. The bifurcated proximal segment comprised a straight and an oblique tube at 45°. Both the straight sheath and the proximal tubes all have the same luminal diameter. The oblique tube can connect to a negative pressure aspirator for vacuum suction. There is a venting slit along the longitudinal axis of the oblique tube for regulating pressure (Fig. 1).
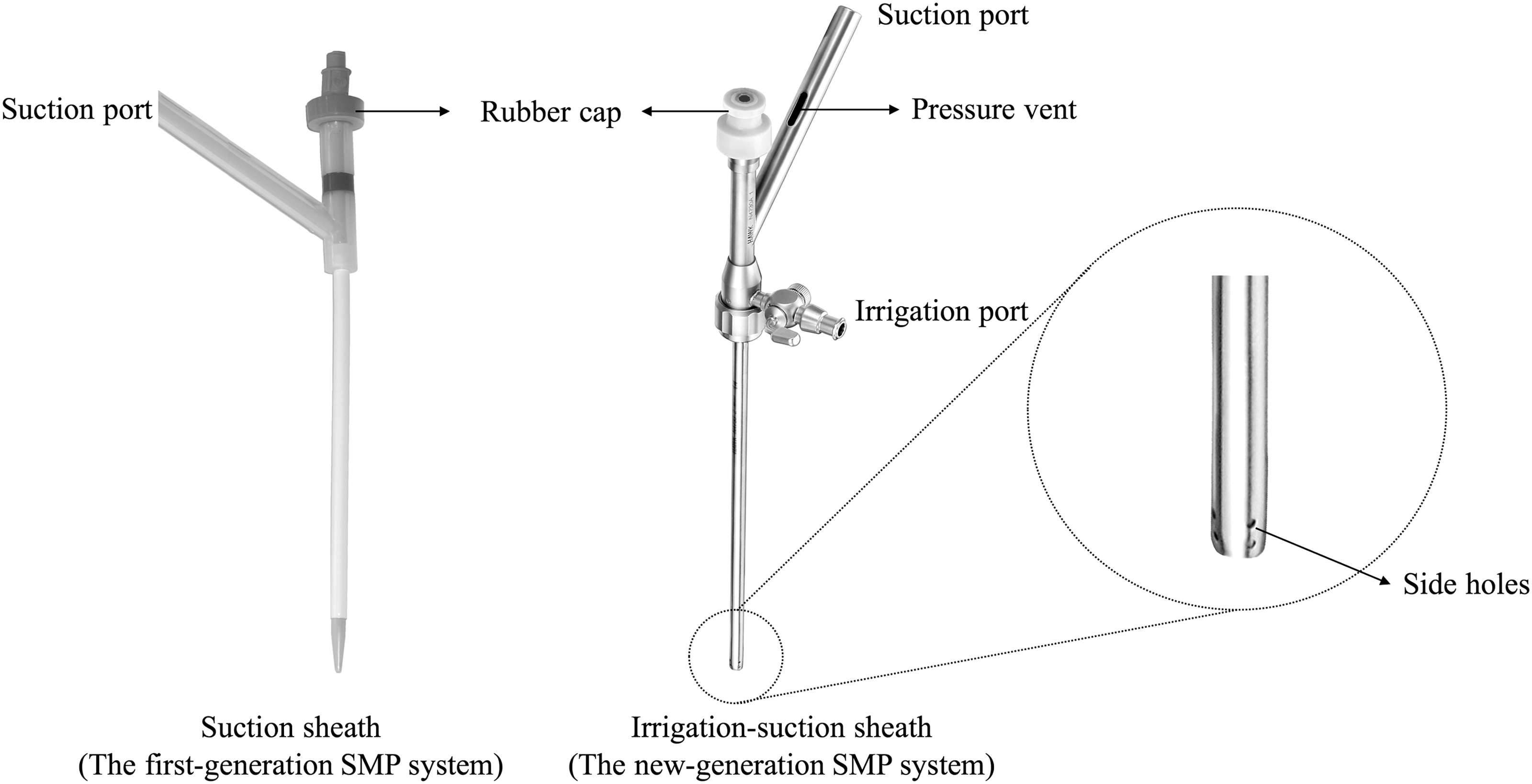
The working sheath used in the first- and new-generation SMP system. SMP = super-mini-percutaneous nephrolithotomy.
