
Abstract
Purpose:
To evaluate the long-term and flexible cystourethroscopy results of holmium laser enucleation of the prostate (HoLEP) and to compare them with those of plasmakinetic resection of the prostate (PKRP).
Methods:
In the long-term follow-up, variables, including the international prostatic symptomatic score, quality of life scores, maximum flow rate (Qmax), and international index of erectile function (IIEF), and the adverse events, including the need for retreatment, were specifically assessed. One hundred twenty-two HoLEP and 119 PKRP of the initial 280 patients included in this study were available, with 10 deceased and 29 lost to follow-up.
Results:
We found that none of the assessable patients required reoperation for recurrent benign prostatic enlargement (BPE) in the HoLEP group, whereas two required reoperation in the PKRP group. There were no significant differences in most variables between the two groups in the long-term results. But in terms of Qmax, transrectal ultrasound prostate volume, prostate specific antigen (PSA) level, IIEF-5 score, and long-term posttrial follow-up of flexible cystourethroscopy, the HoLEP group showed better results.
Conclusion:
The long-term follow-up data of this randomized trial confirm that HoLEP and PKRP are both effective and durable surgical interventions for the treatment of lower urinary tract symptoms due to BPE. Given the clinically relevant advantages associated with HoLEP, the alternation of PSA level, sexual function, and urination can be improved.
Introduction
L
Both of PKRP and HoLEP appear to be likely candidates to replace traditional TURP as the gold standard for the surgical treatment of BPE. 10,11 In our previous study, HoLEP was observed to be at least as effective as PKRP in terms of improving subjective symptoms and urodynamic findings with a 24-month follow-up. 12 However, HoLEP has been considered as one of the endoscopic procedures with equal or superior efficacy compared with TURP for treatment of patients with BPE because of the high level of evidence for its safety, efficacy, durability, and cost-effectiveness. 13 HoLEP provides a more widely used range, less risk of hemorrhage, reduced bladder irrigation and catheter times, reduced hospital stay and recurrence rate, as well as protects sex function more because of less thermal damage and tissue penetration compared with PKRP with a 48-month follow-up. 14 There is still insufficient long-term follow-up data to compare PKRP with HoLEP in terms of efficacy and safety. An in-depth reassessment of this question has important clinical implications.
Flexible cystoscopy is an important diagnostic tool for the urologist and is used in an outpatient setting for patients who present with hematuria and LUTS, as well as in the diagnosis of bladder cancer, and important for surveillance of patients with known bladder cancer. 15 Investigations that directly assess prostatic anatomy allow the accurate diagnosis of restructuring before it significantly progresses, provide additional qualitative information on the state of healing, and help determine both the need for and the type of intervention. 16 However, the evidence for patients undergoing flexible cystoscopy in relation to LUTS in the long-term follow-up is absent and remains controversial.
The purpose of this trial is to evaluate the effectiveness and applicability of HoLEP compared to PKRP using long-term and flexible cystourethroscopy data from a 72-month follow-up.
Methods
Study design
The present study was performed at our institution and included patients undergoing surgical therapy for LUTS and obstruction due to BPE at our hospital from August 2008 to February 2010. In the initial stages, 280 patients were randomized to PKRP (140) or HoLEP (140) after obtaining ethical approval and the written informed consent of the patients. All patients were initially investigated by medical history and physical examination, including digital rectal examination, prostate specific antigen (PSA) level, uroflowmetry testing, QoL score, transrectal ultrasound (TRUS) prostate volume measurement, postvoid residual (PVR) volume measurement, maximum flow rate (Qmax), and international index of erectile function-5 (IIEF-5) score. Inclusion criteria included a self-administered international prostatic symptomatic score (IPSS) greater than or equal to 9, Qmax of 15 mL per second or less, QoL score of 3 or greater, or urine PVR volume of 50 mL or greater. Those patients who had severe pulmonary disease, heart disease, bladder calculus, neurogenic bladder dysfunction, bladder cancer, previous prostate surgery, prostate cancer, urethral stricture, or coagulopathy were excluded from the study. Those patients who were treated while on treatment with antiplatelets or anticoagulants were also excluded from the study. Initial follow-up at 24, 36, 60, and 72 months after surgery has been collected. In the process of long-term follow-up, the variables, including IPSS, QoL, Qmax, cystoscopy, and the IIEF-5 score, were assessed. Adverse events, including delayed bleeding and the need for retreatment, were also specifically assessed.
