
Abstract
The envelope is constantly being pushed to minimize the invasiveness of prostate cancer surgery without compromising oncologic or functional outcomes. Transperitoneal robot-assisted radical prostatectomy has certainly accomplished these goals. However, it is our intent to push the envelope even further, that is, to minimize the invasiveness of already minimally invasive surgery. To accomplish this lofty goal, we borrowed the transperineal approach from open surgery and fused it with the latest robotic technology to innovate an extraperitoneal robotic prostatectomy technique that is less invasive than the traditional robotic technique.
Indications
T
Preoperative Preparation
Surgery is generally scheduled at least 1 month after prostate biopsy to minimize biopsy-related inflammation. In preparation for surgery, antiplatelet and anticoagulation medications are stopped for 1 week before surgery if medically feasible. A bowel preparation is completed the day before surgery.
We first described the robotic perineal prostatectomy technique using a multiport approach with the da Vinci Si surgical system (Intuitive Surgical, Sunnyvale, CA) through a GelPOINT access platform (Applied Medical, Rancho Santa Margarita, CA). 1 With the advent of purpose-built single-port robotic technology, we have adapted the technique to be performed with the da Vinci SP1098 robotic system (Intuitive Surgical, Sunnyvale, CA), a second-generation single-port robotic surgical system. The SP1098 possesses a 25-mm multichannel port that accommodates an articulating high-definition robotic camera, three 6-mm double-jointed articulating robotic instruments, and a 6-mm accessory laparoscopic instrument. The design and functionality of SP1098 have been described previously in detail. 3,4
Patient Positioning
The patient is positioned in exaggerated dorsal lithotomy with 15° of Trendelenburg. All pressure points are padded, and the extremities are maintained in neutral positions (Fig. 1).

Patient positioning.
Surgical Steps
Perineal access and robot docking
A 2.5-cm omega incision is made in the midline between the ischial tuberosities (Supplementary Video S1; Supplementary Data are available online at

Posterior dissection
Posterior to the prostate, Denonvillier's fascia is identified and incised (Supplementary Video S2). The posterior plane is bluntly developed along the length of the prostate. The vas deferentia and seminal vesicles are identified and dissected out. The vasa deferentia are divided with electrocautery, and the blood supply to the seminal vesicles is controlled with clips (Fig. 3a, b).
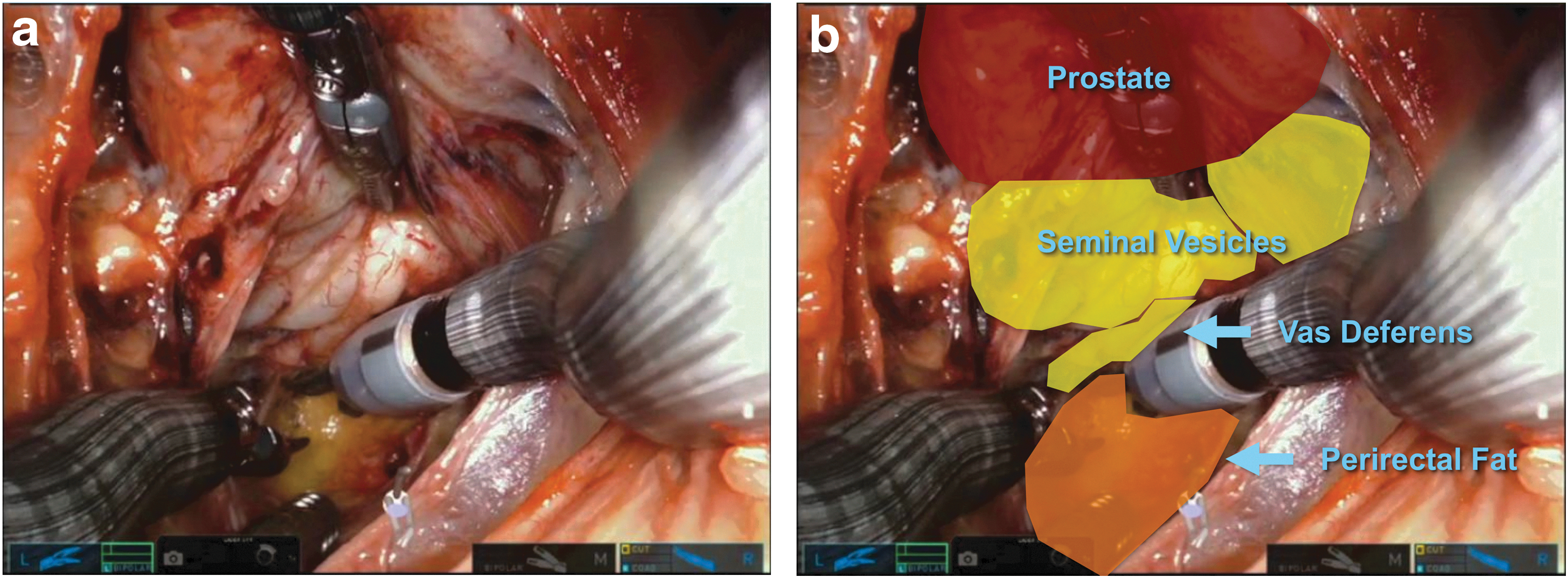
Posterior dissection—video still without
Lateral dissection and vascular pedicle control
The lateral aspect of the prostate is dissected out bilaterally, defining the prostatic pedicles (Supplementary Video S3). The prostatic pedicles are ligated with clips and divided (Fig. 4a, b).

