
Abstract
Port placement for robot-assisted laparoscopic urologic surgery can be critical to effective completion of the minimally invasive procedure. An ideal port template would allow unhampered access to all critical structures during surgery, easy access for the bedside assistant, and minimization of arm collision with the fewest ports necessary to minimize cosmetic impact. We present a comprehensive plan for the placement of ports across different procedures for a variety of upper tract (radical/partial nephrectomy, retroperitoneal radical/partial nephrectomy, and pyeloplasty), lower tract (prostatectomy, and cystectomy), combined upper/lower tract (nephroureterectomy, retroperitoneal lymph node dissection), and female pelvic surgeries. Optimal exploitation of these tips across the different procedures for different generations of robots will help in effective execution of robotic urologic surgery.
Introduction
I
To perform these procedures, it is essential that ports be placed in a manner to allow for maximal instrument excursion, minimal arm collision, and ease of access to structures during key portions of the procedure. We aim to describe our experience of port placement for both upper and lower urinary tract procedures with the hope that these tips may be helpful and serve as a guide when performing robot-assisted laparoscopic surgery for a variety of urologic indications.
Differences between Xi and Si
The Xi® and Si® robotic platforms differ in many ways. Advantages unique to the Xi include a wider field of view, docking flexibility, built-in mechanisms to prevent arm clashing, the ability to perform multiquadrant surgery, end chip camera with autofocus feature, and a smaller (8 mm) lens camera that can be placed into any robotic port. However, with these modifications came new challenges such as an increase likelihood of camera smudging secondary to residue buildup or fogging. Techniques to overcome these new challenges include using the 2 × digital zoom feature, a warm room or warming thermos, and either active manual or facilitated smoke evacuation (Airseal®). The Xi robotic platform consists of instruments that have longer working lengths, thereby minimizing the potential for arm collisions. Port placement is largely similar between the Si and Xi robotic platforms, with specific differences as highlighted in the following sections: upper urinary tract, combined upper and lower urinary tract, lower urinary tract, retroperitoneal lymph node dissection, and female pelvic surgery.