Surgical procedure
Our experienced urologists have treated 500 cases of TURP and 200 cases of PKRP and HoLEP before enrolling patients for this study. HoLEP was performed using a 550 μm end firing laser fiber and a 100 W continuous flow VersaPulse® holmium laser and a 27F resectoscope with a modified bridge to hold the laser fiber (Storz, Tuttlingen, Germany). Power settings were 80 to 100 W at 2 to 1.5 J per second and 50 to 40 Hz. Transurethral morcellation was performed through a 26F nephroscope using a mechanical morcellator (VersaCut™).
PKRP was performed using the PlasmaKinetic™ SuperPulse system, consisting of a PK® generator, a PK resectoscope, and a Plasma-Sect® electrode. The generator for PKRP was set at 160 W for cutting and 100 W for coagulation. A 27F continuous flow resectoscope (Storz) was used for PKRP.
Outcome measures
Once symptoms and/or an obstructed flow were detected by uroflowmetry, flexible cystourethroscopy was performed under local anesthesia as part of our routine follow-up protocol to visualize tissue responses to enucleation of the prostate. To illustrate this point, we defined a grading system that ranged from a low of 0 to a high of 5 (higher numbers indicate better recovery).
Statistical analysis
Data were done using the SPSS computer program (version 17 Windows). Follow-up data of grade were statistically analyzed with a Wilcoxon Rank Sum Test, and other data were analyzed with a two-tailed Student's t test. The data were presented as mean ± SD, and p values <0.05 were considered statistically significant.
Results
Evaluation of IPSS, QoL, and Qmax after surgery
In our previous work, we found that the baseline characteristics of the PKRP vs HoLEP groups were not significantly different in any aspect, and patients in the HoLEP group displayed a lower risk of hemorrhage, shorter bladder irrigation and catheterization time, and shorter hospital stays. A larger amount of prostate tissue was retrieved in the HoLEP group, but the operation time was longer for this group than for the PKRP group. In the last 2 years, due to the development of new technologies, such as of enucleation and morcellation, the operating time of HoLEP has been greatly reduced; this can offset the time-consuming limitation associated with HoLEP. The preoperative and 1-, 6-, 12-, and 24-month postoperative data for IPSS, QoL, and Qmax were shown in the previous report. 12 Compared with the baseline, significant improvements were observed in these primary outcomes in both groups after surgery. However, there were no significant differences between the two groups. The 36-, 48-, 60-, and 72-month postoperative data for IPSS, QoL, and Qmax are shown in Table 1. IPSS was lower at the 72-month follow-up in the HoLEP group (8.79 ± 0.18) compared with PKRP group (10.03 ± 0.16). Qmax was lower at the 60- and 72-month follow-up in the PKRP group (17.50 ± 0.29 and 15.92 ± 0.30) compared with HoLEP group (19.26 ± 0.28 and 17.71 ± 0.28). However, there was no significant difference in Qmax between HoLEP and PKRP group at the 36- and 48-month follow-up (p = 0.90 and p = 0.45).
FC = follow-up scores of the flexible cystourethroscopy results; HoLEP = holmium laser enucleation of the prostate; IPSS = international prostatic symptomatic score; PKRP = plasmakinetic resection of the prostate; Qmax = maximum flow rate; QoL = quality of life.