The new-generation SMP system consists of an 8F miniaturized nephroscope and a newly designed irrigation/suction sheath. The nephroscope has a 3.3F working channel. The irrigation/suction sheath is a two-layered metal structure available in 12F to 14F. The gap between the two layers of the sheath works as a channel for the irrigation water, and the central lumen of the sheath functions as a conduit for continuous suction (Fig. 1). Continuous negative pressure aspirator was connected to the oblique tube, while continuous irrigation was delivered through the irrigation channel of the sheath with a pressure pump.
Surgical technique
Standardized preoperative preparations were carried out as described in our previous study. 10 Preoperative noncontrasted CT was carried out in all patients to assess stone burden and renal anatomy. The stone surface area was estimated using computerized systems on CT scans. The preoperative stone assessment was performed by using the Guy's stone scoring system according to Thomas and colleagues. 11 Patients with positive preoperative urine culture were treated with appropriate antibiotics based on culture sensitivity result and local microbiology protocol at least 72 hours before SMP. Patients who had negative urine culture received a single dose of broad-spectrum antibiotic prophylaxis on induction.
Our technique of SMP has been described in detail elsewhere 7,9,12 and is summarized herein. Under general anesthesia, a 5F ureteral catheter was first inserted into the target kidney in a retrograde manner using ureteroscope. A Foley catheter was placed into the bladder to provide drainage during the procedure. The patient was then placed in the prone position. Percutaneous access was achieved using an 18-gauge coaxial needle to puncture the desired calix under fluoroscopic or ultrasonic guidance. A 0.035” flexible tip guidewire was inserted through the needle. The dilatation was carried out with 10F fascial dilators. Then, a suction/evacuation sheath (first-generation SMP system)/irrigation/suction sheath (new-generation SMP system) were introduced into the pelvicaliceal system.
For the first-generation SMP system, the main irrigation was delivered through the working channel of the endoscope using a pump. For the new-generation SMP system, the irrigation pump was connected to the irrigation port of the irrigation/suction sheath. The suction port of the sheath was connected to the negative pressure aspirator. The negative suction pressure was controlled to a setting of 100 to 150 mm Hg. A specimen bottle could be added between the sheath and the negative pressure aspirator to facilitate stone fragment collection. If multiple nephrostomy tracts were necessary, the same technique and a new irrigation/suction sheath were used for each of the tracts. Then, the irrigation pump and the negative pressure aspirator were connected to the new irrigation/suction sheath.
For both techniques, laser lithotripsy was the stone fragmentation technique of choice. A 200 μm laser fiber was used in the first-generation SMP system, and a larger 550 μm laser fiber was used in the new-generation SMP system. Only in selected patients in whom stones were hard, impacted, or located close to the pelviureteral junction or ureter, a pneumatic device was used to minimize risk of iatrogenic injury to the ureter. The tiny pulverized stone fragments passed alongside the nephroscope and exited through the oblique sluice. When the larger stone fragments were too large to pass around the scope, the nephroscope was withdrawn slowly to just proximal to the bifurcation. An unobstructed channel was therefore created for the evacuation of larger fragments.
At the end of the procedure, a Double-J stent was placed only in the presence of an obstructing inflammatory ureteral edema, ureteropelvic junction obstruction, or concurrent treatment of ipsilateral ureteral stone with rigid ureteroscope. The sheath was removed, and the wound was either sutured or sealed with absorbable gelatin. For patients with significant bleeding or extravasation, a nephrostomy tube was placed.
Postoperative assessment
Low-dose CT with a 2-mm section thickness was obtained for all patients on the morning after the procedure. An absence of visualized stone fragments on CT scans was defined as stone free. Follow-up, including KUB and ultrasonography, was generally scheduled in 3 months.