Upper Urinary Tract
Nephrectomy/partial nephrectomy
We use the transperitoneal approach in the majority of cases, which allows for easier access to upper, interpolar, and lower pole tumors. The retroperitoneal approach is extremely useful for a subset of patients who have a lengthy history of previous abdominal surgeries, patients on peritoneal dialysis, and patients with posteriorly located tumors. Both templates are discussed below in the subsection entitled transperitoneal and retroperitoneal template for the da Vinci Si/Xi.
The patient is positioned in full flank flush against the edge of the bed and the table slightly flexed to increase the space between the costal margin and the anterior superior iliac spine (ASIS), lowering the ASIS resulting in greater space for the fourth arm. The ipsilateral hand is placed on an arm rest or by the side of the torso with appropriate padding.
Transperitoneal template for the da Vinci Si
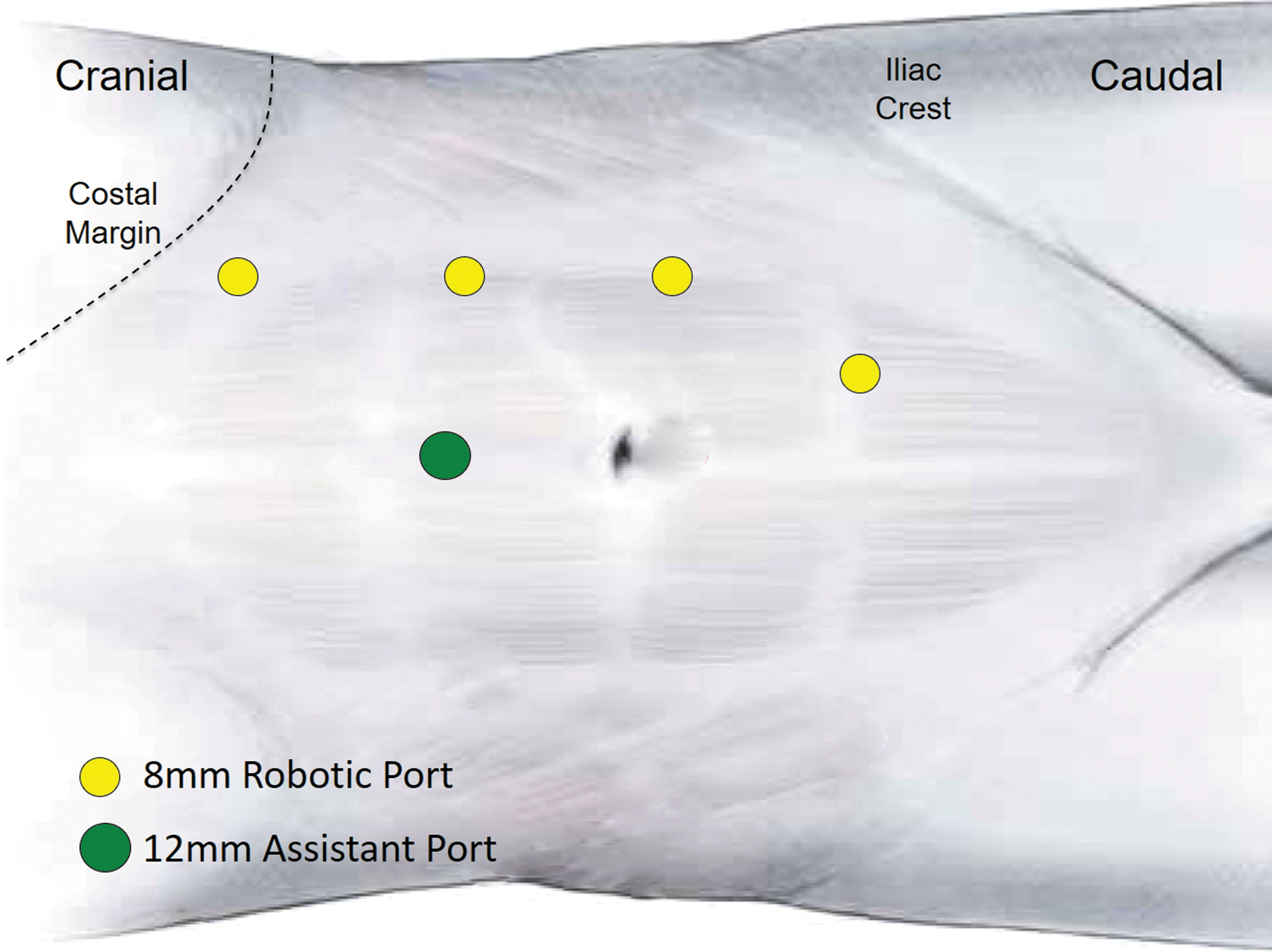
Figure 1 demonstrates our port placement template for transperitoneal renal surgery utilizing the da Vinci Si platform. If using a 0° or 30° down stereoscopic lens, a 12 mm camera trocar is placed through the lateral edge of the rectus muscle with two 8 mm robotic ports on either side. 2 The cranial 8 mm robotic trocar is placed at the lateral edge of the rectus muscle ipsilaterally between the xiphoid process and the umbilicus ∼5 cm away from camera port with the second caudal 8 mm robotic trocar placed at the lateral edge of the rectus muscle ∼5 to 7 cm away from the camera trocar. A 12 mm assistant trocar in the midline, between the cranial 8 mm robotic and 12 mm camera port, with another optional 5 mm subxiphoid port for liver retraction during right-sided procedures, if needed, should be placed. A fourth 8 mm bariatric robotic trocar is placed 2 cm superior to the ASIS along the axillary line. In general, irrespective of robotic platform, we utilize a four-armed robotic technique, incorporating an 8 mm bariatric (longer robotic cannula) trocar to minimize arm collisions with the other robotic arms and assistant port.
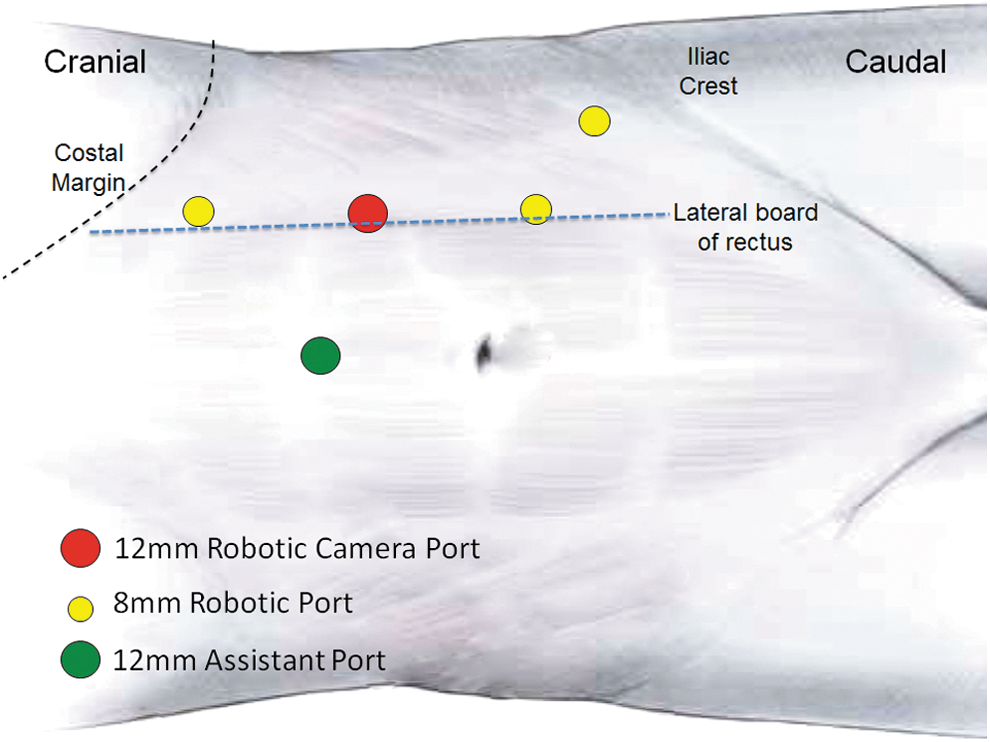
Left-sided kidney surgery for da Vinci Si. Right-sided surgery will be a mirror image.