Evaluation of TRUS, PSA, and IIEF-5 after surgery
TRUS prostate volume (mL) in HoLEP and PKRP before surgery was 56.70 ± 28.41 and 60.31 ± 22.41, respectively. PSA (ng/mL) in HoLEP and PKRP before surgery was 2.23 ± 1.27 and 2.35 ± 1.52, respectively. IIEF-5 in HoLEP and PKRP before surgery was 18.02 ± 3.37 and 18.34 ± 3.29, respectively. The TRUS, PSA, and IIEF-5 data after surgery are presented in Table 2. The long-term follow-up data showed that TRUS and PSA were lower at the 24-, 48-, and 72-month follow-up in the HoLEP group compared with PKRP group. Regarding the IIEF-5, there was no significant difference between the two groups in the first 24 months after surgery. But the long-term follow-up data showed that IIEF-5 was higher at the 48- and 72-month follow-up in the HoLEP group compared with PKRP group, suggesting the advantage of HoLEP. Two years after surgery, the sexual function of these patients was generally declining. Compared with the HoLEP group, the scores of sexual function decreased more quickly in the PKRP group (p < 0.01). During the 24-month follow-up, retrograde ejaculation was reported by 5 of 16 patients in the PKRP group and by 4 of 18 in the HoLEP group. While in the process of long-term follow-up, the results of retrograde ejaculation were limited.
IIEF-5 = international index of erectile function-5; PSA = prostate specific antigen; TRUS = transrectal ultrasound.
Evaluation of FC after surgery
At 5 years after surgery, there were 44 patients (HoLEP 23 and PKRP 21) who volunteered to undergo flexible cystoscopy during a follow-up visit. Based on the combined consideration of the outcome of Qmax and cystoscopy imaging, the post HoLEP operation recovery is better. To illustrate this point, we define a grading system that ranged from a low of 0 to a high of 5 (higher numbers indicate better recovery) (Fig. 1A–F). As no difference in prostate volume was found between the two groups before surgery, the difference between the two groups in the area of the wound surface could be considered not significant. Five years after HoLEP or PKRP surgery, the