
Abstract
Introduction and Objectives:
In recent years, there has been a shift to minimally invasive partial nephrectomy (MIPN) with the dissemination of robot-assisted technology. However, contemporary data on the comparative morbidity of open partial nephrectomy (OPN) and MIPN are lacking. We, therefore, evaluated the perioperative morbidity of OPN and MIPN using a contemporary national cohort.
Methods:
We identified 13,658 patients aged 18 to 89 who underwent PN from 2010 to 2015 in the National Surgical Quality Improvement Program (NSQIP) database, of whom 9018 (66.0%) underwent MIPN. The associations of MIPN with 30-day morbidity were evaluated using logistic regression, adjusted for patient features.
Results:
Median age at surgery was 60 (interquartile range [IQR] 51, 68) years. Overall, 30-day complications occurred in 6.7% of patients. Compared with OPN, MIPN was associated with lower rates of 30-day complications (4.9% vs 10.1%, p < 0.0001), perioperative blood transfusion (3.8% vs 12.5%, p < 0.0001), prolonged hospitalization (5.6% vs 23.4%, p < 0.0001), readmission (4.4% vs 7.8%, p < 0.0001), reoperation (1.8% vs 3.2%, p < 0.0001), and 30-day mortality (0.3% vs 0.6%, p = 0.001). On multivariable analysis, MIPN was independently associated with a reduced risk of 30-day complications (odds ratio [OR] 0.46, p < 0.0001), perioperative blood transfusion (OR 0.27, p < 0.0001), prolonged hospitalization (OR 0.19, p < 0.0001), readmission (OR 0.59, p < 0.0001), and reoperation (OR 0.57, p < 0.0001). Postoperative complications occurred predominantly early after surgery, whereas hospital readmissions and reoperation occurred at a consistent rate.
Conclusions:
In this contemporary national cohort, MIPN was independently associated with reduced rates of 30-day complications, perioperative blood transfusion, prolonged hospitalization, hospital readmission, and reoperation, compared with OPN.
Introduction
P
However, contemporary data assessing the perioperative morbidity of OPN and MIPN are limited. Early reports describing improved perioperative outcomes with MIPN were largely limited to single institution cohorts with small sample sizes. 4 –8 Subsequent studies reporting on population-based cohorts were performed before the dissemination of robot-assisted techniques for MIPN, and may not reflect contemporary practice patterns or patient poulations. 9 –11
In this study, we, therefore, examined the perioperative morbidity and mortality of OPN and MIPN in a contemporary, population-based cohort using the National Surgical Quality Improvement Program (NSQIP). We hypothesized that MIPN is associated with decreased perioperative morbidity compared with OPN, and sought to both comprehensively characterize its perioperative morbidity profile as well as the timing of postoperative complications, hospital readmission, and reoperation.
Methods
Data source and study population
The American College of Surgeons NSQIP captures perioperative clinical data, including 30-day postoperative complications and mortality, for patients undergoing major surgical procedures at participating institutions. Data are abstracted by trained clinical reviewers, and the program employs various quality assurance measures to ensure data accuracy. 16
After obtaining exempt status from our Institutional Review Board, we identified adults aged 18 to 89 years who underwent MIPN or OPN in the NSQIP from 2010 to 2015 using Current Procedural Terminology (CPT) codes 50543 (MIPN) and 50240 (OPN). Patients aged 90 years or older were excluded as they are collapsed into a single age category in the NSQIP.
Patient characteristics
Perioperative variables recorded included age at surgery, year of surgery, surgical approach (OPN, MIPN), race, sex, American Society of Anesthesiology (ASA) class, smoking status (smoker within last year, former/never), chronic steroid use, functional status (independent, partially/totally dependent), discharge destination (home, rehab/skilled nursing facility, death), operative time, and presence of the following comorbidities: diabetes, chronic obstructive pulmonary disease, congestive heart failure, hypertension requiring medical treatment, renal failure or dialysis, and bleeding disorder.