Endpoints and definitions
The primary outcome of the present study was operating time, which was calculated from the starting of percutaneous puncture to final wound closure. Secondary outcomes were SFR, blood loss (hemoglobin decrease), hospital stay, tubeless rate, and complications measured by the modified Clavien-Dindo classification. 13
Statistical analysis
Differences between the two groups were tested for significance using the t test, Pearson χ 2 , and Fisher's exact test. A two-sided p < 0.05 was considered to be statistically significant. Statistical analysis was performed using SPSS 18.0 software.
Results
Between February 2013 and January 2017, a total of 156 patients who underwent either first- or new-generation SMP were eligible for the study. Of 156 patients, the first 85 consecutive patients underwent SMP with the first-generation device, and the remaining 71 consecutive patients were treated with the new-generation SMP system. The baseline characteristics of the study population for both cohorts of patients are summarized in Table 1. There was no statistically significant difference between the groups concerning age, BMI, stone size, Guy's scores, comorbidities, grade of hydronephrosis, and positive preoperative urine culture.
SMP = super-mini-percutaneous nephrolithotomy.
The new-generation SMP had a shorter operation time (39.3 vs 50.5 min, p = 0.016) and a postoperative hospitalization time (2.1 vs 3.0 days, p < 0.001) than the first-generation SMP. The SFRs were similar between the two groups (one-session SFR 90.1% vs 88.2%, p = 0.923; overall SFR at 3 months postoperatively 97.2% vs 96.4%, p = 1.000). No patients in both groups needed to be converted to standard PCNL. The puncture site, location of access tract, tubeless rate, the changes in the hemoglobin, and creatinine levels before and after operation all showed no significant differences between the groups (Table 2).
The overall operative complication rates, using the Clavien-Dindo grading system, 13 were similar between the groups. There was no difference in postoperative fever among the groups. None of the patients from both cohorts required blood transfusion postoperatively, although one patient (1.2%) who underwent the first-generation SMP required selective arterial embolization postoperatively for the development of an intrarenal pseudoaneurysm. Two patients (2.4%) in the first-generation SMP group developed urosepsis following surgery and required a treatment course of intravenous antibiotics, supportive therapy, and enhanced monitoring (Table 2).
Stone analysis was obtained in 83 (97.6%) and 65 (91.5%) of the patients in the first- and new-generation SMP groups, respectively. Calcium oxalate was the most prevalent stone composition in both groups (68.7% vs 81.5%, p = 0.075) (Table 3).
RPP was measured in 9 cases and 38 cases in the first- and new-generation SMP groups, respectively. The RPP was measured using a baroreceptor, which was connected to an open-ended ureteral catheter during the operation of SMP. All 47 patients had a single 14F percutaneous tract. Both groups had a low average RPP, with an overall pressure being less than the backflow pressure (30 mm Hg) (Table 4). The overall RPP in the new-generation SMP was higher than the first-generation SMP (21.3 ± 10.2 vs 14.0 ± 5.6 mm Hg, p < 0.001). The accumulated time intraoperatively with an RPP ≥30 mm Hg was greater in the new-generation SMP compared with the first-generation SMP (92.3 ± 88.4 vs 14.3 ± 18.0 s, p < 0.001).
RPP = renal pelvic pressure.
Discussion
Miniaturized PCNL procedures have gained increasing popularity in the recent years, with an aim of reducing percutaneous tract size to further lower complication rates while maintaining good SFRs. The tract size has decreased considerably in the newer miniaturized modalities of PCNL such as mini-PCNL, 4 UMP, 14 and micro-PCNL, 15 but concerns remained with regard to poorer endoscopic view and difficultly in removing stone fragments via the smaller tract when compared with conventional PCNL. As such, we have devised the first-generation SMP system utilizing suction to remove the stone fragments and to maintain a low RPP. The first-generation SMP used a modified access sheath with a suction function to improve the stone removal. The way to remove stone fragments in SMP is different from the UMP and micro-PCNL. In UMP, 14 the stone fragments are removed mainly by pressured irrigation. In micro-PCNL, 15 the stone fragments are simply left in situ for later spontaneous passage. In SMP, the stone fragments are removed by active suction, with the ultimate goal of rendering the patient stone free at the end of the procedure. The first-generation SMP has been shown to have good outcomes in the treatment of moderate-sized renal calculi in both pediatric 12 and adult patients. 7
Despite the success of first-generation SMP, the problem of limited irrigation by using miniature nephroscope still existed. In the first-generation SMP, the main irrigation is delivered through the same channel used for working instruments. This caused a dramatic reduction in irrigation efficiency once the laser fiber or pneumatic lithotripter probe was inserted. To solve this problem, we designed an irrigation/suction sheath to improve the irrigation efficiency in the new-generation SMP. The irrigation/suction sheath is a two-layered metal structure. The space between the two layers of the sheath forms an independent irrigation channel. Using this new-generation SMP system, the irrigation is delivered through the sheath and thereby freeing up a working channel space of the nephroscope, which allows utilizing larger instruments (550 μm laser fiber or 1.0 mm lithotripter) without reducing the irrigation efficacy.
