
Abstract
Introduction:
Intrarenal inflammation has been implicated in the pathogenesis of nephrolithiasis, with prior work showing increased urine levels of IL-6, IL-8, and CCL-2 in stone patients. However, no studies have assessed for inflammation in the renal papillae. We sought to characterize novel papillary tip and urinary biomarkers in stone patients.
Materials and Methods:
Ninety-two patients with nephrolithiasis undergoing percutaneous nephrolithotomy were enrolled. Papillary tip biopsies, kidney urine, and bladder urine were collected, as well as voided urine from eight healthy volunteers. Quantitative polymerase chain reaction was performed to measure inflammatory gene expression.
Results:
Initial 84-gene polymerase chain reaction array revealed significant elevation of several cytokines in stone patients vs controls (fold change 2.3–694). Twenty-four genes were selected for final analysis. In 41 pairs of urine samples, levels of CCL5, CD40, FasL, RIPK2, SELE, TLR3, and IL-15 were significantly elevated in kidney vs bladder urine (p0.0001–0.04). In 23 triplets of samples, expression of these cytokines plus CCL2, CCL7, CCR2, CSF1, CXCL9, and CXCL10, was significantly greater in papillary tips vs urine samples (p0.001–0.05). Cytokine elevation was independent of maximum postoperative heart rate, respiratory rate, temperature, leukocyte count, urinary tract infection in the past year, presence or absence of antibiotics at the time of surgery, and stone composition (all p > 0.05).
Conclusion:
Expression of CCL-2, CCL-5, CCL-7, CCR-2, CD40, CSF1, CXCL-9, CXCL-10, Fas-L, RIPK2, SELE, and TLR-3 is markedly elevated in the papillary tips, kidney urine, and bladder urine of nephrolithiasis patients. Cytokine elevation was independent of signs of systemic inflammation. These findings further support the role of inflammation in nephrolithiasis and imply that the inflammatory process likely begins at the renal papillae. These may represent novel biomarkers of stone disease, which may be useful in basic nephrolithiasis research, disease diagnosis, and prognosis.
Introduction
R
Smaller studies have reported elevated levels of inflammatory mediators in the urine of nephrolithiasis patients when compared with controls, 6 however, no studies have previously tested their expression in both urine and in the papillary tips. Recent work in renal transplantation has demonstrated that mRNA levels in renal transplant patient urine cell sediment may prove clinically useful in the diagnosis and prediction of acute rejection. 7 –9 We therefore sought to determine which inflammatory mediators are present in the urine of kidney stone patients and to localize the source of these cytokines by comparing relative levels in papillary tip biopsies from these patients with their own urine samples.
Materials and Methods
Patient selection
After Institutional Review Board approval and informed consent (Cleveland Clinic IRB #10-927), all adults undergoing elective percutaneous nephrolithotomy for nephrolithiasis at our institution from 2012 to 2015 were approached for informed consent. A urine culture sent 7–10 days before surgery was obtained and all positive cultures were treated with culture-specific antibiotics. Patients with a history of recurrent urinary tract infection (UTI) and/or suspicion for struvite stones (pH >7) were treated with a 1-week course of preoperative ciprofloxacin. All other patients receive a single dose of perioperative antibiotics at the time of surgery.
Specimen retrieval
For control patients, urine was obtained as a clean voided specimen. For stone patients, catheterized bladder urine samples were obtained at the start of the procedure through cystoscopy before instillation of any irrigant fluid. Urine from the bladder could not be obtained in those males whose urethra could not be traversed without irrigant fluid. A renal pelvis urine sample was obtained by retrograde aspiration through a 10-F dual-lumen ureteral catheter passed up the ureter. Urine from the kidney could not be obtained for select individuals with decompressed systems where an inadequate sample volume could be aspirated. Papillary tips with or without Randall's plaques were identified by direct visual inspection. Papillary tip biopsies were obtained using an 8-F cold-cup biopsy device at the completion of PCNL. Papillary tip biopsies were not obtained if the angle of access precluded the ability to reach a papilla with the rigid nephroscope and cup biopsy forces without undue torque. For the pilot study, voided urine was obtained from eight healthy volunteers without history of kidney stones. Clinical variables were obtained from the electronic medical record.