Outcomes
The following postoperative endpoints were recorded as part of NSQIP: 30-day complications, perioperative blood transfusion within 72 hours of surgery, length of stay (LOS), 30-day readmission, 30-day reoperation, and 30-day mortality. Readmission and reoperation data were available from 2012 to 2015, and these analyses were accordingly restricted to these study years. Prolonged hospitalization (pLOS) was defined as a hospitalization duration greater than the 90th percentile for the overall cohort. Postoperative complications were further categorized as cardiac, thromboembolic (deep venous thrombosis [DVT], pulmonary embolism [PE]), infectious (urinary tract infection [UTI], sepsis), respiratory, renal, neurologic, and surgical site infection/wound infection.
Statistical analyses
Baseline characteristics were summarized using medians/interquartile ranges (IQR) and frequency counts/percentages, and compared across age categories using ANOVA and Pearson's chi-square test, respectively. Postoperative outcomes were summarized using frequency counts/percentages across age categories using Pearson's chi-square test.
Multivariable logistic regression was used to evaluate the associations of surgical approach with perioperative endpoints. Effect estimates were summarized using odds ratios (OR) with 95% confidence intervals (95% CI). Models were adjusted for age at surgery (continuous), sex, year of surgery, race (white, black, other), ASA class (1–2, 3, 4–5), smoking status (smoker within last year, former/never), functional status, steroid use, operative time, and presence of the following comorbidities: diabetes, chronic obstructive pulmonary disease, congestive heart failure, hypertension, renal failure, and bleeding disorder. Observations with missing data were dropped, excluding race, which was assigned to an “Unknown” category.
We conducted an exploratory analysis to evaluate the timing of postoperative complications, hospital readmission, and reoperation. Survival, free of any complication, free of each specific complication category, free of hospital readmission, or free of reoperation, was evaluated separately for each endpoint using the Kaplan–Meier method and compared across surgical approach using the log-rank test.
Statistical analyses were performed using R version 3.3.2 (R Foundation for Statistical Computing, Vienna, Austria). All tests were two-sided, and p-values <0.05 were considered to be statistically significant.
Results
A total of 13,658 patients underwent PN, including 4,640 (34%) patients who underwent OPN and 9,018 (66%) patients who underwent MIPN. Baseline demographics, stratified by surgical approach, are summarized in Table 1. Median age at surgery was 60 (IQR 51, 68) years, and 59% of patients were male. There were statistically significant differences in several baseline characteristics between groups, including lower ASA class and decreased prevalence of diabetes, chronic obstructive pulmonary disease, hypertension, and renal failure among patients undergoing MIPN (Table 1). Median operative time was slightly longer among patients undergoing MIPN compared with OPN (183 vs 174 minutes; p < 0.0001), and the rate of discharge to a skilled nursing facility was higher in the OPN group (3.3% vs 1.4%; p < 0.0001).
Values represent n (%) or median (IQR).
Pearson's chi-square unless otherwise noted.
Variable added in 2011, values represent 2011–2015.
Wilcoxon rank-sum test.
Pearson's chi-square test with Yates' continuity correction.
ASA = American Society of Anesthesiology; CHF = congestive heart failure; COPD = chronic obstructive pulmonary disease; IQR = interquartile range; MIPN = minimally invasive partial nephrectomy; OPN = open partial nephrectomy; SNF = skilled nursing facility.
Perioperative outcomes are summarized in Table 2. Overall, 30-day complications occurred in 6.7% of patients. The most common complication categories were infectious (2.3%), surgical site infection/wound (1.7%), and respiratory (1.7%). Compared with OPN, MIPN was associated with significantly lower rates of any 30-day complication (4.9% vs 10.1%; p < 0.0001), with statistically significantly lower rates of each complication category, except pulmonary embolism, suggesting that there is a global decrease in morbidity rather than a particular type of complication. Furthermore, compared with patients undergoing OPN, those who underwent MIPN had statistically significantly lower rates of perioperative blood transfusion (3.8% vs 12.5%; p < 0.0001), prolonged hospitalization (5.6% vs 23.4%; p < 0.0001), hospital readmission (4.4% vs 7.8%; p < 0.0001), reoperation (1.8% vs 3.2%; p < 0.0001), and 30-day mortality (0.3% vs 0.6%, p = 0.001).
Values represent %.
Pearson's chi-square test with Yates' continuity correction.
Analysis restricted to 2012–2015.
DVT = deep venous thrombosis; PE = pulmonary embolism; SSI = surgical site infection.