Although the first- and the new-generation SMP system both utilized active suction to remove the stone fragments, the hydrodynamic mechanisms for retrieval of fragments are different (Fig. 2). In the first-generation SMP system, the inflow and outflow take place in the same lumen of the sheath. The inflow could sometimes partially offset the effect of outflow and push the stone fragments back to the collecting system, leading to migration of stone fragments and lengthened operation time. The irrigation/suction sheath in the new-generation SMP systems allows the inflow and outflow separately so that the problem is resolved (a one-way flow is created as the inflow that comes out of the irrigation channel of the sheath is immediately aspirated through the suction conduit of the sheath). This improved effective irrigation/suction sheath potentially explains why the new system leads to a more effective surgery and shortens the operative time in our study (39.3 vs 50.5 min, p = 0.016).
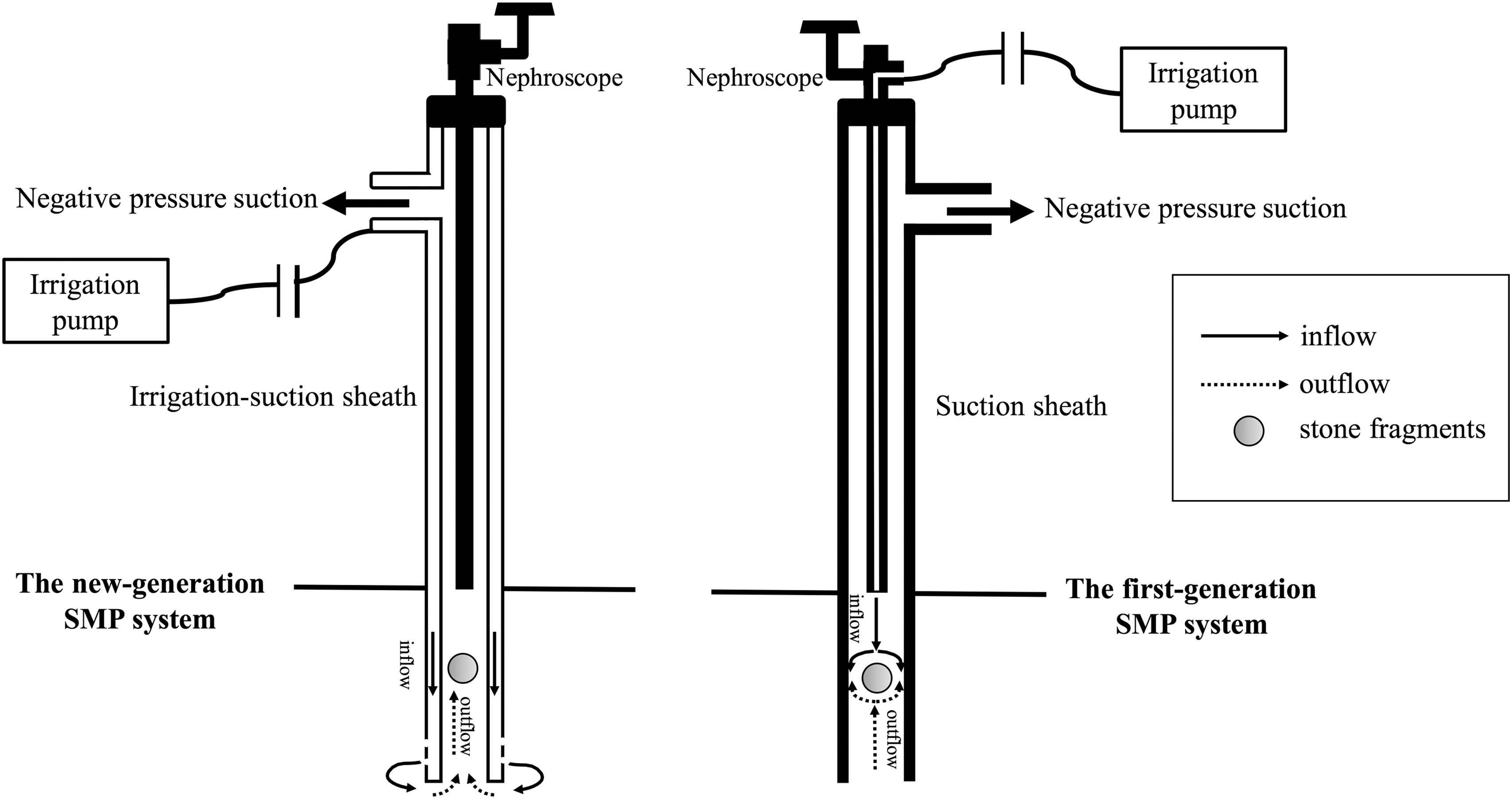
The hydrodynamic mechanisms for retrieval of fragments in the first- and new-generation SMP systems.
The sheath in the first-generation SMP is made of plastic material to have less traumatic effects to the renal parenchyma during the procedure. However, its associated flexibility had led to nephroscope damage on scope bending. Another disadvantage in using plastic material was that the sheath can be only used once. As a result, we have changed the irrigation/suction sheath in the new-generation SMP to medical-grade steel. In this study, the mean drop in hemoglobin levels was similar in the two groups. Transfusion was not required in both groups. There was no evidence in the study to suggest that the use of a metal sheath increased the incidence of renal trauma or blood loss compared with the use of a plastic sheath.
The increasing pixel resolution of nephroscope is another improvement in the new-generation SMP system. The improvements in the new-generation SMP system are summarized in Table 5.
