
Abstract
Aim:
To evaluate the effects of prostatic apex shape variations on positive apical margin (PAM) rate after radical prostatectomy (RP) by undertaking a comparative study of robot-assisted laparoscopic radical prostatectomy (RALP) vs open radical prostatectomy (ORP).
Patients and Methods:
A total of 3324 cases of RP (1004 ORP and 2320 RALP) from January 2004 to March 2017 were retrospectively reviewed. All patients underwent preoperative MRI and the cohorts were stratified into four categories according to prostatic apical shape at the midsagittal plane. Between ORP and RALP groups, age, body mass index, preoperative prostate-specific antigen (PSA), biopsy and pathological Gleason score (GS), clinical and pathological stage, and prostatic apex shapes were compared. Logistic regression analyses were performed to evaluate significant predictors of PAM. Propensity adjustments were undertaken before statistical analysis to minimize the lack of randomization.
Results:
ORP and RALP groups showed no significant differences in age, body mass index, PSA, biopsy and pathological GS, clinical and pathological stage, as well as prostatic apical shape variations. The ORP group showed a PAM of 17.5% that was significantly higher than 12.3% of the RALP group (p < 0.001). Both groups showed the highest PAM with apical type 3, which is the apex covering the posterior aspect of membranous urethra (ORP 33.9%, RALP 28.5%). In unadjusted data, multiple logistic regression analysis showed that prostate apical type 3 was a significant independent predictor of PAM, but other apex types were not.
Conclusions:
Prostate apical type 3 was a significant independent predictor of PAM. The RALP group showed better outcomes in terms of PAM compared with the ORP group. Preoperative MRI might be a potentially useful tool for preoperative designing of the surgical modalities.
Introduction
P
Patients and Methods
Data collection
Total 3531 patients underwent RP and pelvic lymph node dissection at our institution, because of clinically localized PCa from January 2006 to March 2017. After obtaining the Institutional Review Board approval, we retrospectively reviewed the medical records of those PCa patients. A total of 3324 patients remained after excluding 116 patients who underwent neoadjuvant treatments including androgen deprivation therapy (ADT) or external beam radiotherapy (EBRT). Ninety-one patients who received conventional laparoscopic prostatectomy were also excluded in the final cohort. A total of 1004 ORP patients and 2320 RALP patients were selected from the final RP cohort and included in the study. The surgical workup included preoperative MRI in both ORP and RALP groups. According to the midsagittal image of preoperative MRI, the prostatic apex was stratified into four different shapes as described in our previous study reported in 2006; type 1: apex covering both anterior and posterior aspects of membranous urethra, type 2: apex covering anterior side of membranous urethra, type 3: apex covering posterior aspect of membranous urethra, type 4: apex not covering membranous urethra (Fig. 1). 5 The clinicopathological information of the study cohort was retrospectively reviewed. Four experienced surgeons performed both ORP and RALP. In cases of nerve sparring, the procedure was performed before dissection of the prostatic apex and delicate dissection of periprostatic nerve structure was applied to minimize hemorrhage from the dissecting plane that could possibly hinder recognizing accurate structures of prostatic apex and urethra. The pathological specimens of prostate were reviewed by a single senior attending pathologist and apical margins were thoroughly evaluated. The rates and location of PSM were compared according to different surgical methods and prostatic apical shapes. The rates of early continence recovery were evaluated according to prostatic apical shapes, whereas early continence recovery was defined as the absence of spontaneous urinary leakage requiring more than one pad per day within 3 months after RP.