Sample processing
Urine samples were centrifuged, washed with phosphate-buffered saline, and the pellets were resuspended in RNAlater. On collection, papillary tip tissue samples were placed immediately into RNAlater. All samples were kept frozen at −80°C until analysis. RNA was isolated from urine pellet samples with the RNeasy Micro Kit (Qiagen) and from tissue samples with the Invitrogen PureLink RNA Mini Kit (Thermo Fisher). RNA was reverse transcribed using the TaqMan Reverse Transcription reagents and the cDNA concentration was adjusted to 10 ng/μL (based on the input amount of RNA) using Tris-EDTA buffer. To identify candidate genes for further examination, we measured expression of 84 genes using Qiagen RT2 Profiler Human Inflammatory Response and Autoimmunity polymerase chain reaction (PCR) arrays, following the manufacturer's protocol. Results from the preliminary study identified 24 candidate genes that should be further evaluated (Supplementary Table S1; Supplementary Data are available online at
Statistics
Fold change in mRNA expression levels for the pilot study was calculated using Qiagen RT2 Profiler Array Analysis online tools. Cytokine PCR copy number between papillary tip biopsies, kidney urine, and bladder urine was compared using Wilcoxon rank-sum test or Kruskal–Wallis test with Dunn's posttest where appropriate. Differences between groups were considered to be significant at a p-value of <0.05. Spearman's rho was used to examine correlations between marker level and clinical variables. Statistical analyses were performed with GraphPad Prism 5.0 (GraphPad Software, Inc., San Diego, CA).
Results
Of the 92 patients enrolled in the study, 80 patients had at least one adequate urine or tissue sample for analysis (Fig. 1). Usable urine samples were obtained in 73 patients and papillary tip biopsies were obtained from 45 patients; 41 patients had matched pairs of bladder and kidney urine samples, and 23 patients had a full complement of the urine plus biopsy samples, enabling robust comparison of gene expression levels across samples. Five patients had matched pairs of tips with vs without plaque. Patient characteristics are reported in Table 1.
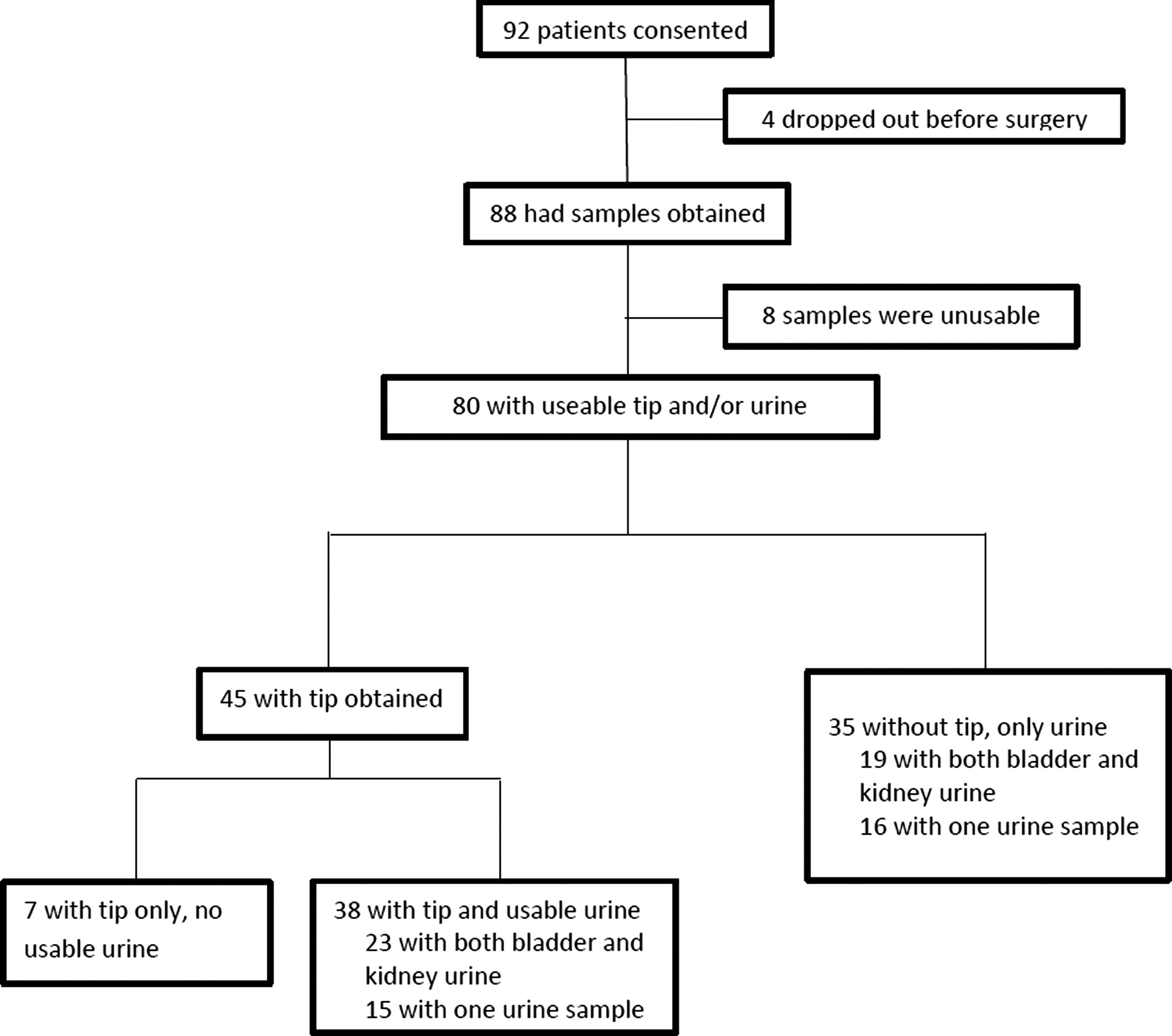
Consort diagram.
Categorical data are presented as frequency (percentage). Continuous data are presented as mean ± SD.
BMI = body mass index; UTI = urinary tract infection.
