
Abstract
Introduction:
Retropulsion, defined as unintended migration of a stone under the influence of the fragmentation device in ureteroscopy (URS) procedures, occurs in 2% to 60% of the cases. Antiretropulsive devices (ARDs) have been studied in experimental and small clinical studies. The current study aims at describing the worldwide usage of ARD and the outcomes related to their usage.
Methods:
The Clinical Research Office of the Endourological Society URS Global Study enrolled 11,885 patients who underwent URS and stone fragmentation for ureteral and/or renal stones. Of the 11,885 treated patients, 9877 were treated for ureteral stones, and data were available on stone migration and ARD use.
Results:
Of all procedures, 14.5% were performed with the use of an ARD. Less stone migration (−2.0%; p = 0.050), higher stone-free rates (SFRs) (2.8%; p < 0.001), and shorter length of stay (−4.7%; p = 0.001) were observed in the antiretropulsive group.
Conclusions:
When an ARD is used during URS, less migration, higher SFRs, and shorter length of hospital stay are observed. This effect is independent from baseline differences and corrected for other treatment characteristics.
Introduction
U
Stone retropulsion, defined as the unintended migration of a stone during fragmentation occurs in 2% to 60% of the cases. 4,6 –11 Migrated stones can obstruct the urinary tract or cause damage or inflammation on the ureteric walls in their new location. To tackle the problem of retropulsion during URS procedures, many antiretropulsive devices (ARDs) such as the Stone Cone (Boston Scientific, Natick, MA), 4,12 the NTrap (Cook Medical, Bloomington, IN), 9,13 and the earlier Dormia-type basket 14,15 have been developed and thoroughly evaluated in experimental settings. 2,4 –7,9 –14,16 –24 In the literature, however, there is no clear indication whether or not to use an ARD during procedures. Most clinicians agree on using such a device during URS in patients with specific stone sizes (both small 2 and large 22 ), patients with increased renal pressure 2,18 (as a consequence of obstruction and hydronephrosis), or in case of impacted stones. 18,22 Other possible factors are type of energy used for lithotripsy 18 and the location of the calculus. 18
Despite some contradictory results in the literature concerning URS outcomes, 10 the overall finding is that using an ARD is advantageous when stone fragmentation is applied. 2,18 The greatest advantage with ARD mentioned in the literature includes lower retropulsion rate. 10,25 Hence, working with ARD does not completely eliminate the risk of migration. 10 An improvement of fragmentation efficacy, 26,27 a decreased intrarenal pressure, 26 the facilitation of fragment extraction, 2 no significant increase in complication rates, 10 and higher (and more secure) stone-free rates (SFRs) 25 have also been reported. Moreover, lower retreatment rates have been reported because nidus formation for stone recurrences through residual fragments can be avoided. 2 Despite the suggested general applicability of URS, 1 the efforts taken to overcome migration of stones to improve intraoperative convenience and postoperative outcomes note the importance of migration and retropulsion of stones. Therefore, the aim of this study is to describe the worldwide use of ARD and its impact on the URS outcomes as well as to examine the predictive factors for stone migration during URS.
Methods
Study population
The Clinical Research Office of the Endourological Society (CROES) URS Global Study is a prospective, observational, international, multicenter study including 11,885 patients with urinary stones. The aims of the CROES URS Global Study and the study population were described in detail in a previous publication. 28
Measures
Characteristics at baseline included age, gender, and body mass index (BMI). Patient's medical history was subdivided to cardiovascular risk (cardiovascular disease [CVD], including diabetes, hypertension, anticoagulant use, stroke, diseases of arteries and veins, and ischemic heart disease), previous stone treatment (any type of treatment for urolithiasis), and stone characteristics (location, stone burden, and stone impaction). Stone burden is calculated as length × width × 0.25 × 3.14159. 29 In addition, the economy of the country, in which the center was located, and the case volumes (the number of treated patients per center) of each of the hospitals were assessed.