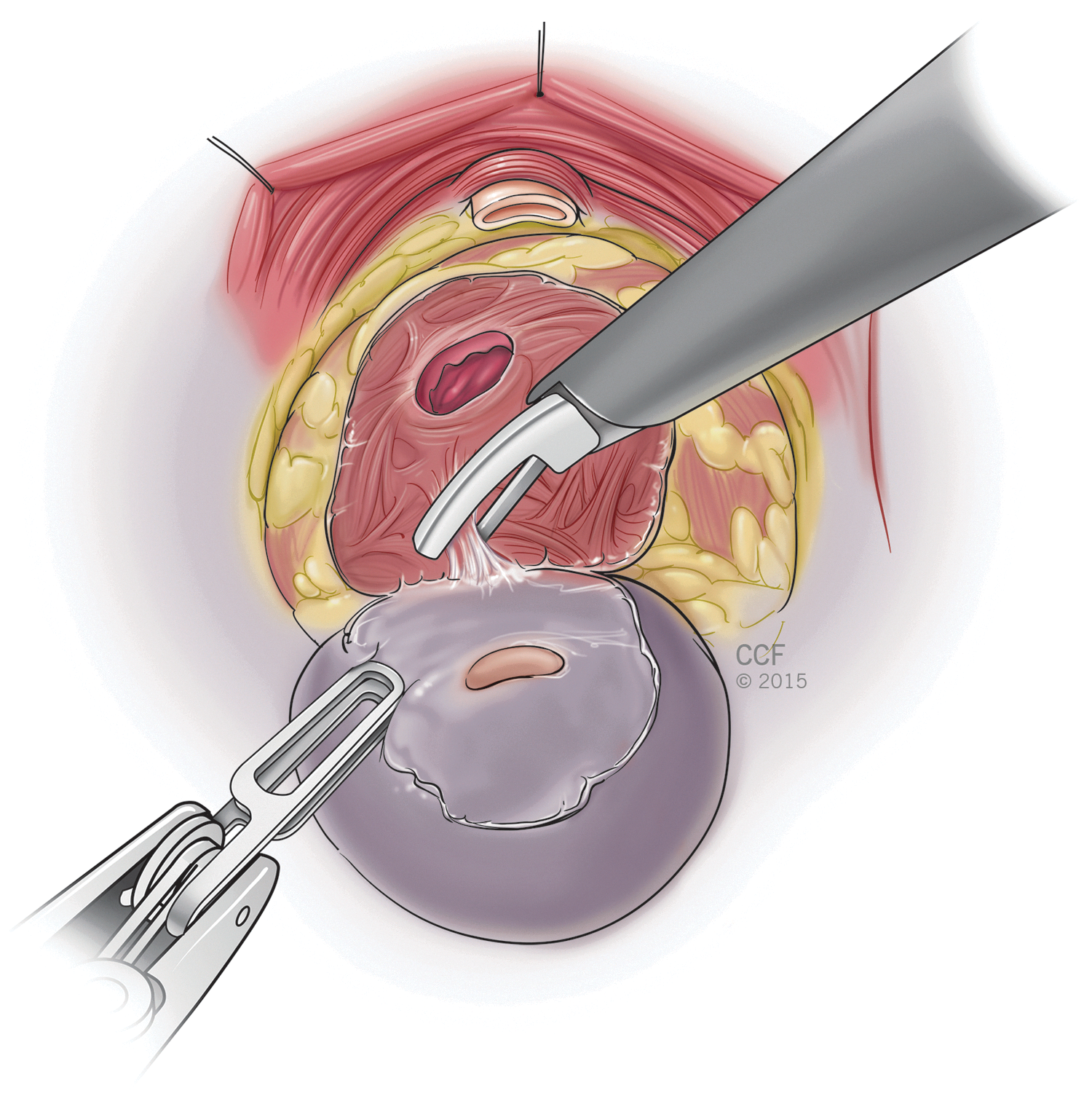
Apical and anterolateral dissections
The prostatic apex is dissected out posteriorly, defining the urethral–prostatic junction, and the urethra is transected (Supplementary Video S4). The anterolateral surface of the prostate is bluntly developed from the apex of the prostate to the prostatic–vesical junction. The dorsal venous complex is preserved (Fig. 5).