We further evaluated the associations of surgical approach with perioperative outcomes in multivariable analyses (Table 3). After adjusting for patient features, MIPN remained independently associated with reduced risks of 30-day complications (OR 0.46; p < 0.0001), perioperative blood transfusion (OR 0.27; p < 0.0001), prolonged hospitalization (OR 0.19, p < 0.0001), readmission (OR 0.59; p < 0.0001), and reoperation (OR 0.57; p < 0.0001). MIPN was associated with a reduced risk of 30-day mortality that did not reach statistical significance (OR 0.62; p = 0.10).
Analysis restricted to 2012–2015.
CI = confidence interval; OR = odds ratio.
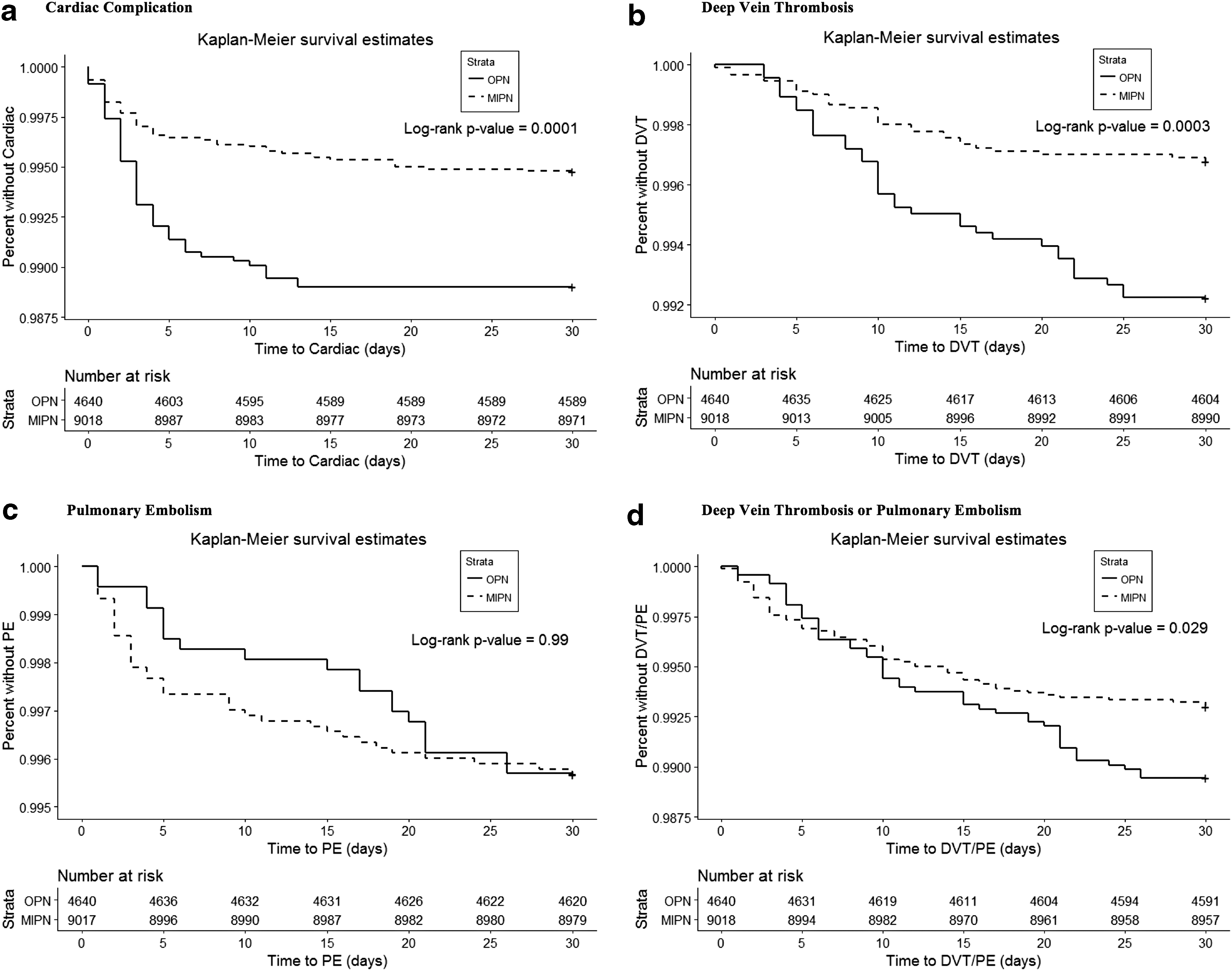
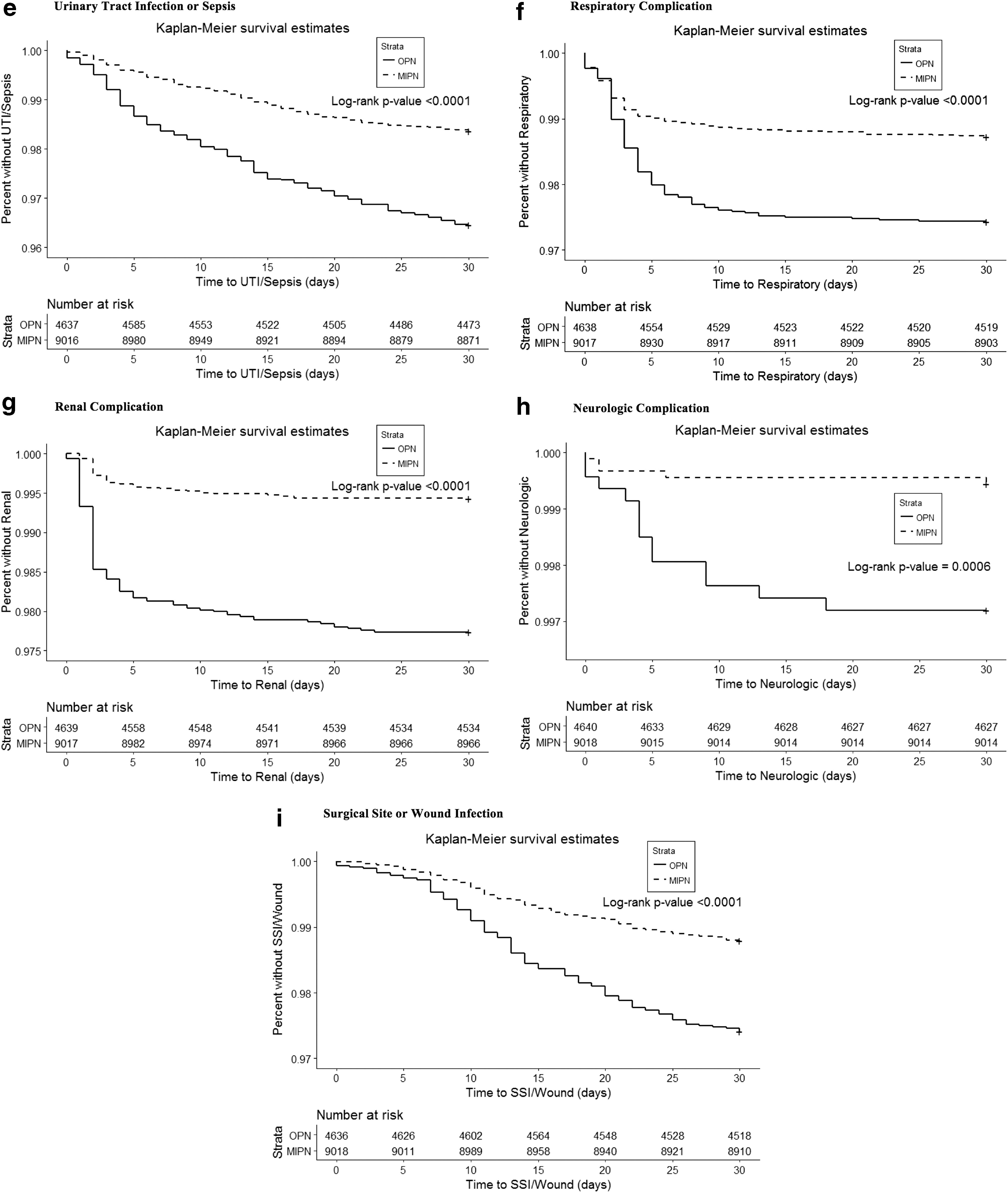
As an exploratory analysis, we evaluated the timing of post-operative complications, hospital readmission, and reoperation, stratified by surgical approach. Reinforcing the bivariate analyses in Table 2, MIPN was associated with improved survival free of any complication (p < 0.0001), cardiac complications (p < 0.0001), DVT/PE (p = 0.03), UTI/sepsis (p < 0.0001), respiratory complications (p < 0.0001), renal failure (p < 0.0001), neurologic complications (p = 0.0006), and surgical site infection (SSI)/sound complications (p < 0.0001) (Figs. 1 and 2a–i). More importantly, Kaplan–Meier figures illustrate that the occurrence of 30-day complications is predominantly early—that is, within the first 10 days postoperatively (Fig. 1). Similarly, predominantly early timing was apparent for cardiac, respiratory, renal, and neurologic complications, whereas thromboembolic complications, UTI/sepsis, and SSI/wound complications occurred consistently throughout the first 30 days after surgery (Fig. 2a–i). Hospital readmissions and reoperation likewise appeared to occur consistently throughout the 30-day postoperative period (Figs. 3 and 4).