Both intra- and postoperative procedure outcomes were measured. Intraoperative characteristics included intraoperative complications, SFRs, and operation time. Intraoperative complications were collected using predefined categories on a standardized case report form (including bleeding, fever, and urinary tract infection). SFR was defined as visual absence of stone fragments larger than 1 mm, left to the discretion of the treating physician. Operation time was measured in minutes and is captured between start and end of the intervention. Postoperative characteristics were length of hospital stay, postoperative complications, and retreatment. Length of hospital stay was dichotomized into prolonged (≥1 day) and normal (<1 day). Postoperative complications were captured using the Clavien–Dindo classification system. 30,31 Retreatment was defined as any kind of retreatment (including readmission), within 3 months after the procedure. Technical characteristics are type of URS and fragmentation device.
Statistical analyses
Descriptive statistics was presented as mean value (standard deviation) for normally distributed data or median value (inter quartile range) for non-Gaussian distributed continuous variables. Categorical and dichotomous variables are presented as n (%).
To analyze the relationship between the use of ARD and procedure outcomes, SFR, complications, long hospital stay, and retreatment, including readmission, an IPWRA (inverse-probability-weighted regression adjustment) model is used. IPWRA uses separate treatment and outcome models. The treatment model is used to weigh the outcome model for baseline differences for treated vs nontreated patients. The treatment model is computed using all possible predictors of the use of an ARD, using a forward selection procedure with patients age, gender, BMI, medical history of CVD, renal congenital abnormalities, preoperatively defined American Society of Anesthesiologists (ASA) score, and possible previous stone treatment together with current stone burden, hydronephrosis (or a preoperative stent to prevent hydronephrosis), impacted stones, fragmentation method, and stone location as possible predictors. Both economy of the respective country and case volume of the center were evaluated for confounding.
The outcome model, which examines the effect of ARD usage on outcomes, has the usage of an ARD as central determinant. This relationship is tested for confounding factors with regard to SFR, operation time, complications, long hospital stay, retreatment, type of URS, type of fragmentation device, and type of evaluation. The models represent the effect of treatment with an ARD on the outcomes. The outcome model is also combined with the treatment model to weigh for the differences between treated and nontreated patients. The level of significance was defined as p < 0.05.
Results
The CROES URS Global Study included 11,885 patients who underwent URS for stones. For the current analyses, only those treated for ureteral stones were included (n = 9877). Out of 9877 patients, in 9691 cases, the information about ARD use (n = 123 [1%] missing data) and stone migration (n = 119 [1%] missing data) was available. Some patients were treated for ureteral stones only (n = 8630), while others were treated for both ureteral and renal stones within the same sitting (n = 1061). Both groups were included. In total, in 1409 cases, an ARD was used during URS (14.5%).
Figure 1 shows the use of ARD among countries. It is interesting to see that in some countries an ARD is used in about 70% of the cases, where in others, an ARD is not used at all. In total, far more procedures are performed without the use of an ARD. Figure 2 presents the most frequently used ARD: The Stone Cone (Boston Scientific); the NTrap (Cook Medical); and the Dormia-type basket, type of basket produced by many, developed by E. Dormia, MD (no single manufacturer).