Alternatively, the 12 mm camera port may be placed laterally, between the anterior axillary line and midclavicular line, 3 to 4 cm below the costal margin. The robotic working ports should be placed medially, ∼10 cm away from the camera port in an effort to triangulate toward the kidney. 3
Transperitoneal template for the da Vinci Xi
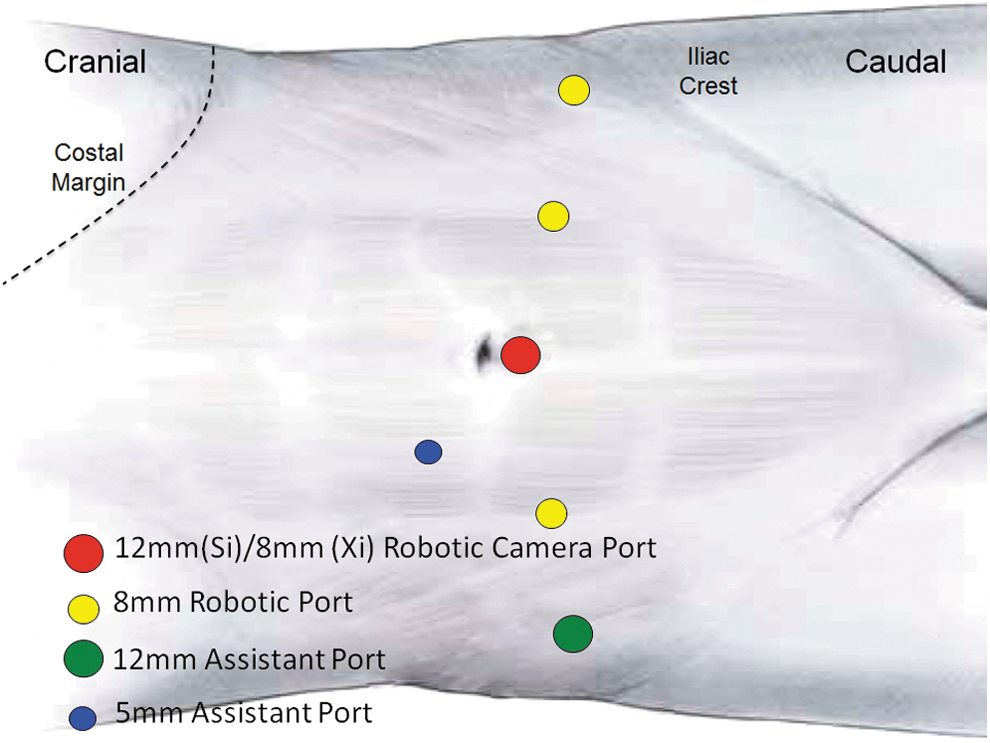
Figure 2 illustrates port placement for the transperitoneal approach when using the da Vinci Xi robotic platform. All 8 mm ports are arranged in a linear manner along the lateral rectus sheath on the ipsilateral side. The camera port is placed along the rectus sheath just cranial to the umbilicus. Three additional ports are placed along the sheath with one about 6 to 7 cm cranial to the camera, and two ports placed caudal to camera about 6 to 7 cm apart. The assistant port can be placed midline between the cranial and camera robotic ports.
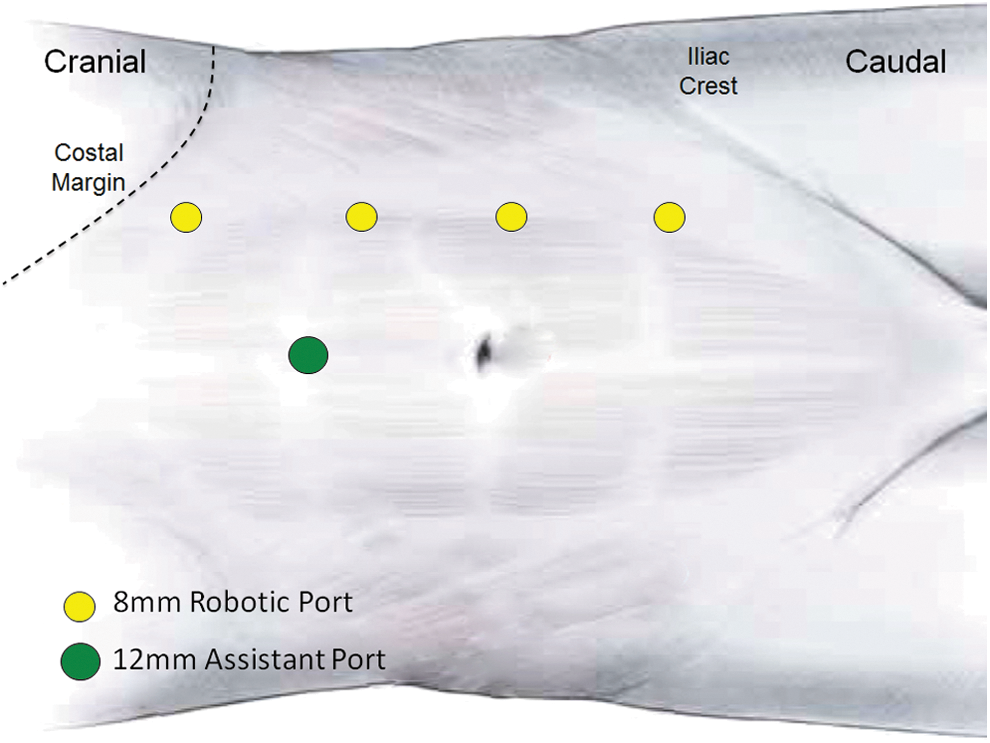
Left-sided kidney surgery for da Vinci Xi. Right-sided surgery will be a mirror image.
With the new da Vinci Xi, docking has simplified. The patient cart possesses four robotic arms that swivel on an overhead boom, enabling 342° of rotation and allowing the robot to be docked from any position. Moreover, infrequent clashing with the armrest can be achieved by using the rotating function to move the “elbow” of the robotic arm away from the armrest. We have performed surgeries with the robotic base both parallel and perpendicular to the patient bed.