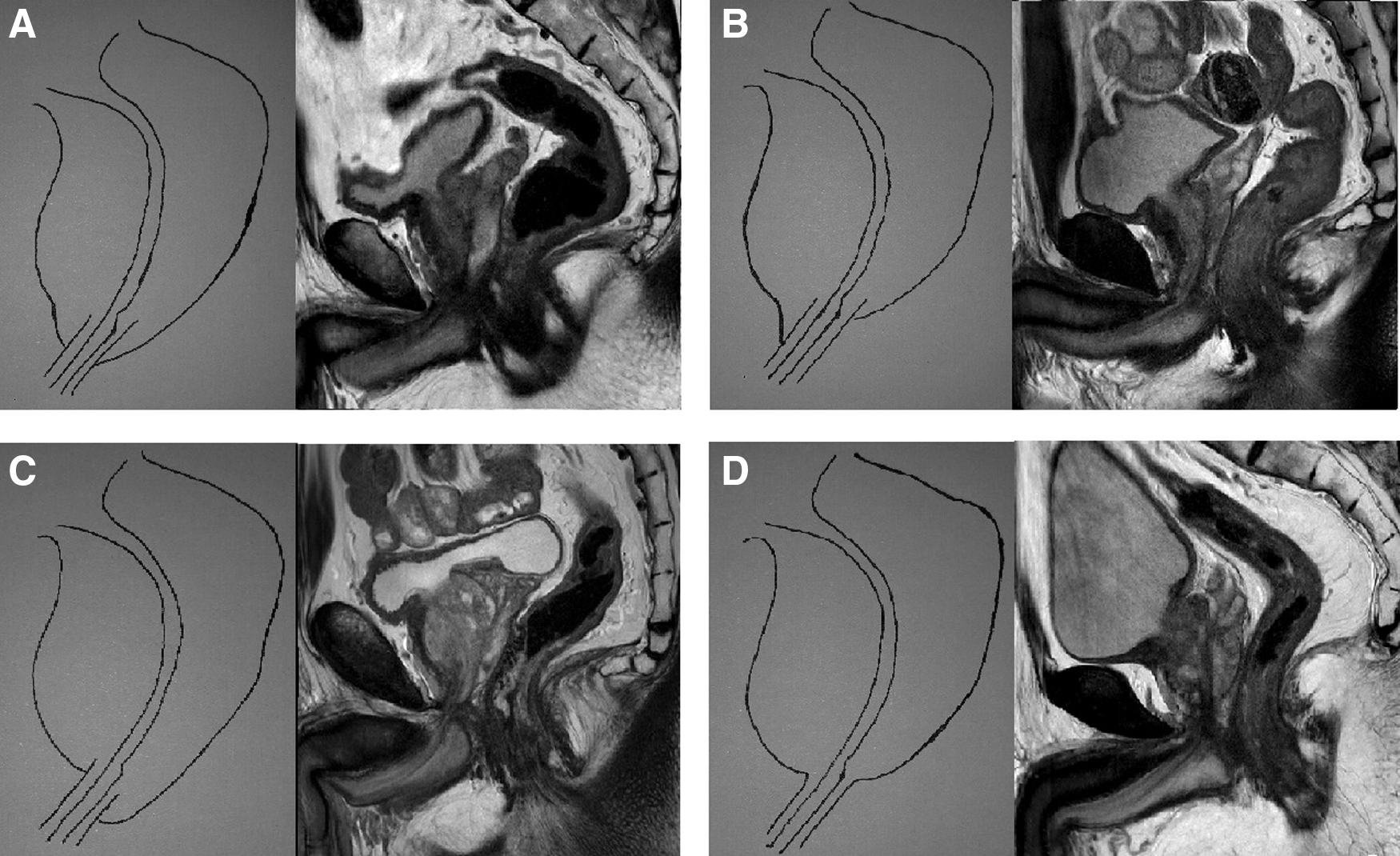
Four types of prostatic apex stratified according to midsagittal MRI scan:
Statistical analyses
All statistical analyses of patients' clinicopathological data were performed using SPSS package version 22.0 (SPSS, Inc., Chicago, IL) and p-values <0.05 were considered significant. Student's t-test and chi-square test were performed to compare the basic characteristics of patients. Univariate and multivariate logistic regression analyses were undertaken to analyze the factors affecting PAM. Means and standard deviations were supplied for continuous variables and proportions were reported for categorical variables. In addition, 1:1 propensity score matching analysis using nearest neighbor matching with a maximum caliber of 0.01 was performed to minimize the lack of randomization. The propensity score was calculated from preoperative characteristics, including age, preoperative prostate-specific antigen (PSA), prostate volume, biopsy and pathological Gleason score (GS), clinical T stage (cT), and pathological T stages (pT). Kaplan–Meier analyses were performed to estimate biochemical recurrence (BCR)-free survival according to the presence of PAM. A Cox's proportional hazards regression model was undertaken to identify the variables influencing BCR.