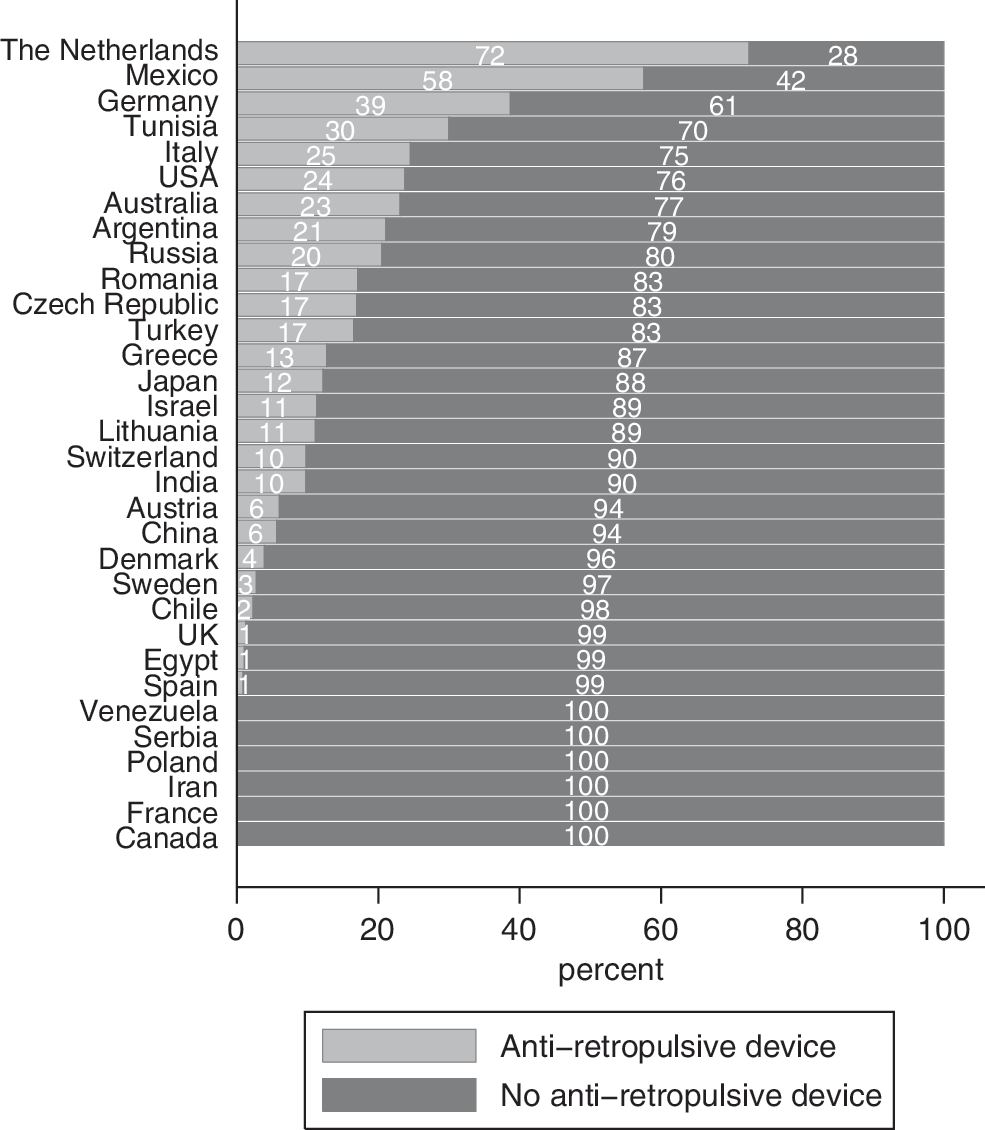
Antiretropulsive device usage worldwide.

Types of antiretropulsion devices.
In the vast majority of procedures performed with the use of ARD, a stone basket was used (11.4%), followed by the stone cone (2.6%) and the NTrap (0.2%). Table 1 shows stone migration occurring during procedures done with and without the use of an ARD. In Tables 2 –5, the descriptive information of the study population, divided in a group with and a group without using an ARD, is shown. Table 2 shows the baseline characteristics, Table 3 shows procedure outcomes, Table 4 shows the technical characteristics of procedures performed, and Table 5 shows the treating centers' information. Notable differences are higher ASA scores, lower stone burden, and longer hospital stay in the group treated using an ARD compared with those treated without the use of an ARD.
ARD = antiretropulsive devices.