For the pilot study, papillary tip biopsies, kidney urine, and bladder urine from 4 nephrolithiasis patients were compared with bladder urine from 8 nonstone-forming healthy volunteer controls using an 84-gene PCR array (Supplementary Table 1). Several different inflammatory marker genes were found to be upregulated in nephrolithiasis patients, with increases ranging from 2.3- to 694-fold change vs controls (Fig. 2, A–C). These changes were noted in all three subgroup comparisons, with the smallest significant fold change seen when comparing patient bladder urine vs control bladder urine (range 2.3–90.5), and increasing in degree with more proximal samples (up to 694 for papillary tips). A 24-candidate gene panel was selected from the 84 assayed genes for further analysis in the validation cohort (Fig. 2D). These were chosen to include a diverse array, including upregulated genes, downregulated genes, and genes that had been previously reported in other data. 6 Final PCR analysis with the 24-gene panel was performed on the 80 patient samples collected in the validation cohort.

Inflammatory cytokine expression is upregulated in nephrolithiasis patients vs controls. Data from four nephrolithiasis patients vs eight healthy control bladder urine samples. Eighty-four inflammatory gene PCR array shows differential gene expression of several inflammatory cytokines in nephrolithiasis patient papillary tips
Direct comparison of inflammatory marker levels was performed in five patients with matched pairs of tips with and without plaque. PCR analysis on the 24-gene panel did not show any significant differences in copy number for any gene between these two groups (Table 2). Forty-one matched pairs of kidney and bladder urine samples were included in the final cohort for analysis. In this group, expression levels of CCL-5, CD40, Fas-L, RIPK2, SELE, TLR-3, and IL-15 were significantly elevated in kidney vs bladder urine (Fig. 3, p < 0.04–0.0001). Stone composition in these patients included calcium oxalate monohydrate (N = 13%, 32%), calcium oxalate dihydrate (N = 6%, 15%), calcium phosphate (N = 13%, 32%), uric acid (N = 6%, 15%), cystine (N = 1%, 2%), struvite (N = 1%, 2%), and ammonium urate (N = 1%, 2%). Inflammatory cytokine expression did significantly differ between groups based on stone composition (p0.20–0.81, depending on specific marker analyzed, data not shown).