Survival free of any complication, stratified by surgical approach.
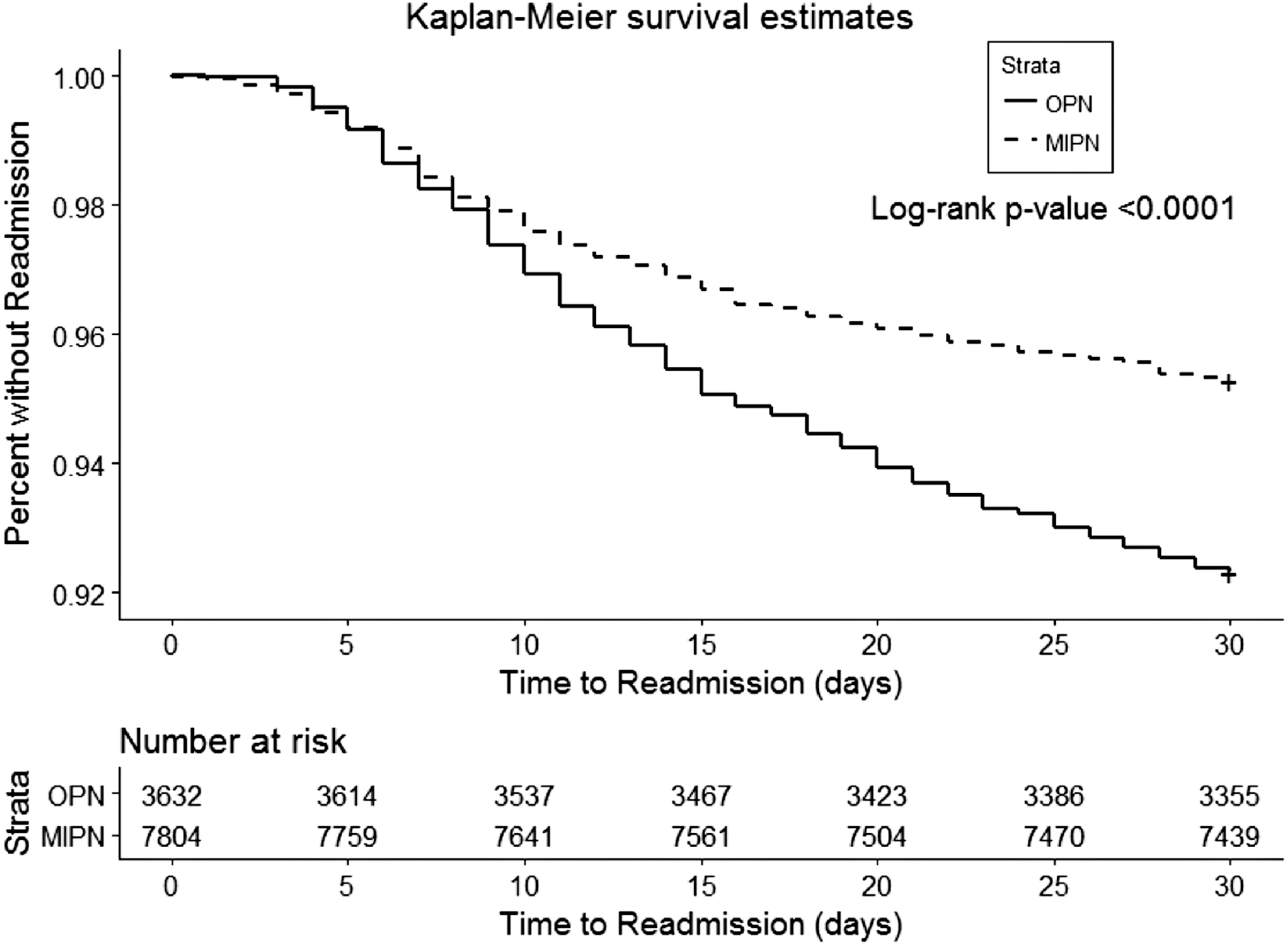
Survival free of hospital readmission, stratified by surgical approach.