Retroperitoneal template for the da Vinci Si
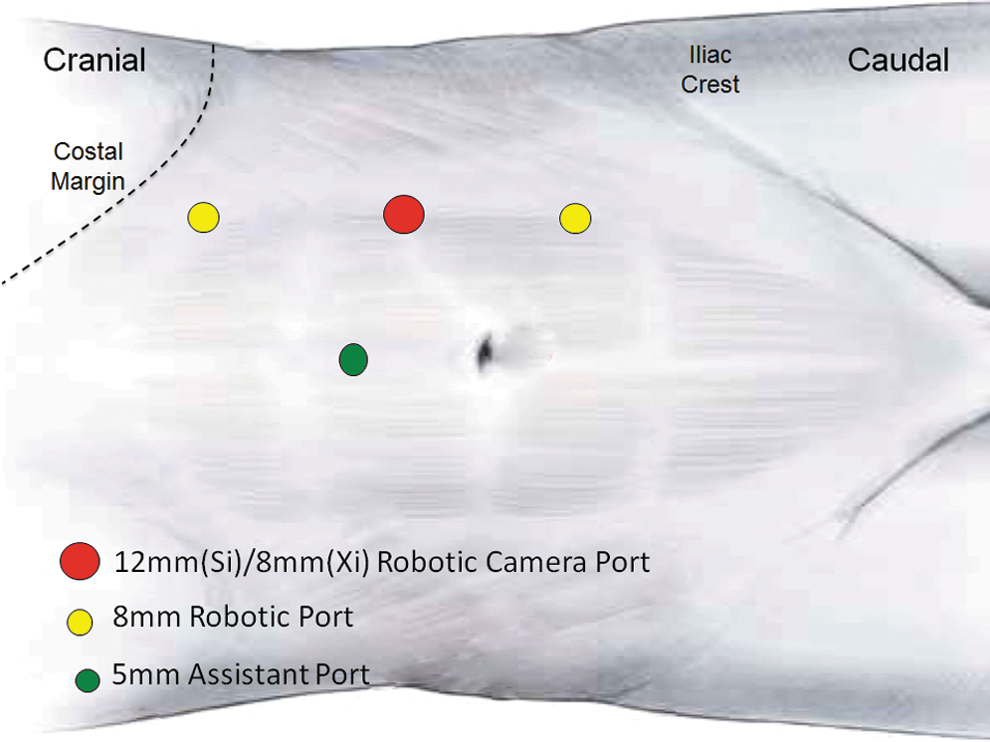
Retroperitoneal access can be achieved by placing the patient in full flank position with full table flexion and an anterior tilt. A 1.5 cm incision is made about 3 to 4 cm cranial to the ASIS or below the tip of the 12th rib. The incision is carried out through the lumbodorsal fascia to access the retroperitoneal space, which is further developed with the assistance of a balloon dilator such as OMS-PDB 1000 Autosuture™ (Tyco Healthcare, U.S. Surgical, Norwalk, CT). Next, a 12 mm blunt tip balloon trocar (Autosuture; Tyco Healthcare, U.S. Surgical) is placed for the camera. The two 8 mm working robotic instrument ports are placed under vision in line or just caudal to the umbilicus. A fourth arm can be placed medially, in line with the other working ports. The assistant port is placed between camera and medial working port (Fig. 3). To facilitate placement of the ports, a laparoscopic Kittner may be utilized to sweep the peritoneum away.

Right-sided retroperitoneal renal surgery using the da Vinci Si/Xi. Left-sided port placement would be a mirror image. The camera is placed 2 cm cranial to the ASIS. The working ports are placed in the anterior axillary and posterior axillary lines 7.5 cm away from the camera port. The assistant port is placed caudal to the anterior working port along the posterior axillary lines. ASIS = anterior superior iliac spine.
Alternatively, a 12 to 15 mm incision1.9 cm above the iliac crest just lateral to the triangle of Petit can be made. After development of the retroperitoneal space, port placement can be achieved by first placing the lateral robotic port 7 to 8 cm superolateral to the camera port. The assistant port is placed in the anterior axillary line cephalad to the ASIS, which should be 7 to 8 cm caudal to the medial port. A fourth robotic arm may be placed 7 to 8 cm beyond and 2 cm below the medial robotic port. 4
Retroperitoneal template for the da Vinci Xi
When transitioning to the da Vinci Xi, one can use the similar Si template with a few modifications (Fig. 3). The currently available balloon port is 10 mm and can accommodate the 8 mm camera. Alternatively, the 8 mm camera port can be piggybacked through a 12 mm metal trocar. If only a 12 mm plastic trocar is available and the surgeon attempts to place the 8 mm camera trocar trough, the potential for capacitive coupling exists where electrical energy can cause charge buildup and discharge. Finally, if the trocar is not designed for 8 mm ports, an 8 mm robotic port can be placed and a purse-string suture can be applied to avoid the loss of pneumoperitoneum.
For the Si, the robot is docked from the ipsilateral shoulder. When using daVinci Xi, it is helpful to swivel robotic arms on an overhead boom as needed, allowing the robot to be docked both perpendicular and parallel to the bed.
Pyeloplasty
Port placement for pyeloplasty differs from other renal surgery secondary to reconstructive vs oncologic nature of the procedure. Therefore, care is taken to minimize the number and size of the ports utilized. In addition, port templates are modified based on the anatomy and size of the patient and usually placed in midline or just lateral to rectus muscle.
Transperitoneal template for the da Vinci Si
For younger children, patients are positioned in the full flank position, typically without flexion of the operating room table. Veress needle insufflation is obtained and pneumoperitoneum is established to a pressure of 14 cm H2O. A 12 mm camera port is placed, above the umbilicus, along the lateral boarder of the rectus sheath. The robotic working trocars are placed about 6 to 8 cm cranial and caudal to the camera in the midline or along the lateral boarder of the rectus sheath as the body anatomy permits. A 5 mm assistant port is placed in the midline (Fig. 4). This template is ideal for most patients with a large dilated renal pelvis. For patients with a small renal pelvis or those with high insertion where the working space will be more cranial, the axis of the ports can be rotated around the camera port to point toward the surgical field. 5
Left-sided pyeloplasty with da Vinci Si/Xi for young children. Right-sided port placement would be a mirror image. For small children can use 8.5 mm camera and 8 mm working instruments. This template is ideal for children with a large renal pelvis. For children with a small pelvis, the ports can be shifted cranial in the midline or can be rotated with an axis looking toward the upper quadrant.
Usually one should avoid placing a fourth port, however, if necessary, a fourth working port can be placed just medial to ASIS just lateral to the rectus sheath. We typically try to avoid using this port for better cosmetic appearance and lower cost. For younger patients, the camera port may be placed just inferior to the umbilicus and the assistant port may be negated, which passed through a robotic trocar to enhance cosmesis and minimize scar formation. 5
Transperitoneal template for the da Vinci Xi
The port template for the da Vinci Xi is similar to that of the Si except the camera port will be a standard 8 mm robotic port (Fig. 4). For the Xi platform, at this time there are no smaller 5 mm working instruments so the 8 mm ports will be necessary for all cases.