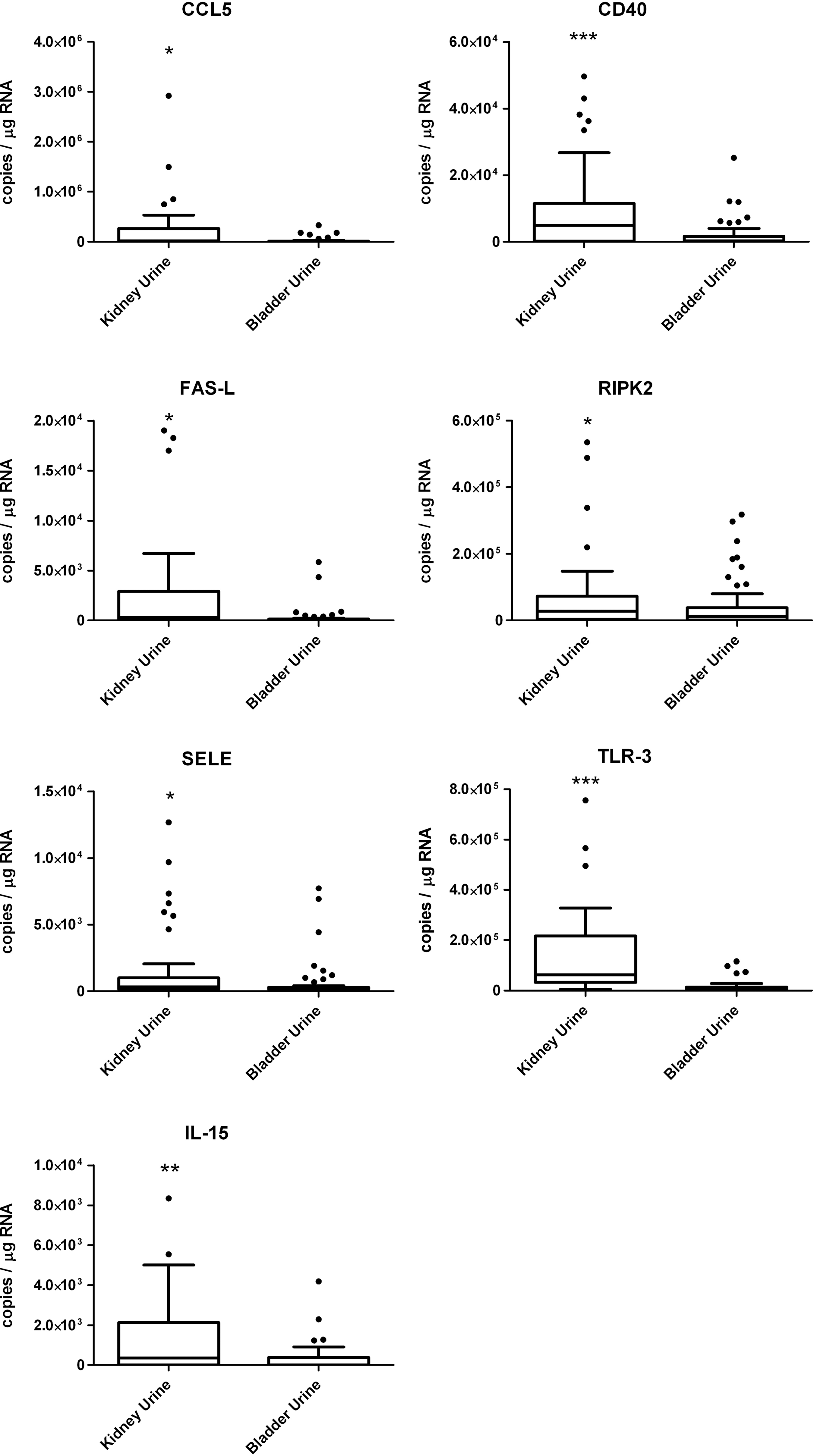
CCL-5, CD40, Fas-L, RIPK2, SELE, TLR-3, and IL-15 are inflammatory biomarkers significantly elevated in kidney urine of nephrolithiasis patients vs bladder urine. Data presented as Tukey Box plots, gene expression measured as PCR copy number/μg RNA. Outliers shown as dots. *p ≤ 0.05, **p ≤ 0.01, ***p ≤ 0.001 by Wilcoxon rank-sum test.
Paired t-test. Significance was judged as p ≤ 0.05.
