
Abstract
Purpose:
The purpose of this study was to compare the efficacy of tolterodine and gabapentin vs placebo in catheter related bladder discomfort (CRBD) following percutaneous nephrolithotomy (PCNL).
Materials and Methods:
This study was a double-blind parallel group randomized clinical trial. Patients who were candidates of PCNL were enrolled. Patients were randomized to treatment groups of tolterodine 2 mg orally (PO) (group T, n = 50), gabapentin 600 mg PO (group G, n = 50), and placebo (group P, n = 70) 1 hour before operation using balanced block randomization. The primary endpoint of interest was visual analog pain scale in 1, 3, 12, and 24 hours after the operation. Secondary endpoints included rescue analgesic use (opioid and nonopioid).
Results:
The frequency of severe CRBD in 1,12, and 24 hours after the operation was 4%, 4%, and 6% in group T vs 4%, 0%, and 2% in group G vs 47%, 14%, and 6% in the P group (p < 0.001). The number of paracetamol injections for CRBD in the T and G groups was significantly lower than the placebo group (1.8 ± 0.8 vs 1.8 ± 0.7 vs 3.6 ± 0.7, p < 0.001). Likewise the number of pethidine injections in the T and G groups was significantly lower than the placebo group (0.42 ± 0.54 vs 0.68 ± 0.62 vs 2.4 ± 0.64, p < 0.001). In patients with history of Double-J insertion, the severity of CRBD was lower in all treatment groups.
Conclusions:
Preoperative administration of oral tolterodine or gabapentin reduces postoperative CRBD and the need for rescue analgesics as much as 24 hours after surgery. Patients with history of Double-J insertion experience less CRBD.
Introduction
W
CRBD is thought to occur as a result of bladder muscular contractions due to activation of bladder muscarinic receptors. Antimuscarinic agents such as tolterodine and oxybutynin are competing antagonists of the bladders' muscarinic receptors and adjust the overstimulation of the sacral reflex center. Therefore, these agents had been the mainstay of CRBD treatment.
Gabapentin is derived from gamma-Aminobutyric acid and reduces the release of glutamate. Glutamate is a neurotransmitter which transfers pain to the central nervous system. It attaches to the α2δ1 and 2 subunit in voltage gated calcium channels and reduces the flow of calcium in the central nervous system. Gabapentin also stops new synapses from being formed. It has been observed that the upregulation of afferent fibers (C-fibers) in the bladder is the cause of lower urinary tract symptoms such as urgency and frequency. Gabapentin inhibits the C-fibers and based on its safety and efficiency is a suitable choice for lower urinary tract symptoms. The efficacy of gabapentin in overactive bladder refractory to anticholinergic medications has also been demonstrated. 7
Most previous studies evaluated medications within the same classification, including antimuscarinic agents 2,8 –12 and antiepileptic agents 5,7,13 on CRBD. A recent review article on treatments for CRBD emphasized the need for direct comparisons between medications of different classifications. 14
The purpose of this study was to perform a direct head to head comparison for evaluation of the efficacy of tolterodine vs gabapentin vs placebo in CRBD following percutaneous nephrolithotomy (PCNL).
Materials and Methods
This study is a parallel group randomized clinical trial. Patients who were referred to our center for PCNL operation from March 2016 to December 2016 were included. Inclusion criteria for PCNL were as follows: renal stones ≥2 cm on longest diameter, smaller stones resistant to extracorporeal shockwave lithotripsy, large proximal ureteral stones, age ≥18 years, and American Society of Anesthesiology score of I (no prior history of acute or chronic illnesses, including malignancies, systemic diseases, chronic infections, and age ≤60 years). Exclusion criteria were as follows: drug or alcohol abuse, allergic reactions to gabapentin, tolterodine or narcotics, painful circumstances which can affect pain assessment, including lower urinary tract symptoms, medical or psychologic circumstances which can affect the patients' communication or tolerance, analgesic use within 12 hours before surgery, urethral pathologies necessitating intervention or causing difficulty in passage of urethral catheter, and change in anesthesia protocol during the operation.