patients in the HoLEP group had the benefit of better and quicker wound healing. The wound surface of PKRP lacks smoothness or regularity, and the bladder neck also has an irregular shape. The follow-up scores of the flexible cystourethroscopy results are 3.83 for HoLEP compared with 3.05 for PKRP (Table 1); thus HoLEP performs better.
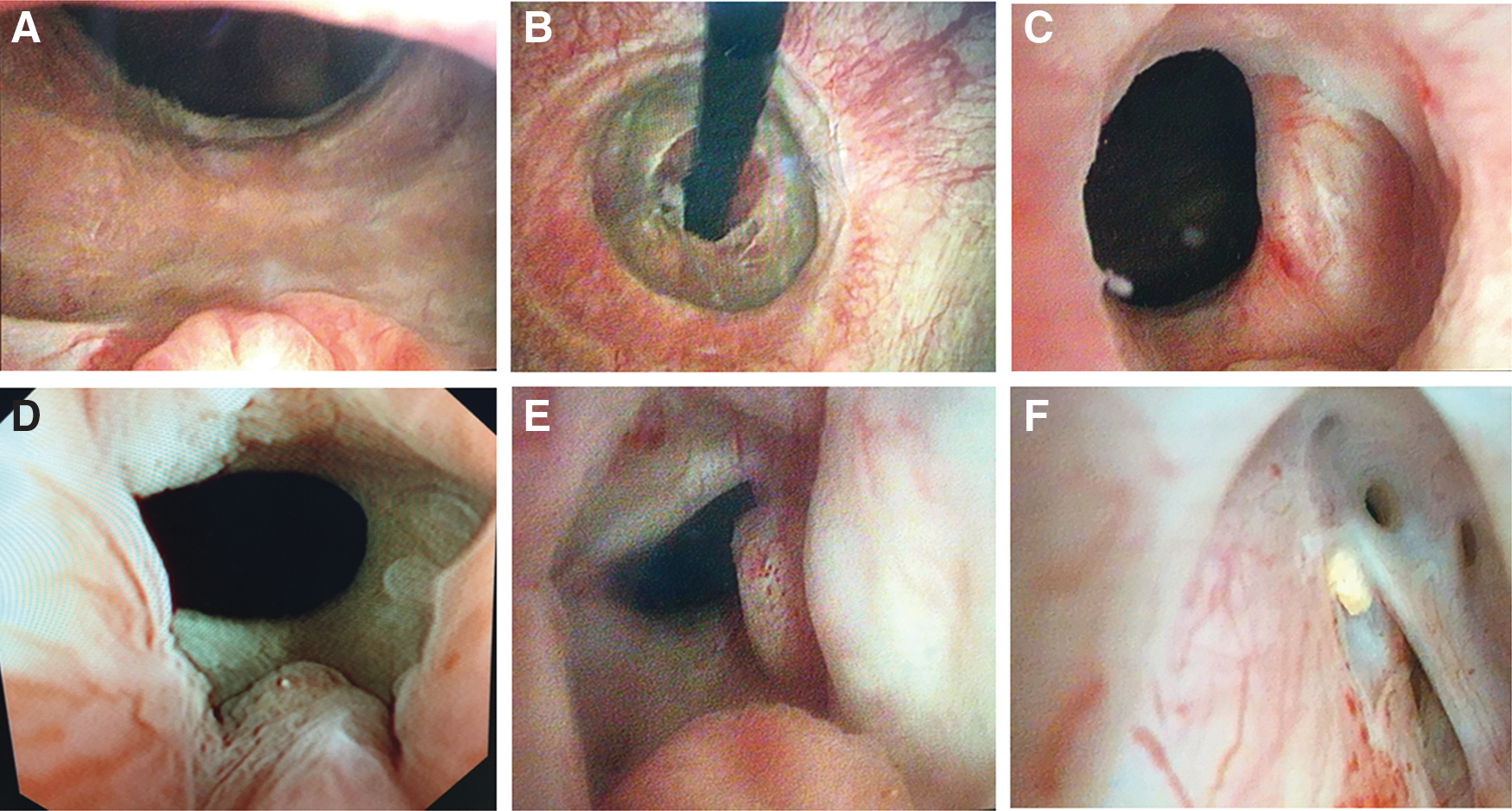
The flexible cystourethroscopy results of the prostatic cavity wall.
Discussion
Several surgical methods have proven to be safe and effective for the treatment of benign prostatic obstruction. TURP and PKRP have remained the procedure of choice for the surgical treatment of bladder outflow obstruction for several years. 8,17,18 HoLEP is now emerging as a challenger to the gold standard procedure. 19,20 The advantages of HoLEP have been shown by the outcome data of short-term follow-ups; our prospective randomized trial using the first 2-year follow-up data of HoLEP vs PKRP has shown that HoLEP had a better result than PKRP in treating BPE. However, the limitations of that study included absence of long-term follow-up. The present study introduces the evidence base for PKRP vs HoLEP, with the particular data of a randomized, controlled 6-year follow-up study. At long-term follow-up, HoLEP was still found to be superior to PKRP in several aspects, a result that is similar to other long-term data.
Fortunately, in the 6th year, there were only 39 patients (18 HoLEP and 21 PKRP) who were lost to follow-up; this is superior to other comparable research studies. 17,19,21,22 The improvement of the living standards and the fact that most patients are neighboring residents may have led to a lower lost rate of follow-up.
In the last 6 years, there were no reoperations in the HoLEP group, whereas there were four in the PKRP group. Two patients were found to have bladder neck stenosis, and the other two had adenomatous remnant or recurrence of prostatic hyperplasia. At 6 years, the symptom scores were significantly lower in the HoLEP group, but at former years there was no difference between the two groups.