Twenty-three matched triplets of samples (kidney urine, bladder urine, and papillary tip) were obtained. Significant levels of CCL-2, CCL-5, CCL-7, CCR-2, CD40, CSF1, CXCL-9, CXCL-10, Fas-L, RIPK2, SELE, and TLR-3 expression were noted in papillary tip biopsies vs kidney and bladder urine samples (Fig. 4, p < 0.05–0.001). Kidney urine cytokine mRNA expression levels were generally greater than bladder urine levels, although this did not reach statistical significance when compared in this cohort. Certain markers, such as IL-1β and IL-8, demonstrated a clear trend in the opposite direction. Levels of IL-1β and IL-8 were highest in the bladder urine, lower in the kidney urine, and lower still in the papillary tip biopsies (Fig. 5).
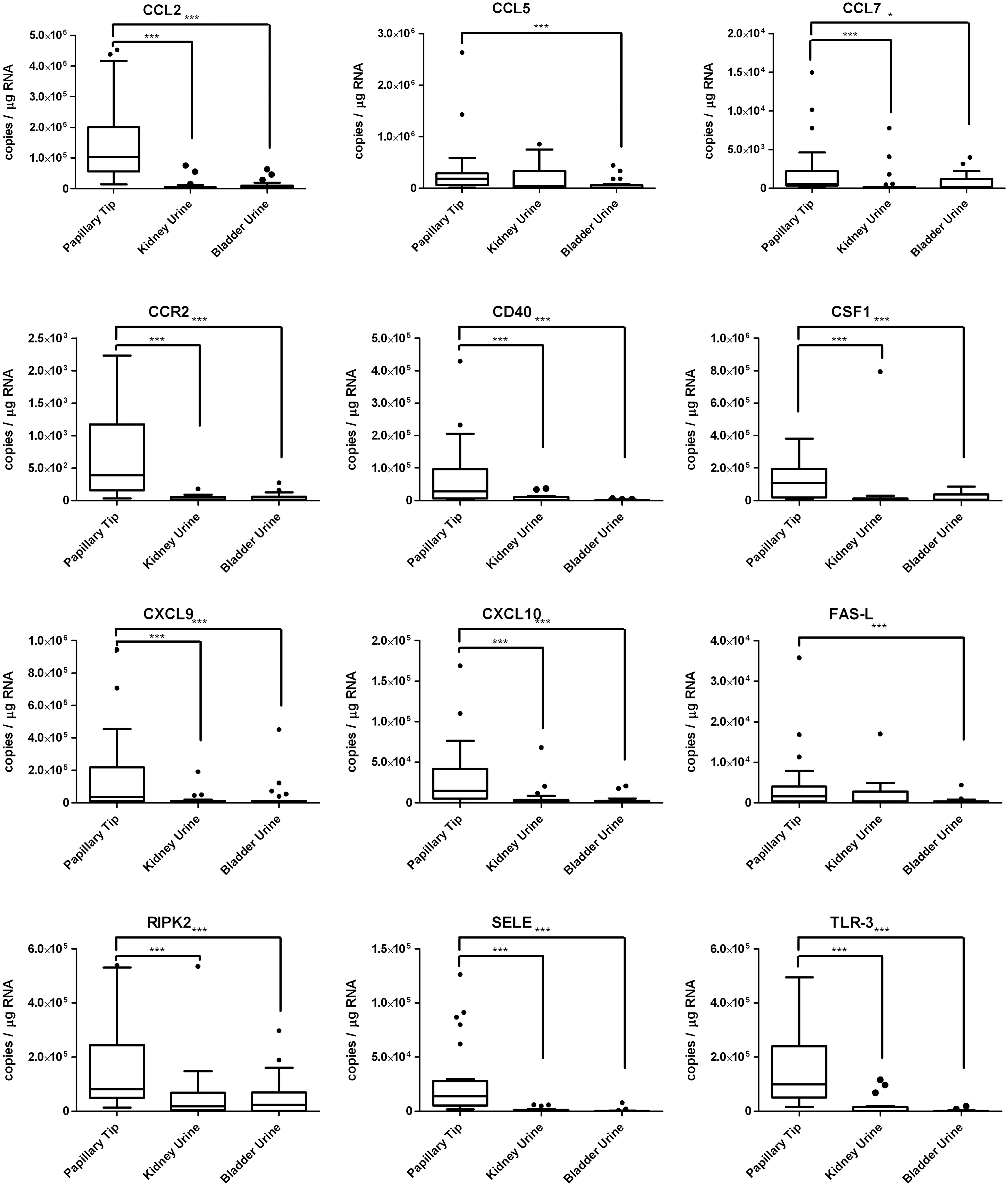
CCL-2, CCL-5, CCL-7, CCR-2, CD40, CSF1, CXCL-9, CXCL-10, Fas-L, RIPK2, SELE, and TLR-3 are inflammatory biomarkers significantly elevated in papillary tip tissue of nephrolithiasis patients vs kidney and bladder urine. Data presented as Tukey Box plots, gene expression measured as PCR copy number/μg RNA. Outliers shown as dots. *p ≤ 0.05, **p ≤ 0.01, ***p ≤ 0.001 by Kruskal–Wallis test with Dunn's multiple comparison test post-hoc.