All patients were admitted the day before surgery. Laboratory examinations included complete blood count, creatinine, aspartate transferase, alanine transferase, prothrombin time, partial thromboplastin time, and direct and indirect bilirubin. Patients were randomly allocated to groups of tolterodine (n = 50), gabapentin (n = 50), and placebo (n = 70) using balanced block randomization. The allocated treatments of each patient were recorded in concealed envelopes designated as A, B, or C and were opened after ensuring eligibility. Information regarding visual analog pain reporting was given to each patient by a staff nurse before surgery, and the designated drug was administered according to envelope contents. Envelope A patients were given oral tolterodine 2 mg with a sip of water 1 hour before surgery (designated as group T afterward). Envelope B patients were administered oral gabapentin 600 mg with a sip of water 1 hour before surgery (designated as group G afterward). Envelope C patients were given oral vitamin C (250 mg) with a sip of water 1 hour before surgery (designated as group P afterward). Patients were unaware of the type of medications they received.
Surgical methods
The anesthesia protocol was the same for each patient: Atracurium with a dose of 0.5 to 0.6 mg/kg, fentanyl 5 to 10 mg/kg, Nesdonal 5 to 7 mg/kg, and inhalation isoflurane MAC = 0.8 to 1. After extubation, no drug was used in the protocol. In case of need for change of anesthesia protocol, the patient was excluded from the study.
PCNL operation was performed according to the standard prone position with fluoroscopic guidance as described earlier 15,16 and is summarized below. After cystoscopy a 5F ureteral catheter was fixed to 16F urethral catheter. The urethral catheter was inserted after passing lubricating lidocaine jelly into the urethra and its balloon was filled with 10 mL sterile water. If the insertion of ureteral catheter was not possible through cystoscope, it was inserted by use of ureteroscope. Access was obtained in prone position under fluoroscopic guidance, and the tract was dilated to 30F by single shot Amplatz dilators. Lithotripsy was accomplished using pneumatic lithotripter. The procedure was typically terminated leaving an internal (Double-J) or external ureteral catheter in place. The 16F urethral catheter, which was inserted after cystoscopy, was fixed with adhesive tapes to the suprapubic area.
Outcome measurement
The primary endpoint of interest was visual analog pain scale (VAS) which was measured 1, 3, 12, and 24 hours after surgery by staff nurses. The nurses who measured VAS were blinded to treatment allocations of patients. VAS scores were graded as follows: 0, no pain; 1 to 4, mild pain; 5 to 7, moderate pain; and ≥8, severe pain based on the average finding of previous studies. 17 –20
Secondary endpoints included the number of injections of non-narcotic agents (paracetamol) and narcotic agents (pethidine 25 mg). These rescue analgesics were given to patients with moderate-to-severe VAS (VAS score >4).
In the postoperative period, vital signs, including temperature, blood pressure, heart rate, and respiratory rate, were recorded at 1, 3, 12, and 24 hours after operation.
Statistical analysis
Data were entered into the SPSS ver. 21 software for analysis. The statistician was aware of the existence of 3 distinct study groups, but was unaware of their specifications. Comparison of quantitative variables over three study groups was performed with one way analysis of variance. Qualitative variables were compared using chi square test. The statistician was blinded to the nature of the treatment groups coded as A, B, and C.
The sample size calculation was performed considering 30% reduction in CRBD with medications with type I error rate of 5% and type II error rate of 10%. The size of the control group was chosen 1.4 times the size of each intervention arm. As a result, 48 samples were calculated for each intervention arm and finally 50 samples were chosen regarding the possibility of attrition. As a result, 50 samples in each intervention arm (groups T and G) and 70 samples for the control group (group P) were enrolled.
The ethics of this study has been approved by the ethics committee of the Iran University of Medical Sciences with the approval code of IR.IUMS.REC1395.9221254002 and were in accordance with the 1964 Declaration of Helsinki and its later amendments. All patients were explained about the study protocol in their own language. Written informed consent was obtained.
This study has been registered at the Iranian Registry of Clinical Trials with the registration number of IRCT201204066504N3.
Results
During the study period, 249 patients were assessed for eligibility. Ten patients were excluded for age >60 years, 5 patients for chronic use of pain medication, 24 patients for lower urinary tract symptoms, 3 patients for history of transurethral resection of prostate, 4 patients for history of lower urinary tract surgery/instrumentation, 6 patients for probable overactive bladder or neurogenic bladder, 15 patients for diabetes mellitus, and 12 patients refused to participate. Fifty patients were enrolled in each treatment groups of T and G, and 70 patients were enrolled in the placebo group. Details of patients' enrollment algorithm are outlined in Figure 1.