Results
Baseline characteristics
The differences of clinicopathological features among two surgical groups are presented in Table 1. Total 1004 and 2320 patients were included in the ORP and RALP group, respectively. No significant differences were observed between the two study groups in terms of age, body mass index, PSA, prostate volume, biopsy and pathological GS, cT, pT, and prostate apical shapes. However, when PSM rates were evaluated according to prostate apical shapes, the ORP group had a greater PAM rate compared with the RALP group (before matching: ORP 17.5%, RALP 12.3%, after matching: ORP 15.3%, RALP 12.0%). Both groups showed the greatest PAM rates in type 3 apical shape. The ORP group had the least PAM rates for type 2 apex (before matching: 11.8%, after matching: 11%), but the RALP group showed type 4 with the smallest PAM rates for apex (before matching: 6.2%, after matching: 6.0%) among apical types (Table 1). In terms of early continence recovery, there was no significant difference between the two groups (p = 0.107, Table 1) and both groups showed the greatest rate for type 4 apex (ORP: 85.7, RALP: 88%). However, the RALP group presented significantly better outcomes in early continence recovery after matching, especially for type 4 apex (p = 0.039). The patients with stage ≥pT3 presented greater PAM rates (ORP 25.4%, RALP 22.6%) compared with ≤pT2 patients (ORP 13.8%, RALP 7.5%).
The bold values indicate p-values <0.05 that were considered significant in terms of statistical analysis.
BMI = body mass index; RP = radical prostatectomy; GS = Gleason score; ORP = open radical prostatectomy; PAM = positive apical margin; Prostate apical shape: 1—apex covering both anterior and posterior aspects of membranous urethra, 2—apex covering anterior side of membranous urethra, 3—apex covering posterior aspect of membranous urethra, 4—apex not covering membranous urethra; PSA = prostate-specific antigen; RALP = robot-assisted laparoscopic radical prostatectomy.
Predictors for PAM
The logistic regression analyses undertaken before and after propensity matching revealed that biopsy GS ≥8, and clinical stage ≥cT3b were independent predictors of PAM among the preoperative factors (Table 2). Biopsy GS 7 and cT3a were significantly associated with PAM in univariate analysis, but they failed to achieve independent predictor status in multivariate analysis. Regarding surgical methods, ORP was significantly associated with PAM in prematching data (hazard ratio [HR]: 1.254, p = 0.021), whereas postmatching data indicated that ORP was not a significant predictor of PAM (HR 1.388, p = 0.056). Among the postoperative factors, pathological GS and pT achieved independent predictor status of PAM in pre- and postmatching data (Table 2). Among the four prostatic apical shapes, only type 3 apex was significantly associated with PAM in prematching data (HR: 1.685, p = 0.039). However, postmatching multivariate analyses presented that all four prostatic apical shapes failed to achieve independent predictor status of PAM.
The bold values indicate p-values <0.05 that were considered significant in terms of statistical analysis.
CI = confidence interval; HR = hazard ratio.