IL-8 and IL-1B show a trend of increasing copy number in more distal areas of the urinary tract, although without reaching statistical significance. Data presented as Tukey Box plots, gene expression measured as PCR copy number/μg RNA. Outliers shown as dots.
To assess the potential confounding effect of systemic inflammation, biomarker levels were compared against several clinical indicators of systemic inflammatory response syndrome (SIRS). Regression analysis performed for each biomarker against maximum postoperative heart rate, respiratory rate, temperature, and white blood cell count did not show any meaningfully significant correlations (Table 3), demonstrating independence of biomarker elevation from indicators of systemic inflammation. In addition, biomarker levels did not vary by UTI in the past year, or by whether the patient was on antibiotics at the time of surgery (p > 0.05).
Correlation analysis using Spearman's rho with p-values reported in table. Only two significant correlations between marker levels and systemic inflammatory response syndrome criteria were noted (* p ≤ 0.05).
HR = heart rate; RR = respiratory rate; WBC = white blood cell count.
Discussion
In 1937, Randall hypothesized that renal calculi originate from epithelial defects in the renal papilla, at the interface of physiologically complex microenvironments. 11 In recent years, the potential role of inflammation in this microenvironment has been increasingly investigated. In this study, we confirm previous findings that CCL-2, CCL-5, CXCL-9, and CXCL-10 are elevated in the bladder urine of patients with nephrolithiasis undergoing PCNL compared with controls. 6 In addition, we report that CCL-7, CCR-2, CD40, CSF1, Fas-ligand, RIPK2, E-selectin, and TLR-3 are also elevated in the urine of nephrolithiasis patients vs controls. We also report the novel findings that expression of these genes is further amplified, by several degrees of magnitude, in papillary tip biopsies from these patients. Taken together, these data imply that inflammation may play a significant role in the pathogenesis of nephrolithiasis and that this process appears to originate at the papillary tip. This correlates with evidence linking nephrolithiasis to other inflammatory conditions, such as cardiac disease, 12 and atherosclerosis. 13 Recent data have also established an epidemiologic link between kidney stones and asthma in children, perhaps due to shared epithelial ion channel abnormalities related to inflammation. 14
One possible alternative hypothesis is that these inflammatory markers are simply indicators of sepsis or systemic inflammation. However, no significant correlation of cytokine level to postoperative temperature, heart rate, respiratory rate, and white blood cell count was seen. In addition, cytokine levels did not vary between patients with a history of UTI vs those without, nor between patients on vs off antibiotics. This would appear to indicate that the observed cytokine elevations exist independently of systemic inflammation.
Notably, no significant difference was found between the levels of inflammatory mediators in papillary tips identified as containing Randall's plaques and those without plaque. This may indicate that inflammation in the kidney is a global process, taking place throughout the kidney, and not necessarily confined only to those areas with clearly visible Randall's plaque formation, although our sample size was not powered for this comparison. Marker elevation was not significantly different between stones of different types when comparing calcium oxalate, calcium phosphate, and uric acid stones. One would hypothesize that struvite stone formers should have a different cytokine profile than idiopathic calcium stone formers, given the infectious environment in which they form. However, only one patient in our cohort had a struvite stone, limiting our ability to detect this difference. One interesting observation is that certain cytokines, such as IL-8, are highest in the bladder urine, lower in kidney urine, and lower still in the papillary tip. Prior studies have indicated that IL-8 may serve as a biomarker for nephrolithiasis formation. 6 However, all studies to date have only looked at bladder urine, and have not previously examined urine from the renal pelvis or papillary tip. Our findings suggest that IL-8 and IL-1B may be more reflective of a lower urinary tract process. As such, their role as urinary stone markers may be limited.