Combined Upper and Lower Urinary Tract
Nephroureterectomy
Nephroureterectomy can be a complex procedure using the robotic approach since port placement is critical to be able to access both the upper and lower urinary tracts. We have previously described our technique for port placement for nephrouretectomy using the Si 6 and Xi 7 robot without the need to undock or move the patient side cart. Alternative to the single-dock technique, surgeons may prefer to undock and reposition the patient in steep Trendelenburg, especially if there is difficulty in reaching the distal ureteral cuff.
Transperitoneal template for the da Vinci Si
Patient positioning is similar to renal surgery aforementioned. Port placement can be seen in Figure 5. The 12 mm camera port is placed just lateral to the ipsilateral rectus sheath and just cranial to the umbilicus. Three additional 8 mm robotic ports are placed: (1) 8 cm cranial to the camera and lateral to the rectus sheath, (2) midline about 6 cm caudal to the umbilicus, and (3) 2 cm cranial to the ASIS. A 12 mm assistant port can be placed in the midline between the camera port and the cranial working port. The robot is docked at a 90° angle over the patient's back. For the nephrectomy portion, the cranial port is the left arm, the caudal port is the right arm, and the lateral port is the fourth arm. During the bladder cuff portion, the arms are switched with the caudal port as the right arm, the lateral port as the left arm, and the cranial port as the fourth arm. This port template allows seamless transition from upper to lower tract surgery without de-docking and moving the patient side cart. 6,8,9
Left-sided nephroureterectomy using the da Vinci Si. Right-sided ports would be a mirror image.
Transperitoneal template for the da Vinci Xi
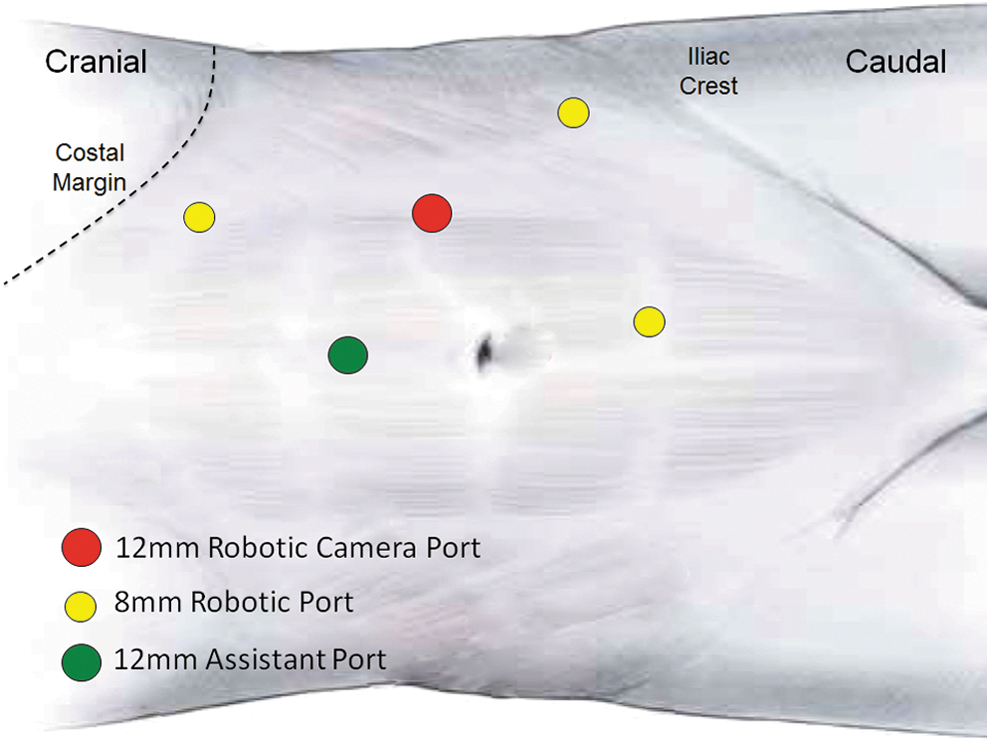
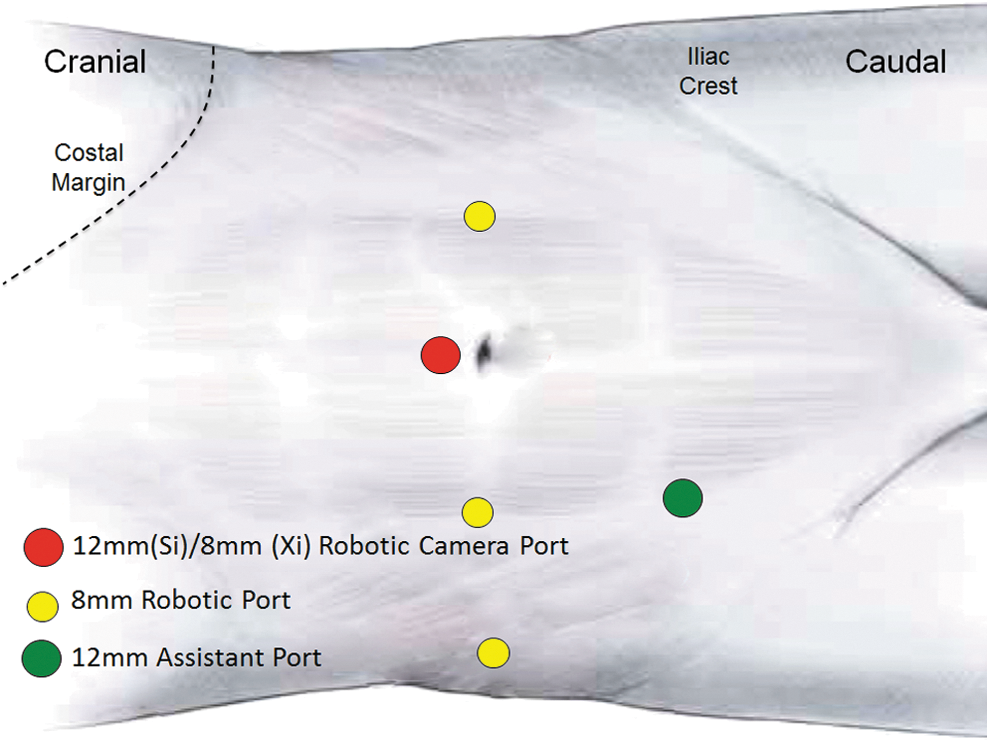
Port template for the Xi can either be arranged in a linear manner along the rectus sheath (Fig. 2) or the fourth port may be placed more medially (Fig. 6).