Patients' flow diagram.
Details of patients' demographic data and operations characteristics are presented in Table 1.
PCNL = percutaneous nephrolithotomy; SWL = extracorporeal shockwave lithotripsy.
Figure 2 illustrates the confidence interval for visual analog pain scores measured after PCNL separately for the three intervention and control groups. As evident, the difference in VAS is highest between treatment groups and the control group 1 hour after surgery. The magnitude of difference ameliorates toward 24 hours after surgery when patients in the placebo group still experienced higher average pain scores in relation to treatment groups of T and G.
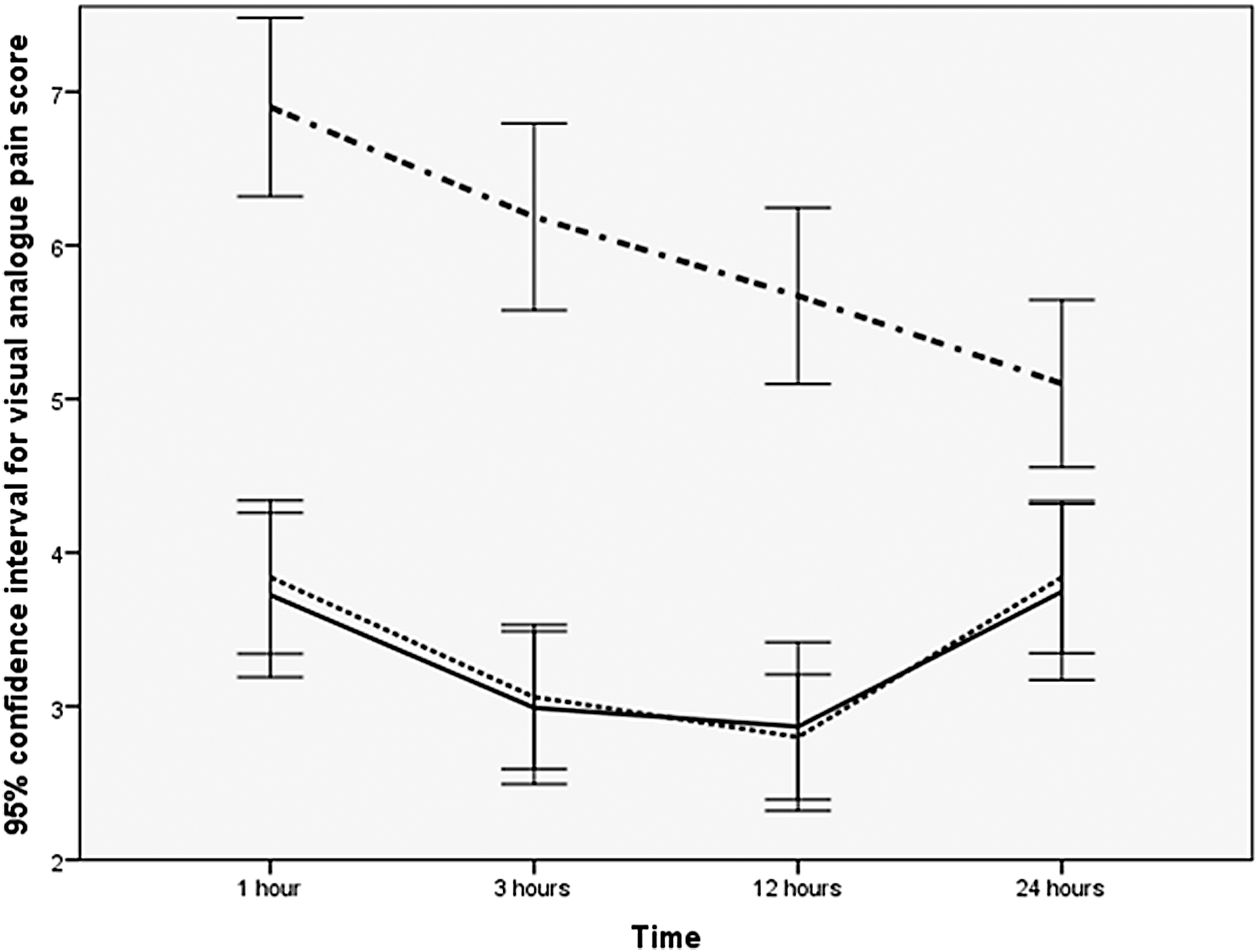
VAS scores in different treatment groups in postoperative hours. (Dash-dot indicates the placebo group, solid line indicates the tolterodine group, and dotted line indicates the gabapentin group). VAS = visual analog pain scale.