There are several limitations to this study. Although samples were obtained from 88 patients, sufficient RNA was only available for analysis in 80 of them. An even smaller subset of these patients, 23, had sufficient samples in all categories (papillary tip, kidney urine, and bladder urine). Although this limited our sample size, we felt it best to limit our analysis to only these patients so as to best control for the high interpatient variability in gene expression that was observed. Another limitation is that we are unable to directly evaluate and compare gene expression in papillary tip and kidney urine samples from control patients, due to the prohibitive morbidity of such sample collection in healthy volunteers.
Whether stress associated with surgery itself could explain the observed marker elevations is a reasonable question. Studies on cytokine kinetics after trauma or surgery tend to show an ∼6–72-hour time frame from initial insult to inflammatory marker elevation in both serum 15 and peritoneal fluid. 16 In our study, both bladder and kidney urine samples were collected within minutes of the start of the procedure, and papillary tips were similarly collected as expeditiously as possible. We therefore feel it is unlikely that inflammation from surgical stress alone plays a significant role in our observations.
Although inflammatory markers appear to be significantly elevated in the papillary tissue of nephrolithiasis patients, their exact role is unclear. CCL-2, CCL-7, CCR-2, and CSF1 are associated with monocyte activation, and CCL-2 and osteopontin have previously been linked to renal stones and tubular damage. 17,18 Mouse models with induced hyperoxaluria but without observable stones have shown normal CCL-2 and osteopontin levels, suggesting that elevated papillary tip and urinary levels of oxalate do not trigger inflammatory reactions, and crystal deposition is likely required to activate monocytes. 19 In a study of lithogenic mice, which produce stones when administered glyoxylate, deposition of calcium oxalate into the renal interstitium was found to peak by day 9 of exposure, and almost completely resolved by day 16. Accompanying the rise and fall of crystal deposition was a sharp increase in the number of monocytes and associated cytokines. Cells were seen to be phagocytosing crystals, 19 findings also noted in cultured macrophage studies. 20 Oxidative stress has been displayed in cultured mouse epithelial cells exposed to apatite crystals, with maximal response found once crystals were on the basal side of the basement membrane. 20 NFκB is also an important regulator of proinflammatory gene expression and has been identified to be integral to the expression of CCL-2 and the activation of mesangial cells. 20
Several established models of nephrolithiasis exist, centered around Randall's plaque formation and papillary ductal plugging. 21,22 It is possible that within this construct, papillary inflammation may play a role as a response to initial crystal deposition, which then further promotes stone formation through mechanisms of macrophage infiltration, increased oxidative stress, parenchymal inflammation, and urothelial injury. Conversely, the elevated expression of CCL-5, CXCL-9, and CXCL-10 points to the possibility of a T cell-mediated inflammatory pathway as well. The innate immune system may therefore have multiple roles in stone disease, and a better understanding of inciting factors, chronology, and dysregulation of events will be important in future treatments and the development of new diagnostic and prognostic tests.
Conclusion
Several inflammatory cytokines, including CCL-2, CCL-5, CCL-7, CCR-2, CD40, CSF1, CXCL-9, CXCL-10, Fas-L, RIPK2, SELE, and TLR-3, were found to be markedly elevated in papillary tip samples of nephrolithiasis patients undergoing PCNL. These cytokines were also elevated in kidney urine cell and bladder urine cell samples compared with bladder urine cell samples from healthy controls. No correlation of these inflammatory biomarkers with clinical signs of SIRS was found, implying elevation independent of systemic inflammation. Cytokine expression did not significantly differ between groups based on stone composition. These findings support the role of inflammation in the pathogenesis of nephrolithiasis. Further research should be performed to investigate whether these cytokines can be used as a biomarker signature to inform clinical practice.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.