Left-sided nephroureterectomy using the da Vinci Xi, with the inferior port placed more medial. Right-sided ports would be a mirror image.
The camera port is placed along the rectus sheath just cranial to the umbilicus. Three additional ports are placed along the sheath with one about 6 to 7 cm cranial to the camera, one about 6 to 7 cm caudal to the camera, and one about 6 to 7 cm caudal to the third port. A 12 mm assistant port is placed in the midline between the cranial port and the camera port. The robot is docked at a 90° angle over the back of the patient. During the nephrectomy portion of the procedure, the targeting feature is used to direct the arms of the robot toward the renal hilum. Once this portion is complete, the arms are disconnected, and the robot is retargeted toward the bladder cuff. This allows the robotic boom to rotate without moving the patient side cart. In addition, the camera “hops” from the port just cranial to the umbilicus to the port just caudal to the umbilicus. 7
Lower Urinary Tract
Radical/simple prostatectomy
Transperitoneal template for the da Vinci Si/Xi
Initial description of port placement for radical prostatectomy continues to remain the basic foundation. 1,10 Port placement for both the Si and Xi are similar as shown in Figure 7. Patients are positioned in dorsal lithotomy with arms tucked ensuring adequate padding of all extremities to avoid potential compartment syndrome and/or neuropraxia. Moreover, the patient is adequately secured to the table and placed in steep Trendelenburg. In both templates, the camera port is placed either below (shown) or above the umbilicus. An assistant 12 mm port is placed 2 cm cranial to the right ASIS. Alternatively, the assistant port can be placed on the left side, should one want to have two robotic arms on the right. Working 8 mm ports are placed about 6 to 8 cm lateral on each side of the camera just lateral to the rectus sheath. The third working port is placed about 3 to 4 cm cranial and 2 cm cranial to the left ASIS. A 5 mm assistant port is placed about 2 cm cranial to umbilicus between the camera and the right working port. Traditionally, the patient is placed in the dorsal lithotomy position, and the robot is docked between the legs of the patient.
Prostatectomy using the da Vinci Si/Xi.
Although port placement is similar between the Si and Xi, the robot can be docked differently among the different robotic platforms. For the Xi, the patient can be kept in supine position with the robot docked at a 45° angle. Although side-docking in the Si can be achieved, 11 the ease with which the Xi can achieve this feat does not go unnoticed.
Extraperitoneal template for the Si/Xi
Robotic prostatectomy via an extraperitoneal approach has proven efficacious in several case series. 12 In this approach, the peritoneal layer acts as a natural retractor, negating any bowel-related complications. Moreover, steep Trendelenburg is not needed. Joseph and colleagues describes port placement for this approach involving a 2.5 cm periumbilical incision, which is dissected down to the posterior rectus sheath, at which point a 0° lens is inserted into an OMS-XB2 Extra View™ balloon dilator. Under direct visualization, the space is developed and the dilator can be replaced for the camera port. Assistant ports are placed 5 cm medial and cephalad to the ASIS, bilaterally. Two 8 mm robotic ports can be placed along the pararectal lines ∼8 to 10 cm caudal to the umbilicus.
Perineal template
Patients are placed in exaggerated lithotomy position and 15° Trendelenburg. A 3 cm perineal incision in the central tendon is incised. After development of the subcutaneous adipose tissue, a gel port (GelPOINT Mini; Applied Medical, Rancho Santa Margarita, CA) is placed. The camera port is placed anteriorly, with the robotic working ports (8 mm) placed posterolaterally and the assistant port at the 6 o'clock position. The robot is docked over the patient's head. 13
Radial cystectomy
Cystectomy with subsequent urinary diversion is a technically challenging operation, often completed in an open manner; however, recent literature is challenging the notion of this maximally invasive option and instead, invoking intracorporeal diversion as a superior alternative. 14 –16 The first series of robotic radical cystectomy was described in 17 patients with excellent oncologic outcomes. 17
The patient is positioned similarly to radical/simple prostatectomy aforementioned. However, before proceeding to intracorporeal diversion, Trendelenburg should be reduced to 10 to 15°. Alternatively, the patient can be left supine and the robot can be side-docked to avoid prolonged lithotomy position.