Apical and anterolateral dissections.
Bladder neck dissection
The bladder neck is transected, freeing the prostate of its last remaining attachment (Supplementary Video S5). The prostate specimen is extracted through the perineal access site (Fig. 6).
Bladder neck dissection.
Pelvic lymphadenectomy
After removal of the prostate, the extraperitoneal space is developed medial to the pelvic sidewall and lateral to the bladder bilaterally, exposing the obturator fossa and external iliac vein (Supplementary Video S6). The obturator and external iliac lymph nodes are dissected out and extracted through the perineal access site (Fig. 7a, b).
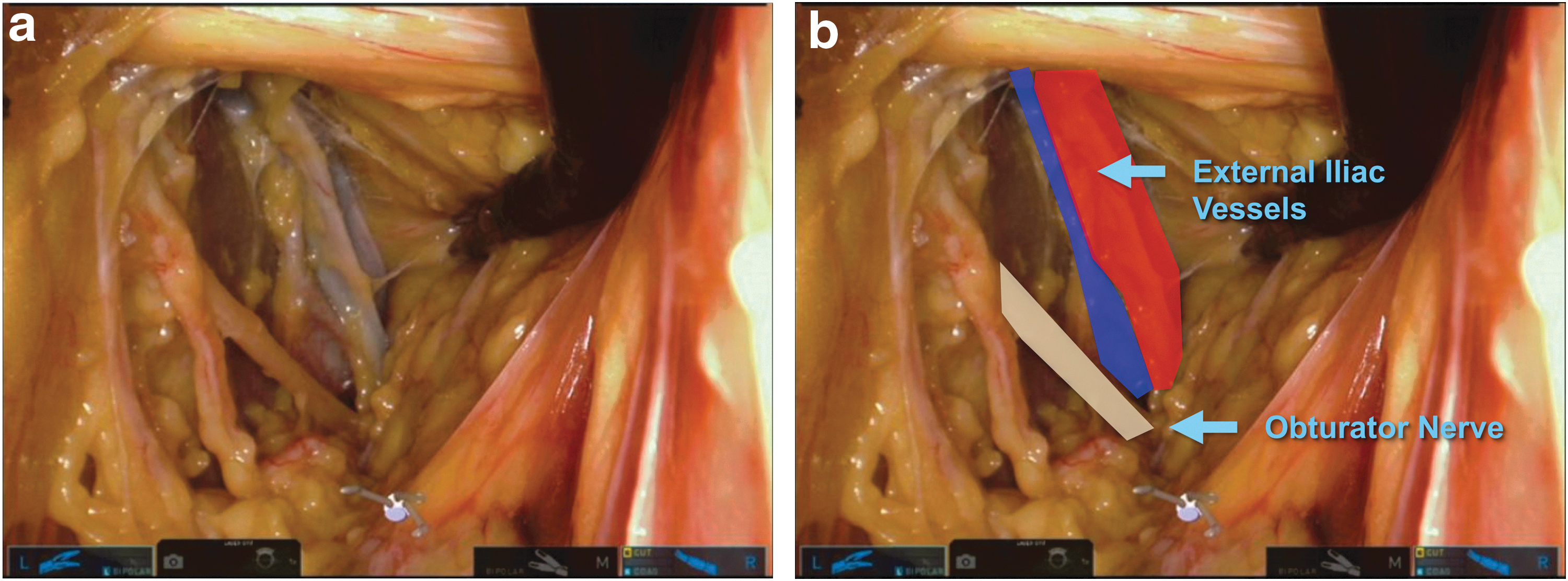
Pelvic lymphadenectomy—video still without
Vesicourethral anastomosis
The anastomosis is performed in a running manner over a catheter, beginning anteriorly and finishing posteriorly (Supplementary Video S7). The anastomosis is tested to ensure a watertight closure. The robot is undocked, and the single port is removed. The incision is closed in two layers over a closed suction drain (Fig. 8a, b).