The numbers of patients in each category of mild, moderate, and severe pain separately for the 1st, 3rd, 12th, and 24th postoperative hours are presented in Table 2. Moderate and severe pain were experienced in 24%, 20%, and 76% of patients in groups T, G, and P, respectively, during the first postoperative hour. These frequencies decreased to 12%, 8%, and 63% 12 hours after surgery. The relative frequencies of moderate-to-severe CRBD increased slightly to 24% and 20% in the intervention groups (T and G), while it continued to decrease to 59% in the placebo group (Fig. 2 and Table 2).
Data are presented as number of patients in each category.
CRBD = catheter related bladder discomfort.
Multivariable repeated measures design was used to investigate the independent factors that had an influence on pain perception after surgery. Age, body mass index, stone size, number of tracts, operation duration, history of PCNL surgery or extracorporeal shockwave lithotripsy, and insertion of Double-J or ureteral catheter were not statistically significant predictors of CRBD. Only history of Double-J insertion was a statistically significant predictor of postoperative CRBD (P = 0.002).
Figure 3 illustrates that pain perception in patients with a history of Double-J insertion was lower in comparison with patients without such a history. This reduction in pain perception was observed in all study groups, including the control group.
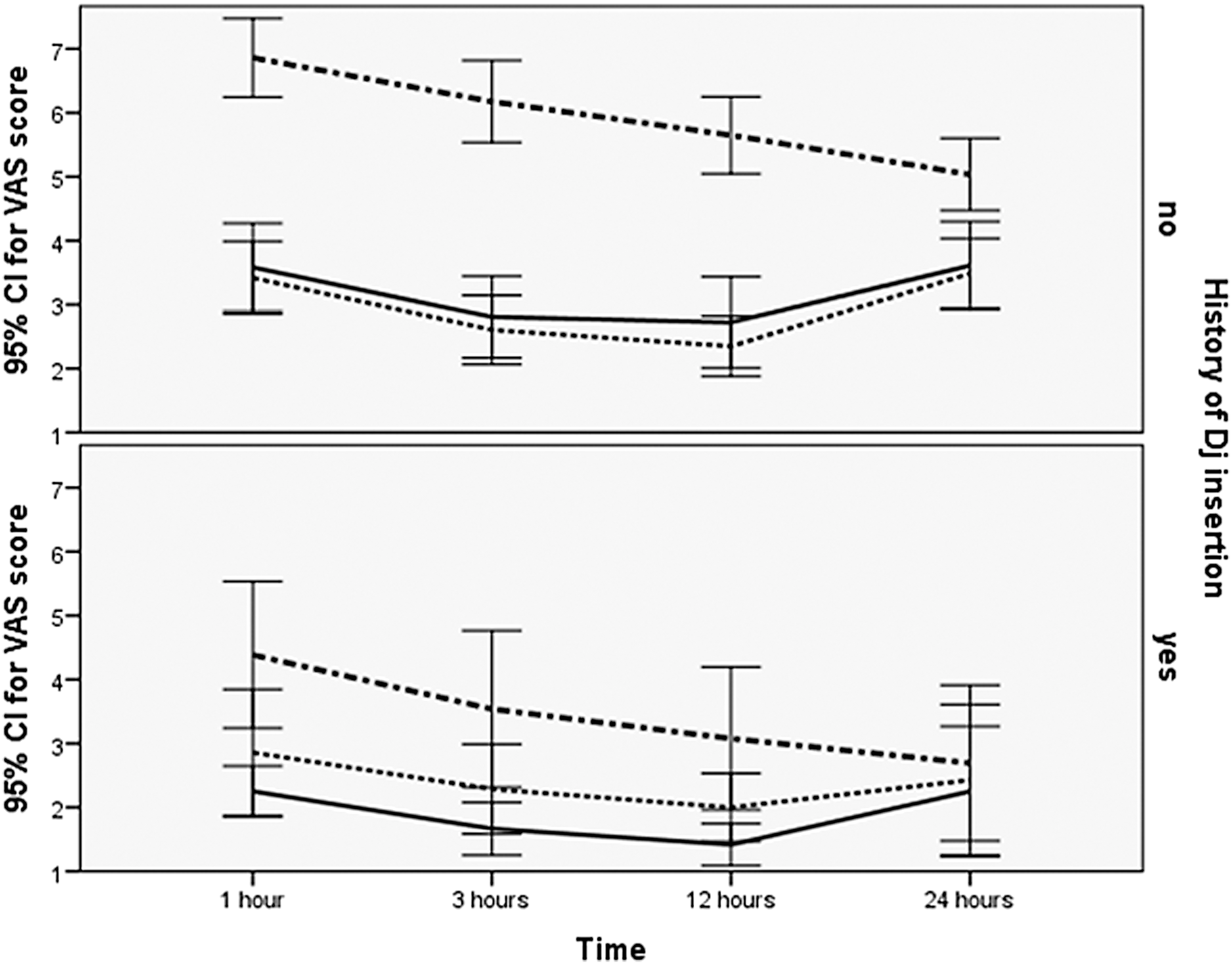
VAS scores in different treatment groups in postoperative hours separately for patients with and without history of Double-J insertion. (Dash-dot indicates the placebo group, solid line indicates the tolterodine group, and dotted line indicates the gabapentin group.)
Discussion
The results of this study reveal that preoperative oral administration of tolterodine 2 mg or gabapentin 600 mg significantly reduces postoperative CRBD in patients who undergo PCNL. This reduction in CRBD was evident as much as 24 hours after surgery when our last measurement was made. Interestingly insertion of Double-J vs external ureteral catheter has no statistically significant influence on postoperative CRBD. However, history of Double-J insertion ameliorated CRBD in all study groups probably due to their previous experience of the symptoms. As indicated previously, no previous study has compared drugs of different classifications in reducing postoperative CRBD specifically an antimuscarinic agent with an antiepileptic agent.