Template for the da Vinci Si
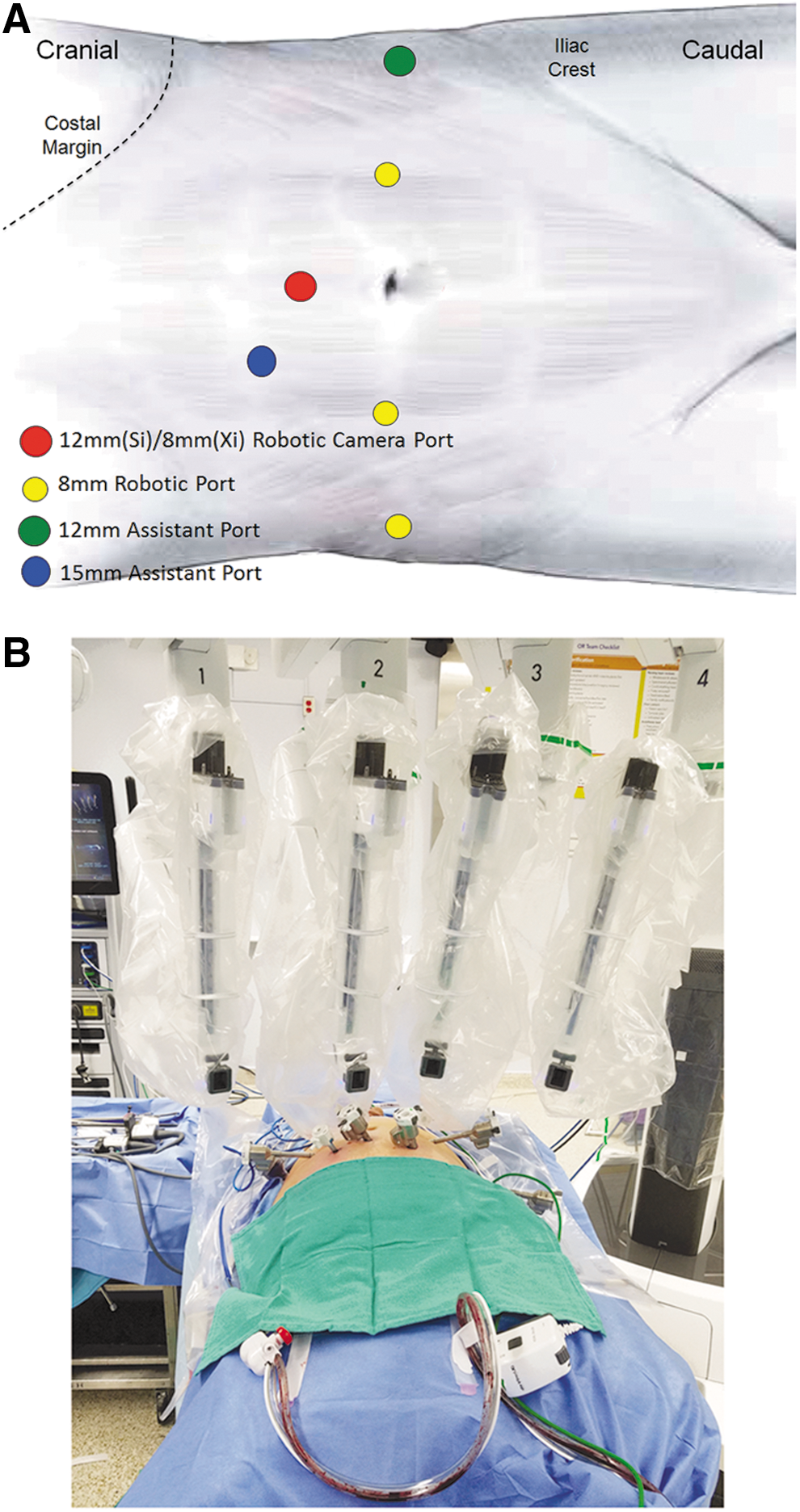
An Endopath® Xcel™ 12 mm bariatric trocar is placed 5 cm above the umbilicus with two robotic ports on each side of the camera port ∼7 to 10 cm lateral and above the level of the umbilicus. The additional robotic port is placed in the right lower quadrant of the abdomen ∼7 to 10 cm lateral to the right-sided robotic port and 5 to 7 cm superior to the iliac crest (Fig. 8A). A 12 mm assistant trocar is then inserted on the left side 5 to 7 cm superior to the iliac crest. The use of the fourth arm on the right and 12 mm assistant port on the left facilitates bowel manipulation by avoiding acute-angle stapling. A second assistant port can be placed through the premarked stoma site when an ileal conduit is desired or can placed on the left side, allowing the assistant to have control on both ports from one side. Having an additional 12 mm assistant port close to the midline greatly simplifies pedicle stapling during extirpative cystectomy. The robot is docked similarly to prostatectomy aforementioned.
We typically utilize three instruments: Hot Shears™ in the right robotic arm, PK® dissecting forceps in the left robotic arm, and Cadiere forceps in the third robotic arm. Robotic-assisted radical cystectomy (RARC) can be performed entirely with these three instruments to help cut down on operative costs. However, for intracorporeal orthotopic neobladder, two needle drivers inclusive of one suture cut are utilized. The 0° camera lens can be used for a majority of the dissection, but the 30° down lens is helpful for dissecting deep within the pelvis and for the extended pelvic lymph node. The 30° up lens may be helpful for dissecting behind the prostate, retro-apical dissection for providing additional urethral length, and for dropping the bladder.
Template for the da Vinci Xi
As mentioned earlier a six-port transperitoneal approach is used and all ports are placed about 5 cm cephalad to the umbilicus. On the Xi system, the 12 mm camera port is replaced by a da Vinci 8 mm universal camera-robotic port (Fig. 8a). With the Xi robotic platform, side-docking can be achieved with relative ease. The authors' current preference is a hybrid position, where the cystectomy portion is performed in dorsal lithotomy with steep Trendelenburg with the robot positioned between the legs and the intracorporeal diversion performed with the robot side-docked in mild Trendelenburg. However, prolonged positioning in steep Trendelenburg may have potential for ocular, pulmonary, musculofascial, and neurologic 18 complications. Especially in these patients, the authors prefer side-docking entirely (Fig. 8b). With integrated table motion (TruSystem™ OR Table; Trumpf Medical), the authors have found simultaneous position changes to be effortless without the need to re-dock.
When performing intracorporeal urinary diversion, some centers utilize a gel port for the camera, which can also aid as the specimen extraction site as well as manipulation of bowel in creation of a urinary reservoir extracorporeally, which can then be placed back into the pelvis with the robot re-docked to complete ileo-urethral anastomosis. When performing ileal conduit urinary diversion intracorporeally, the prior-marked stoma site can be utilized as an additional 12 or 15 mm port to facilitate a stapling device.