Previous evidence showed that PSA levels and prostate volume decreased more in the HoLEP group than the PKRP group, indicating that more prostate tissue was resected in HoLEP group. 12 Additional evidence of this long-term follow-up revealed that HoLEP is better than PKRP in slowing some disabling effects and decreasing the recurrence of BPE. 14 Enucleation along with the gouge of the surgical capsule could minimize the residual prostate tissue and reduce the chance of relapse of prostate tissue.
In the process of long-term follow-up, HoLEP gradually manifested its superiority in improving dysuria. From 36-month postoperatively, the maximal urinary flow rates of all patients were better maintained, but began to decline, and such decline was even faster in the PKRP group. Noteworthy difference in two groups can be observed at year 5. Similar trends were observed in the follow-up of the patient's sexual function. Similar results can also be seen in the follow-up of PSA levels and TRUS data. The difference is that the increase of the changing trends of the PSA levels and TRUS data is more obvious in the PKRP group. After operation, this negative development means that some part of prostate tissue has started to grow again. But even at that rate, the trends over the past 6 years give cause for optimism in all patients.
The most ideal operation method for BPE is one that can acutely remove as much as possible the prostatic adenoma within the surgical capsule and have as little as possible perioperative morbidity while providing as good as possible and durable patient outcomes. 21,23,24 Ahyai and colleagues 19 reported that the prostatic cavity after enucleation is similar to that after the open procedure; HoLEP has a remarkable outcome on immediate BPE symptom relief, but in addition, it also has it on late assessment. To assess the condition of recovery of prostatic cavity after enucleation using a scoring system that ranged from 0 to 5 (higher numbers indicate better recovery), patients are graded on the basis of information supplied in response to eventual recovery of the wound's surface of the prostatic cavity. According to the practical value in five different conditions, problems of each assignment will be graded 0 or 1 point. On the premise that patients had got normal voiding, bladder neck and prostate apex in good form each can get 1 point. In addition, it also means that 1 point would be deducted for one unsatisfactory case, and full mark is 5 points.
Each of the left or right prostatic cavity walls (after removal of the prostate gland) without good recovery could not restore its smoothness or elasticity without residual and recurrent adenoma; thus 1 point would be deducted. Postoperative complications occurred in four cases (1.4%), including the bladder neck stenosis and recurrence of prostatic hyperplasia, making significant dysuria, thus 5 points would be deducted all at one time, considering the lowest score of all. For instance, Figure 1A and B of the patient can be given 5 points; he is one of the best postoperation rehab we had. For the patient in Figure 1D, his prostatic cavity walls recover well with no adenoma recurrence, but as his bladder neck and prostate apex had no good form, each was deducted 1 point; thus he only can get 3 points. For the patient in Figure 1F, his bladder neck stenosis makes dysuria or is painful, so he needs another operation and thus gets 0 point. By that analogy, the clinical effects of HoLEP and PKRP can be evaluated by the flexible cystourethroscopy results.
To date, as holmium laser enucleation therapy can enucleate more prostate tissue, promote wound healing, and reduce gland residue or recurrence, maybe HoLEP is the most suitable technique that can meet all of these criteria. Nevertheless, over the next few years in clinical practice, PKRP could still be able to be accepted as a valuable intervention in the armamentarium of urologists, especially in the economically less-developed regions. However, with growing economic pressures and the evolution of minimally invasive therapies, its presence might potentially fade.
The main limitation of the present study is the flexible cystourethroscopy assessment system of the postoperative recovery condition. Therefore, we established the relatively objective evaluation criteria according to the recovery of bladder neck and prostate fossa after operation. Although its accuracy may not be satisfactory, the present study is the first to report the long-term posttrial follow-up of flexible cystourethroscopy.
Conclusion
HoLEP is at least equivalent to PKRP in the long term with fewer required reoperations and it could reduce the damage of the sexual function and decrease recurrence rate.
Footnotes
Acknowledgments
This work was funded by the Shanghai Municipal Science and Technology Project (15DZ1941503) and Key Disciplines Group Construction Project of Pudong Health Bureau of Shanghai (PWZxq2014-11).
Author Disclosure Statement
No competing financial interests exist.