The subgroup multivariate evaluation results of clinicopathological features (postmatching data) affecting PAM are summarized in Table 3. For the RALP group, stage ≥cT3b was the only variable significantly associated with PAM among the preoperative factors. Type 3 apex, which was an independent predictor of PAM in a multivariate analysis conducted for the entire study cohort, failed to achieve independent predictor status for the RALP group (odds ratio [OR]: 1.101, p = 0.877). However, type 3 apex was significantly associated with PAM in the ORP group (OR: 5.665, p = 0.001). For the ORP group, four additional preoperative variables, including biopsy GS 7 and ≥8, stage = cT3a, and stage ≥cT3b also reached independent predictor status of PAM (Table 3). Among the postoperative factors, pathological GS and pT were significantly associated with PAM in both RALP and ORP groups (Table 3).
The bold values indicate p-values <0.05 that were considered significant in terms of statistical analysis.
OR = odds ratio.
Predictors for BCR
Kaplan–Meier curves for BCR-free survival are presented in Figure 2, and the results of multivariate Cox proportional hazards regression analyses are presented in Table 4. The postmatching multivariate Cox regression analysis revealed that PAM was significantly associated with BCR (HR 1.691, p = 0.003). There were five additional predictors of BCR in the multivariate analyses, including preoperative PSA, pathological GS 7, pathological GS ≥8, pT3a, and ≥pT3b (Table 4). The presence of PAM was associated with poorer BCR-free survival in the overall study cohort, and both ORP and RALP groups also showed that PAM had a negative effect on BCR-free survival (Fig. 2). Among the patients with PAM, no specific apex type showed better BCR-free survival compared with the other types (Fig. 2).
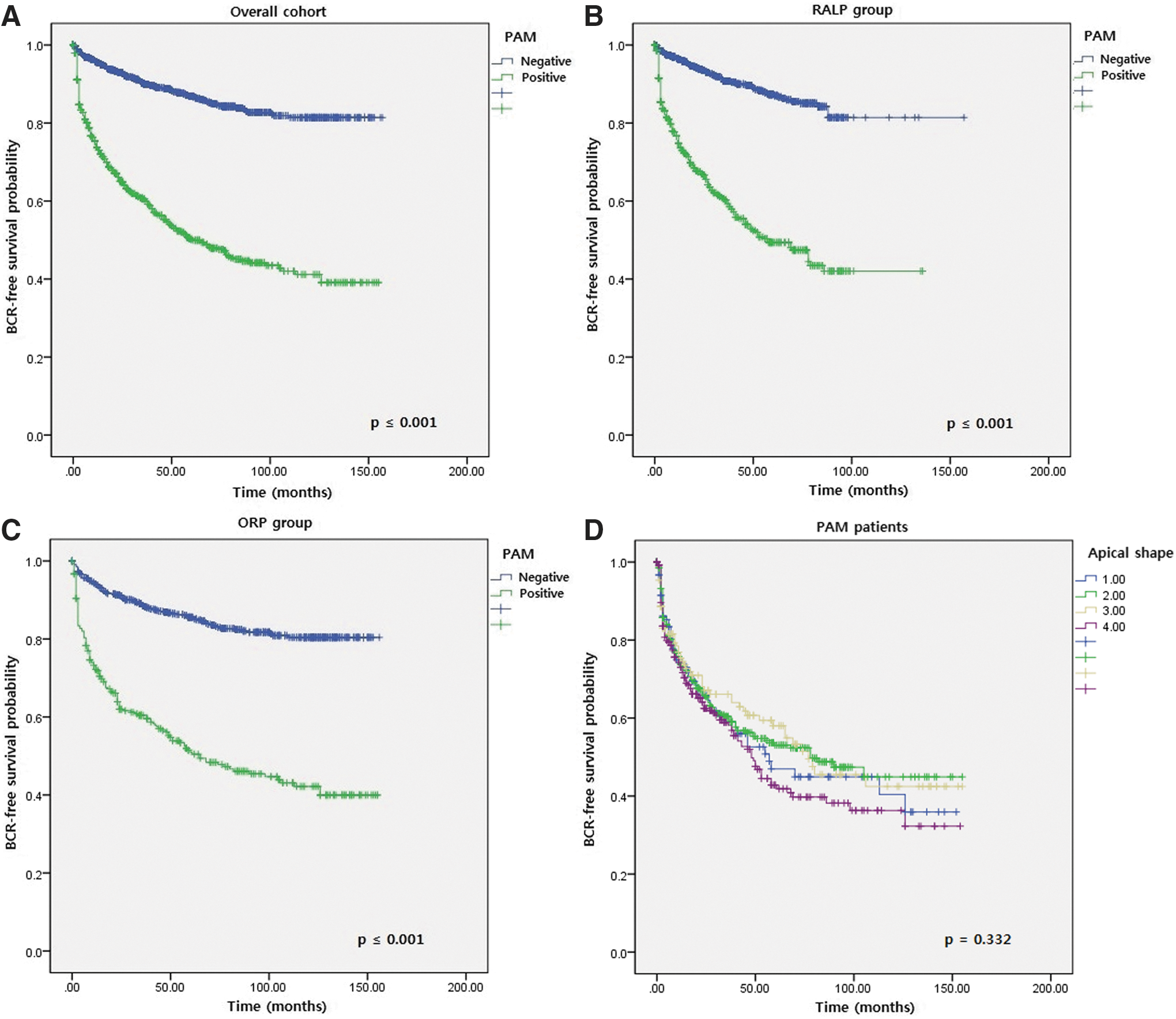
Kaplan–Meier curves for BCR-free survival in different patient groups:
The bold values indicate p-values <0.05 that were considered significant in terms of statistical analysis.