Retroperitoneal Lymph Node Dissection
Template for the da Vinci Si and Xi platforms
Retroperitoneal lymph node dissection was initially performed for diagnostic purposes in the postchemotherapy setting but has since evolved and is now being performed for therapeutic purposes. The port template for retroperitoneal lymph node dissection (RPLND) involves placing ports in a straight line angled toward the side of dissection with a 12 mm assistant port on the contralateral side. 19
At our institution, the patient is placed in the supine position. Once pneumoperitoneum is established, the camera port is placed just cranial to the umbilicus (12 mm for Si; 8 mm for Xi). Two working ports are placed lateral to the camera on either side of the rectus sheath 6 to 8 cm from the camera port. A third working port is placed on the left side in line with the other working ports about 3 cm cranial to the ASIS. A 12 mm assistant port is placed just lateral to the rectus sheath about 6 cm caudal to the camera port. If necessary, an additional 5 mm assistant port can be placed contralateral to the 12 mm assistant port just lateral to the rectus sheath. The robot is typically docked from the side opposite to the assistant port (Fig. 9). This port template allows access between the common iliac and renal arteries and can be used for unilateral and bilateral extended node dissection.
Retroperitoneal lymph node dissection using the da Vinic Si/Xi. A second 5 mm assistant port can be placed, if necessary, contralateral to the 12 mm assistant port just lateral to the rectus sheath.
Female Pelvic Surgery (Sacrocolpopexy, Vesico-Vaginal Fistula Repair, Pelvic Lymph Node Dissection, Hysterectomy)
The patient is positioned similarly to prostate/bladder surgery with dorsal lithotomy, arms tucked, and Trendelenburg. A standard periumbilical incision can be made for placement of the 12 mm camera port, but occasionally it may be placed supraumbilically as an alternate site. Positioning of the ports for robotic sacrocolpopexy is similar to the robotic prostatectomy; however, ports should be placed slightly more cephalad to allow for maximal access to the sacral promontory but not compromising access to the deep pelvis. We routinely use a fourth arm placed ∼3 to 4 cm cephalad to the iliac crest on the left lateral sidewall.
Special Considerations
Oftentimes, patients have significant comorbidities or differing body types necessitating shifting from traditional port placement. With the rising obesity epidemic, the urologic robotic surgeon should be adept at modifying port placement to accommodate for different patient subtypes. Below are special considerations for distinct patient populations.
Obese patients
Obesity cannot only pose a technical challenge for the surgeon, but can also affect oncologic and functional outcomes in robotic urologic surgery. 20 For upper tract surgery, the template should be shifted laterally. 21 The assistant 12 mm port may be placed more laterally than the traditional supraumbilical location. In lower tract surgery, traditional port placement is typically adequate but the need for special bariatric trocars becomes paramount, especially for body mass index (BMI) >40. Patients may be positioned supine with the robot side-docked in an effort to reduce the risk of rhabdomyolysis in this patient population.
Pediatric patients or BMI <20
For upper tract surgery in pediatric patients, we typically utilize a three-arm technique for pyeloplasty 5 with or without an assistant port. For patients with low BMI, the assistant port, if used, may need to be placed on the contralateral side. Lower tract surgery is typically similar and mentioned above.
Renal transplant/inflatable penile prosthesis
Patients with prior renal transplant and with prior placement of inflatable penile prosthesis possess unique challenges with heightened care as to not injure the renal graft or prosthesis. For patients with a single kidney allograft or inflatable penile prosthesis, the patient should be tilted toward the ipsilateral allograft/reservoir, elevating the contralateral side with the camera port placed 5 cm above the umbilicus on the contralateral side of the allograft/reservoir. Only one robotic arm should be placed on the ipsilateral side, with two robotic ports on the contralateral side. A single assistant port can be placed after insufflation to determine the ideal location. For patients with dual renal allografts or a single allograft and a contralateral prosthetic reservoir, the patient should be kept in supine position with a camera port placed above the umbilicus. Two robotic arms should be placed 5 cm lateral to the central camera port, with the third robotic arm and assistant port planned after initial insufflation, visualization, and dissection. 22
Single-site surgery
For patients concerned with surgical scars, robot-assisted laparoscopic single-site surgery provides the urologist the ability to perform urologic surgery with the use of minimal incisions and scars. Single-site surgery in various upper and lower tracts has been reported. 22 For upper tract procedures, a 2 to 5 cm periumbilical incision can be made to facilitate the insertion of the gel port. The camera port should be placed medially, with two robotic working ports placed at the lateral most position. Assistant ports may be placed between the camera and robotic working ports. 23
Closure of port sites
Given the increased utilization of minimally invasive surgery, importance should be placed on using proper closing techniques for port sites to prevent or minimize the occurrence of a port-site hernia. We routinely close fascia for all port sites >8 mm with selective closure of 8 mm robotic working ports. Closure can be traditionally performed via a hand-sewn method or utilization of various port closure devices such as Carter-Thomason®, Weck EFx®, or CrossBow™ systems. When using one of these devices, port closure can be done under visual guidance to minimize risk of bowel entrapment or bleeding. Selective closure of 8 mm robotic working ports should be indicated for patients with excessive traction/manipulation of the robotic arm or those with additional risk factors for hernia formation. The skin layer of the extraction site and all other port sites are then closed with subcutaneous 4–0 monocryl suture and skin adhesive or alternatively dressed.
Conclusion
Placement of ports is critical to the effective completion of most robotic cases. Modifications to the working template can help ease the surgeon's transition from the da Vinci Si to the da Vinci Xi robotic platform. The above port templates represent the authors' preferred strategy when performing robotic urologic surgery. Utilization of these templates can facilitate surgeons treating a wide variety of urologic conditions.
Footnotes
Author Disclosure Statement
No competing financial interests exist.