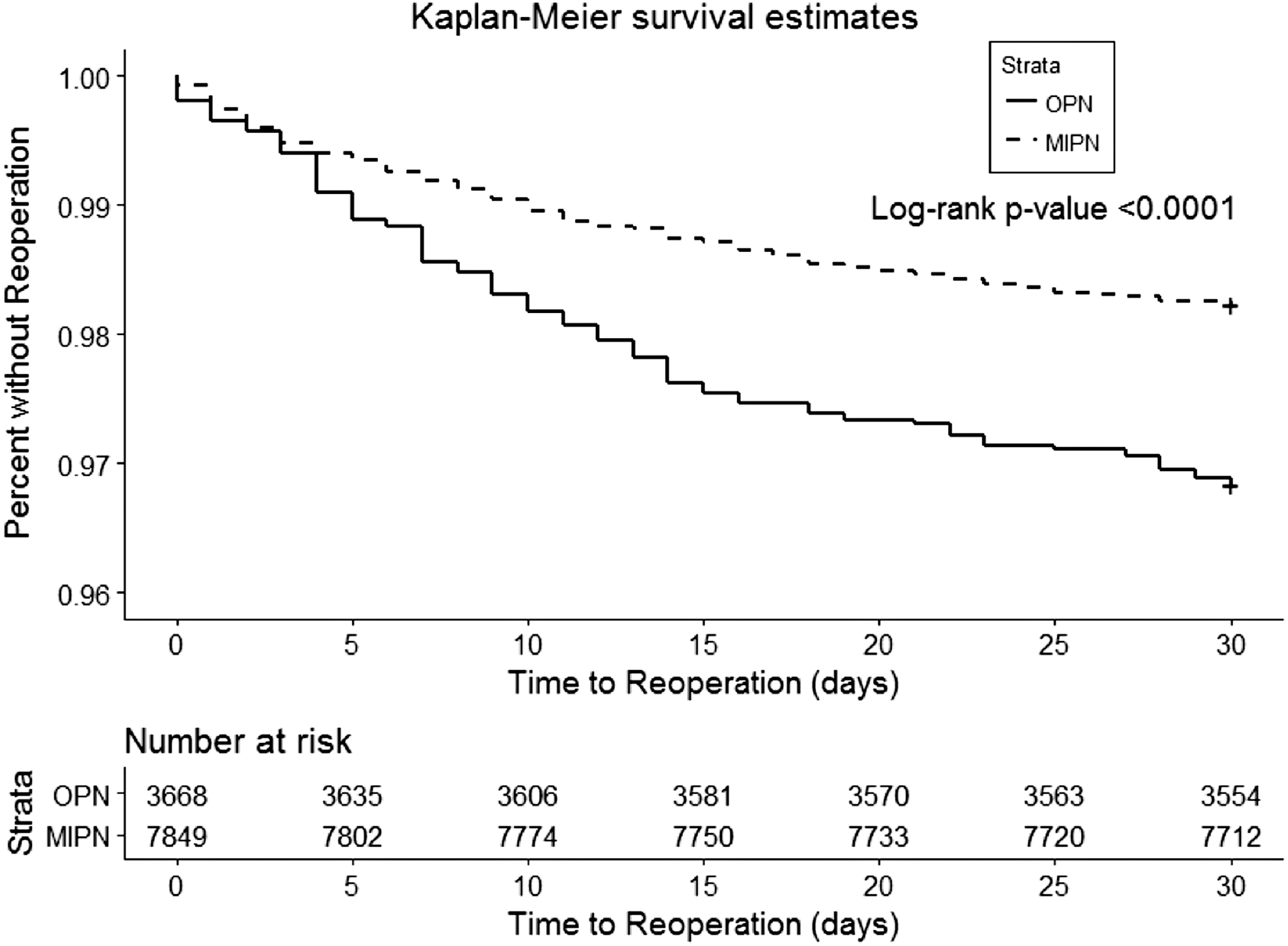
Survival free of reoperation, stratified by surgical approach.