Discussion
During the last decade, the importance of active surveillance has been emphasized in very-low-risk or low-risk PCa, yet RP is still considered the standard surgical treatment for localized PCa. Despite improvements in surgical techniques, PSM has been a challenging obstacle as it is associated with poor oncologic outcomes. 8 Although many previous researches reported that the location of PSM does not possess oncologic prognostic significance, the prostatic apex is one of the most frequent locations of PSM. 8,9 Because of anatomically vague margins between the prostatic apex and the external urinary sphincter, it is occasionally difficult to define whether the cancer tissues within the apex are extraprostatic or intraprostatic, and an additional immunohistochemistry staining is required to confirm PAM. 9,10 Moreover, the broad extent of the dorsal venous complex and the location of the apex under the pubic bone are also challenging factors for surgeons to minimize the chance of PAM. Therefore, compromising the apical margin is occasionally inevitable to maximize urethral length. 11 In addition, early stage PCa, including T1a or T1b exhibits increased rates of harboring the prostatic anterior margin after RP. 10 PAM can be a consequence of intraprostatic incision in the prostatic apex. 12 Intraprostatic incision occurs most often in the prostatic apex and neurovascular bundles because of the difficulties in recognizing extraprostatic extension. Thus, to avoid focal extraprostatic extension into the prostatic apex, lacking prostatic glands within the urethral margin is crucial. 12,13 Recently, von Bodman et al. introduced systematic frozen specimen analysis as an alternative method for reducing PSM. von Bodman and colleagues reported that 22% of patients had PSM, causing the patients to undergo secondary resection of the PSM-involved tissues and converted 92% of them to definite negative surgical margin status. 14 However, the long-term benefits of this systematic approach are still debatable.