The influence of various medications on postoperative CRBD has been the subject of several previous studies. Various medications, including antimuscarinic agents, antiepileptic agents, anesthetics, and analgesics, have been used to treat postoperative CRBD. In most studies, the efficacy of administration of medications on postoperative CRBD has been confirmed.
Zhang and colleagues 8 in a randomized prospective trial evaluated the influence of preoperative and postoperative administration of solifenacin 5 mg orally (PO) for 2 weeks on postoperative CRBD in transurethral resection of bladder tumor (TURT) patients. They reported 26% reduction in CRBD in the intervention group 6 to 12 hours after the operation which reduced to 15% at 48 to 72 hours of the surgery.
Agarwal and colleagues 2 in a randomized double-blind trial compared the administration of oxybutynin 5 mg PO vs tolterodine 2 mg PO vs placebo 1 hour before surgery on CRBD. They reported 23% to 25% reduction in CRBD in the intervention groups in cost of more dry mouth (46–51% in the intervention group vs 19% in the placebo group).
Bala and associates 5 compared the preoperative administration of gabapentin 1200 mg PO (G1) vs gabapentin 600 mg PO (G2) vs placebo on postoperative CRBD after TURT surgery in a randomized clinical trial. They reported 0% to 26% CRBD in the G1 group vs 9% to 66% in the G2 group vs 66% to 90% in the placebo group (p < 0.05).
Similarly, Agarwal and colleagues 13 randomized 108 patients undergoing elective PCNL to gabapentin 600 mg PO and placebo. They reported severe CRBD in 1 and 2 hours after surgery in 0% and 3% vs 42% and 25% in the gabapentin and placebo groups, respectively.
In all cited studies, the efficacy of administration of a drug or different doses of the same drug or the efficacies of different drugs within the same drug classification on CRBD has been demonstrated. To our best knowledge, no study has compared the efficacies of drugs of different classifications in postoperative CRBD.