Discussion
In this study, we utilized a large, national cohort to evaluate outcomes by surgical approach for PN. We observed that MIPN was associated with decreased risks of 30-day complications, perioperative blood transfusion, prolonged hospitalization, hospital readmission, and reoperation, even after adjusting for patient features. MIPN was associated with a similar reduction in 30-day mortality in multivariable analyses, although this did not reach statistical significance. Moreover, we characterized the timing of postoperative complications, readmissions, and reoperation, with implications for postdischarge follow-up and interventions targeted at reducing morbidity. While most complication categories occurred early, rates of hospital readmission and reoperation occurred consistently throughout the 30-day postoperative period, likely reflecting the occurrence of other complication categories that may warrant readmission and reintervention such as SSI/wound complications. These observations highlight the importance of continued vigilance and patient monitoring throughout the postdischarge period.
There is a paucity of data comparing perioperative outcomes for MIPN and OPN in contemporary clinical practice. Utilization of MIPN has increased, in large part due to the dissemination of robotic PN (RPN). Indeed, the utilization of robot-assisted techniques in renal surgery has increased from less than 2% of renal surgeries in 2006 performed with robotic assistance to almost 50% of renal surgeries in 2012 performed using the robotic platform. 12 Furthermore, there has been a shift away from laparoscopic PN (LPN), with only 7% to 9% of PN performed using LPN. 12
While several studies have compared perioperative outcomes of MIPN to those of OPN, most were performed before the widespread adoption of MIPN. Early single-institutional series with relatively small sample sizes reported that MIPN was associated with increased operative time when compared with OPN, but decreased blood loss, lower opioid requirements, and shorter hospital stays. 4 –8 Notably, in these studies, MIPN was not associated with a statistically significant difference in complication rates compared with OPN. In a larger multicenter study involving 1800 patients undergoing PN, Gill and colleagues also reported decreased LOS and intraoperative blood loss, but an increased risk of postoperative complications with LPN. 17 Our observations of reduced rates of perioperative morbidity with MIPN contrast from such early series, and may be explained by the use of predominantly pure laparoscopic rather than robot-assisted approaches in such series. In fact, more recent multi-institutional studies comparing RPN to OPN have found OPN to be associated with more than twice the risk of postoperative complications compared with OPN. 18 –20
Early population-based comparisons of MIPN and OPN were performed using surveillance, epidemiology, and end results program (SEER)-Medicare and Nationwide Inpatient Sample (NIS) data with conflicting findings. 10,11 One study examined SEER-Medicare data from 2000 to 2007, and observed decreased pLOS for LPN compared with OPN. 11 However, there were no statistically significant differences in postoperative complications or hospital readmission. Conversely, in another study that examined NIS data from 1998 to 2007, the authors reported that LPN was associated with decreased rates of perioperative complications, blood transfusion, and pLOS. 10 It is interesting that these population-based studies provided disparate findings regarding the perioperative morbidity of MIPN depending on the dataset used. This may be related to differences in ascertainment of complications using administrative claims data, or the lack of postdischarge data in the NIS, which limits captured complications to the index hospitalization. Alternatively, this may be attributed to the older study periods in these studies, which was early in the adoption period of MIPN as reflected in lower utilization rates of MIPN (28% and 6%, respectively).