We found that stage ≥cT3b, pathological GS, and stage ≥pT3a were significantly associated with PAM in both RALP and ORP groups. Although comparing PAM rates by clinicopathological stage were not undertaken in this study; the ORP group had a higher overall PAM rate compared with the RALP group (17.5% vs 12.3%). These results are consistent with recently published high-volume researches that reported lower PSM rates in the RALP group compared with open surgical approach. 4,15 There have been numerous numbers of multisurgeon, multi-institutional researches published and most of them proposed comparable results in terms of PSM-related factors. In the corresponding studies, the factors associated with PCa aggressiveness, such as pathological GS and clinicopathological stage were significant independent predictors for PSM. 16 –18 However, few studies have evaluated the factors influencing PAM. Matikainen and colleagues 19 measured the apical prostate distance using preoperative MRI and demonstrated that the depth of the prostatic apex within the pelvic cavity was an independent predictor for PAM. In our previous study, we showed that bony pelvic dimensions index was associated with PSM in univariate analysis, but failed to achieve independent predictor status in multivariate analysis. 20 Prematching data of this study showed that type 3 apex was significantly associated with PAM in overall RP patients. However, postmatching multivariate analysis showed that type 3 apex achieved independent predictor status only in the ORP group, but not in the RALP group or overall study cohort. These outcomes might have resulted from the surgical benefits of better intraoperative visuals and improved technical approach to the apex in the RALP group, as suggested by Patel et al. 21
Although type 1 apex covers both anterior and posterior aspects of membranous urethra, type 1 apex has relatively less prominent posterior lobe of prostate covering urethra posteriorly compared with type 3 apex, as demonstrated in our previous study. 5 Thus, as described in the present study results, approaching type 3 apex might be more challenging for surgeons than type 1 apex, which indicates that robotic approach with more delicate apical dissection such as selective ligation of dorsal vascular complex 22 can be a reasonable presurgical option for the patients with type 3 apex. Moreover, our previous study 5 showed that patients with type 4 apex had significantly earlier continence recoveries after ORP compared with the ones with other types of prostate apex, and it is consistent with the results of this study. We believe these outcomes are derived from a relatively longer urethral length in type 4 apex as no apical overlap of the prostate is present in the corresponding apical type. The present study had the greatest number of patients stratified as type 2 apex in both ORP and RALP groups, and this finding is not consistent with our prior study results indicating that type 1 apex (37.8%) was the most common type among the four prostatic apical shapes. 5 This difference in distributions of prostate apical shapes might be deduced from the relatively small cohort (156 patients) of the corresponding prior study 5 compared with the cohort size of 3324 patients in the present study.
Zorn and colleagues 23 and Link and colleagues 24 analyzed the effects of prostate size on RP outcomes and presented higher PSM rates in patients with smaller prostate size. However, this study revealed that prostate volume was not associated with PSM in the apical region. Generally, there might be higher chances for surgeons to dissect smaller prostates more aggressively that causes a possible increase in PSM. It is assumed that the technical maturity of the surgeons involved in this study might have overcome the effect of prostate size on PSM.
The results from this study concordantly showed that PAM is strongly associated with BCR and BCR-free survival of PCa patients after RP that is consistent with other studies. 1,4 However, the significance of PAM in BCR-free survival needs to be further evaluated within the cases having PAM accompanied by PSM in other locations of prostate, because an increase in the number of PSM is associated with higher rates of BCR. 25,26
This study has some limitations. Given the retrospective nature of this study, the treatments within the study cohorts, including postoperative ADT duration and EBRT protocols, are heterogeneous. Therefore, our study results should be further evaluated in prospective analysis. We evaluated PSM rates after RP performed at a single high-volume institution. Thus, the present study results might not be applicable to low-volume research. We did not perform subclassification based on the pathological extent of PAM, whereas some previous studies 27 demonstrated the effect of PSM extent on BCR. Additional factors that can be potentially associated with PAM, such as tumor volume indexes or operative time were not included in the analysis. Despite these limitations, this study still remains the first and the largest known comparison of RALP and ORP techniques in terms of PAM rates.
Conclusions
In conclusion, prostate apical type 3 was an independent predictor of PAM in the analysis undertaken before propensity matching. In subgroup analysis with prematching data, prostate apical type 3 was significantly associated with PAM in the ORP group, but failed to achieve independent predictor status in the RALP group. The RALP group showed better outcomes in terms of PAM compared with the ORP group. PAM was strongly associated with BCR and BCR-free survival.
Footnotes
Acknowledgments
This research was supported by a grant from the Korean Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HI17C1264).
Author Disclosure Statement
No competing financial interests exist.