In the present study, the new-generation SMP results in shorter length hospitalization than the first-generation SMP (2.1 vs 3.0 days, p < 0.001). The most likely reasons were the increasing clinical experience in the use of the SMP within the unit rather than purely due to the upgrade in the device.
In this study, the first- or new-generation SMP both had a low RPP less than the backflow level (30 mm Hg), although the new-generation SMP brought a higher average RPP and a longer accumulated time of RPP ≥30 mm Hg. The reasons for the difference might be the increasing irrigation during the new-generation SMP by using the irrigation/suction sheath. Theoretically, a higher RPP and a longer accumulated time of RPP ≥30 mm Hg in the new-generation SMP might make a difference regarding postoperative infection complications such as fever and urosepsis. This, however, was not proven to be the case in the present study.
We acknowledge that there are limitations to this study. First, it was a nonrandomized study. Second, clinical experience gained during the first 2-year period using the first-generation SMP undoubtedly has caused bias toward the outcome of the new-generation SMP used in the latter period of the study. However, we believe that such bias is not significant as SFR and postoperative complication rates were similar in both cohorts.
Conclusion
The clinical outcomes of the new-generation SMP in patients with moderate-sized renal stone were comparable when compared with the first-generation SMP. New-generation SMP system using an irrigation/suction sheath was associated with better irrigation, a more efficient hydrodynamic mechanism for retrieval of fragments, and, hence, a shorter operative time than the first-generation SMP system.
Footnotes
Acknowledgments
This work was financed by a grant from the National Natural Science Foundation, China (No. 81670643 and 81370804) and the Science and Technology project in Guangzhou (No. 201604020001).
Author Disclosure Statement
No competing financial interests exist.