Later population-based studies have supported a reduction in perioperative morbidity with minimally invasive renal surgery, suggesting improvements in perioperative endpoints with greater experience with minimally invasive techniques and a shift from LPN to RPN. 9,21 –23 In studies comparing minimally invasive and open renal surgery in NSQIP from 2005 to 2012, it was reported that minimally invasive renal surgery was associated with decreased 30-day morbidity, mortality, and readmission rates. 21 –23 Interestingly, the earliest of these studies observed increased utilization of MIPN over the period studied, with MIPN utilization increasing from 0% before 2007 to over 50% of PN by 2011. 21 In another study using the NIS from 2008 to 2010 comparing OPN, LPN, and RPN, the authors found that MIPN (LPN or RPN) was associated with lower risks of blood transfusion, postoperative complications, and pLOS. 9
The present study represents the most recent population-based data comparing the perioperative outcomes following MIPN and OPN. Indeed, two-thirds of PN in this study were performed using a minimally invasive approach. Although NSQIP does not distinguish the use of LPN from RPN, the present study reflects contemporary clinical practice in the era following dissemination of robot-assisted renal surgery.
In this study, we also examined the timing of postoperative complications (including postdischarge complications), hospital readmission, and reoperation following PN. The observation that the majority of postoperative complications occur early, likely during the index hospitalization, suggests that early complications represent events closely linked with the operative procedure. Perhaps more importantly, particularly in the current emphasis on value-based healthcare, hospital readmissions and reoperation occurred at a consistent rate throughout the first 30-days postoperatively. Accordingly, postdischarge interventions targeting reductions in these endpoints, such as postoperative outpatient follow-up, should be considered with this timing in mind.
Data examining the timing of postoperative complications following nephrectomy are sparse. In one study that investigated the timing of postoperative complications following nephrectomy (including both PN and RN), the authors reported that major complications were most likely to occur early and before discharge, whereas minor complications were more likely to occur later after discharge. 24 Notably, that study did not separately examine PN, which is associated with unique complications, such urinary leak and pseudoaneurysm/arteriovenous fistula formation that may require readmission or reintervention. Indeed, in the current study, we observed that while some complication categories occurred early in the postoperative period, those likely to require readmission or reintervention, such as thromboembolic complications, UTI/sepsis, and SSI/wound complications, tended to occur throughout the 30-day postoperative period. This may explain the steady rate of hospital readmission and reoperation during the postoperative period.
The present study benefited from a large sample size, national cohort of patients from institutions participating in NSQIP, and multiple surgeons performing surgery. Accordingly, these observations may hold greater external validity for the “average” patient undergoing PN than the experience of high-volume referral institutions. In addition, NSQIP data are clinically abstracted by trained personnel in a standardized fashion and, therefore, may more accurately reflect perioperative outcomes than administrative data sources.
This study has several limitations. Most importantly, we were unable to adjust for a number of clinicopathological features that are not available in the NSQIP dataset, such as hospital or surgeon case volume, patient socioeconomic status, and preoperative functional assessment. Furthermore, NSQIP does not capture preoperative imaging or pathological features, which are necessary to adjust for anatomic complexity and case mix. This may serve as a potential source of bias as anatomically complex or pathologically advanced cases may be more likely to undergo OPN rather than MIPN. In addition, it was not possible to assess Clavien grade of postoperative complications, although additional morbidity endpoints, such as readmission, reoperation, and mortality, capture a degree of severity. Furthermore, certain complications of PN, such as urinary leak, are not specifically captured by the NSQIP database and could not be assessed. In addition, it was not possible to not distinguish LPN from RPN in NSQIP. Finally, we did not examine oncologic outcomes or endpoints beyond 30 days postoperatively, which are relevant for patient counseling and treatment selection. Despite these limitations, our study provides a comprehensive characterization of the perioperative morbidity of MIPN compared with OPN in a contemporary, national cohort, as well as characterization of the timing of postoperative complications, hospital readmission, and reoperation.
Conclusions
In this contemporary national cohort, MIPN was independently associated with reduced rates of 30-day complications, perioperative blood transfusion, prolonged hospitalization, hospital readmission, and reoperation, compared with OPN. These results suggest that MIPN techniques should be preferred when technically feasible to reduce perioperative morbidity.
Disclaimer
The American College of Surgeons National Surgical Quality Improvement Program and the hospitals participating in the ACS NSQIP are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.
Footnotes
Author Disclosure Statement
No competing financial interests exist.