A systematic review on the management of CRBD in elective surgeries emphasizes that wise selection between different treatment options necessitates direct comparative studies on their efficiencies. 14
We observed statistically significant decrease in postoperative CRBD in patients who received oral tolterodine or gabapentin before operation in line with prior publications. The need for rescue medications, including intravenous analgesics and opioids, was markedly less in treatment groups in comparison with the placebo group. Interestingly the difference in postoperative CRBD was not statistically significant between treatment groups of tolterodine vs gabapentin.
Gabapentin as explained earlier in the Introduction section is both a centrally and peripherally acting medication. Tolterodine on the contrary is a peripherally acting medication, which inhibits bladder muscarinic receptors. The pain of CRBD is medicated through bladder pathways; however, the pain of PCNL is mediated through kidney receptors which should theoretically be unresponsive to tolterodine. The result of our study clearly demonstrated the equivalency of CRBD suppression by tolterodine in comparison with gabapentin. Unfortunately, we did not assess postoperative PCNL pain; however, theoretically gabapentin can be more effective on the perception of postoperative PCNL pain due to its central effects. Therefore, one can conclude that gabapentin will result in more overall suppression of CRBD and postoperative PCNL pain in comparison with tolterodine although this conclusion cannot be directly extracted from our crude data but can be the subject of future studies.
Another interesting finding was that the reduction in perception of CRBD was maintained as much as 24 hours after oral administration of tolterodine or gabapentin when our last VAS measurement was performed. Studies which evaluated the preoperative oral administration of an antimuscarinic agent or an antiepileptic agent on postoperative CRBD evaluated CRBD as much as 6 hours after surgery. 2 –4,6,7,9,10,12,13 No study with only a single oral preoperative administration of medication has evaluated CRBD beyond 6 hours after administration when theoretically the medical influence of medications like gabapentin which need every 6 hour administration disappears. Nonetheless, the reduction in CRBD perception was maintained as much as 24 hours after operation when our last measurement was made. We think that this observation could be explained by psychologic influence of less prior CRBD during early postoperative hours on their later reporting of CRBD; however, we have no hard proof for our claim.
Shariat and coworkers 4 investigated the influence of intravenous administration of ketamine after induction of anesthesia on postoperative CRBD. They reported that postoperative difference on CRBD was only observed 1 hour after operation. Two and 6 hours after the operation the CRBD perception in treatment groups was not statistically different. On the contrary, most other studies which evaluated preoperative oral administration of antimuscarinic, antiepileptic, anesthetic, or analgesic agents on postoperative CRBD, reported the maintenance of influence as much as 6 hours after surgery when their last measurements were made. 2,3,6,7,10,12,13,21
Another interesting finding of this study was the significantly reduced CRBD perception in patients with history of Double-J insertion in all treatment groups. We could not find evidence for investigation of such relationship in prior studies. 22,23
The limitations of this study include failure to simultaneously investigate the influence of combined administration of tolterodine and gabapentin. As a marked percentage of patients in each treatment group experienced postoperative CRBD despite oral medication, it is advisable to study the combined efficacy of an antimuscarinic agent with an antiepileptic to observe their combined efficacy on CRBD regarding the safety profile of their administration with regard to absence of deleterious side effects in all published studies. We cannot exclude the possibility of misperception of patients' subjective assessment of CRBD by VAS from the overall postoperative PCNL pain; however, the location of PCNL pain is away from CRBD which is felt suprapubic or over the urethra, and the results of our study support the observation that medications with only possible effect on CRBD (tolterodine) suppressed CRBD pain equivalently to centrally and peripherally acting medications like gabapentin. VAS has not been standardized for measuring CRBD discomfort. We also failed to observe for side effects of prescribed medications; however, several previous studies reported the frequency of medication side effects and most agreed that side effects however frequent are tolerable. 14
Conclusions
The results of this study approve the efficacy of preoperative oral administration of tolterodine 2 mg or gabapentin 600 mg 1 hour before surgery on CRBD during the first 24 hours after surgery in patients who undergo PCNL. The need for rescue analgesic or opioid to relieve CRBD is markedly less in patients premeditated with the above drugs. In patients with a history of Double-J insertion, the perception of CRBD is less in comparison with patients without such a history.
Footnotes
Author Disclosure Statement
No competing financial interests exist.