ASA score = American Society of Anesthesiologists score; BMI = body mass index; CVD = cardiovascular disease; IQR = interquartile range; SD = standard deviation.
Data are n (%) of patients for whom data were available. Percentages exclude missing values from denominators.
SFR = stone-free rate.
Data are n (%) of patients for whom data were available. Percentages exclude missing values from denominators.
EHL = electro hydraulic lithotripsy; URS = ureteroscopy; US = ultrasound.
Data are n (%) of patients for whom data were available. Percentages exclude missing values from denominators.
BRIC = Brazil, Russia, India, China; MIKT = Mexico, Indonesia, South Korea, Turkey.
Table 6 shows the prediction model of ARD use. Computing a prediction model using forward selection procedure suggests that ARD use is predicted by economy level, case volume, stone location, and patient's preoperative ASA score, and age.
p < 0.05, b p < 0.01, c p < 0.001.
OR = odds ratio; ref = reference category.
In Table 7, the IPWRA model, based on both treatment and outcome models, is shown. Model A shows migration as outcome of ARD use. This model shows that, if all URS procedures were performed with the use of an ARD, the average migration rate would be 0.102, meaning as much as 10.2% of the population would experience stone migration. In addition, if all of the URS procedures were performed without the use of an ARD, the average migration rate would be 0.118. In other words, as much as 11.8% of the population would experience stone migration. The difference of 2.0% represents the treatment effect, the effect that can be attributed to the use of an ARD, and is significant (average treatment effect [ATE] = −0.020, p = 0.050).
Difference is significant when p < 0.05.
Difference is significant when p < 0.001.
ATE = average treatment effect; probabilities based on the full population.
In addition, the differences in SFR (2.8%) and length of hospital stay (−4.7%) reached statistical significance. This suggests that using an ARD is associated with less migration, higher SFR, and shorter length of stay. These differences are independent from baseline differences and corrected for intraoperative confounders. All other outcomes (operation time, complications, and retreatment) are not different for patients treated with or without an ARD.
Discussion
The current analyses of worldwide use of ARD in URS show that in only 14.3% of the URS procedures, an ARD is used. When such a device is used, less migration, higher SFRs, and shorter length of stay are observed. This effect is independent from baseline differences in the groups and corrected for possible other predictors of complications and SFR.
Concerning migration, the idea of basketing is that all fragments that migrate during ureteroscopic stone fragmentation are captured in the ARD. We could confirm the findings of Shabana et al. 10 and Rizkala and Monga 25 regarding decreased retropulsion rate. Consequential lower retreatment rates, due to the absence of residual stone fragments, as proposed by Ahmed et al. 2 could not be confirmed. However, in clinical practice, some stone fragments may pass the ARD and stay in vivo, causing possible future stone formation. 25 These fragments, which are likely to be small residual fragments, could pass spontaneously, which subsequently means no nidus for recurrent stone growth.
Regarding secondary outcomes, namely SFR, complications, operation time, and length of hospital stay, literature showed that using an ARD is better than using none, when stone fragmentation is applied. 2,18 Improvement of fragmentation efficacy, as Bader et al. 26 and Finley et al. 27 propose, could be confirmed in the current study. The idea that facilitation of fragment extraction 2 is more effective, and this is supported by the observed increased SFRs. 25 The improved efficacy as proposed by Bader et al. 26 and Finley et al. 27 is also reflected in the shortened hospital stay in the ARD-treated patients. Usage of ARD does not lead to more complications, this was confirmed in our analyses as well. 10,13 In literature, there is no clear conclusion regarding operation time, 5,10 but with current view on clinical practice, we believe that procedure time is not lengthened by the use of an ARD, as there is no difference between patients treated with or without an ARD.
The current study has some limitations that need discussion. First, availability of devices and techniques is not granted throughout all centers. The selection of cases in which an ARD is used was based on availability of these devices within study centers. This selection could have led to findings related to centers instead of patient groups. However, a group of 1409 cases over 26 countries is a substantial group, which we believe is sufficient to analyze relationships with IPWRA regression analyses. Hence, availability of ARD in combination with types of ureteroscopes may play a role in involuntary retropulsion. Although we corrected for type of scope used (semirigid, flexible, or both), we did not record whether (all types of) ARDs were available in each of the centers. Second, surgeon's experience is an important factor that could influence outcomes. However, this information is unfortunately not captured in the database. We have performed a sensitivity analyses (Appendix Table A1). When examining only those cases that were treated in a hospital with more than 30 cases treated with an ARD, the group of treated patients is smaller, but conclusions on SFR remain. Hence, registries have limitations in their standardization of documentation, and the present project did not include standardized imaging in follow-up. Some questions remain in true SFR when using ARD or not. Third, another important but unexamined factor is the economic consideration of treatment with an ARD. Future research should aim at cost effectiveness of the use of an ARD, to examine whether it is cost effective treating 11,643 patients with an ARD to increase SFRs by only 2.6%. Finally, the CROES URS Global study was performed mostly in the year 2011. Over the past 5 years, the management of stones changed from mainly semirigid toward more frequent use of flexible ureteroscopes. The use of ARD may also have changed. When using flexible scopes, migrated stones can be treated in the kidney when migration occurs, allowing for an extra opportunity to get a patient stone free.
Take-Home Message
Worldwide, 14.5% of the URS procedures are performed with the use of an ARD. When such a device is used, less migration, higher SFRs, and shorter length of stay are observed. Future research should also aim at evaluating the costs of URS procedure.
Footnotes
Acknowledgments
The CROES URS Global Study was supported by an unrestricted educational grant from Boston Scientific, who had no involvement in the design, collection, analysis, interpretation, or reporting of the data. Dr. Nienke Wijnstok provided statistical support for the analyses reported.
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
Appendix
| Model A: Migration | |
|---|---|
| ARD use | |
| Coefficient (CI) | |
| No | 0.132 (0.122, 0.141) |
| Yes | 0.097 (0.079, 0.115) |
| ATE (p) | −0.035 (0.001)a |
| Model B: Stone free | |
|---|---|
| ARD use | |
| Coefficient (CI) | |
| No | 0.881 (0.872, 0.890) |
| Yes | 0.925 (0.910, 0.939) |
| ATE (p) | 0.044 (p = 0.000)a |
| Model C: Operation time | |
|---|---|
| ARD use | |
| Coefficient (CI) | |
| No | 0.810 (0.799, 0.821) |
| Yes | 0.811 (0.789, 0.832) |
| ATE (p) | 0.001 (p = 0.933) |
| Model D: Complications | |
|---|---|
| ARD use | |
| Coefficient (CI) | |
| No | 0.071 (0.063, 0.078) |
| Yes | 0.082 (0.065, 0.099) |
| ATE (p) | 0.011 (p = 0.216) |
| Model E: Long hospital stay | |
|---|---|
| ARD use | |
| Coefficient (CI) | |
| No | 0.386 (0.372, 0.399) |
| Yes | 0.325 (0.297, 0.353) |
| ATE (p) | −0.061 (p = 0.000)a |
| Model F: Retreatment including readmission | |
|---|---|
| ARD use | |
| Coefficient (CI) | |
| No | 0.154 (0.144, 0.164) |
| Yes | 0.153 (0.135, 0.171) |
| ATE (p) | −0.001 (p = 0.945) |
aDifference is significant when p < 0.001.
Excluded: France, Iran, Poland, Serbia, Venezuela, Sweden, Austria, Spain, Chile, Denmark, Egypt, UK, Switzerland, Australia, Lithuania, Tunisia, China, Israel, Mexico, and Canada. (6723 cases left).
ARD = antiretropulsive device; ATE = average treatment effect; CI = confidence interval; IPWRA = inverse-probability-weighted regression adjustment.