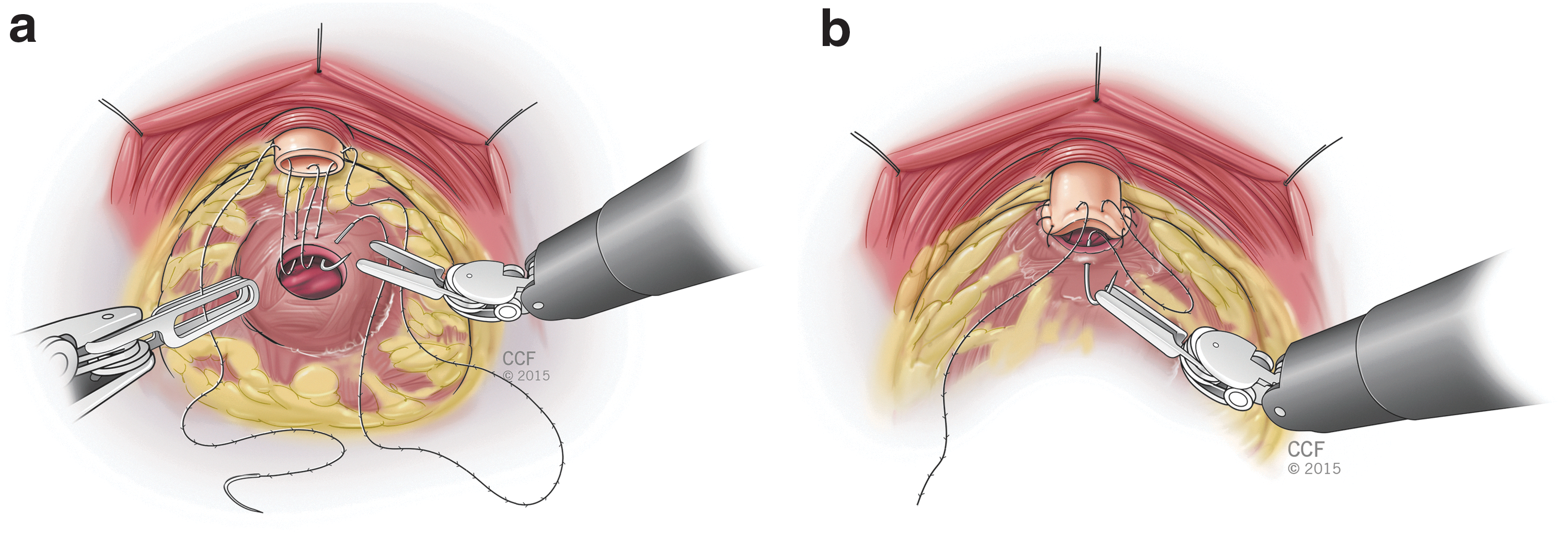
Vesicourethral anastomosis
Outcomes
The total operative time was 180 minutes. There were no intraoperative complications, and the surgery was completed without the need for conversion to other approaches and/or techniques.
Postoperative Care
The postoperative care path is similar to that following standard robotic prostatectomy, including immediate diet resumption, minimization of narcotic pain medications, and early ambulation. Patients are observed postoperatively and discharged home within 24 hours in routine cases. The perineal drain is removed before discharge, and the urethral catheter is removed after 1 week.
Trouble Shooting
Compared with standard transperitoneal robotic prostatectomy, the clinical situations that typically pose challenges, such as obesity or previous abdominal surgeries, are less problematic using an extraperitoneal perineal approach because of avoidance of the intra-abdominal cavity. However, there are several technical considerations specific to the SP1098 that are important to recognize when performing SP-RAPP. First, unlike conventional robotic technology, whereby the robotic arms move around fixed pivot points, the SP1098 robotic arm and the single port to which it is attached can be moved in the xy plane, independently of the robotic instruments, which greatly improves maneuverability within the operative field. Second, the instruments are double jointed with a hinged proximal joint and an articulating distal (wrist) joint to allow maximal range of motion within the body. The articulating wrist, although highly effective and easy to operate, requires some adjustment for the robotic surgeon who is accustomed to nonarticulating instruments. Lastly, the robotic camera is articulating as well, which improves camera mobility but requires some surgeon adjustment. Since the camera and instruments all enter the body through a single port, the surgeon must constantly adjust the position of the camera relative to the robotic instruments. On the surgeon's console, a navigation system tracks the locations of the single port, the camera, and the instruments within the operative field, and alerts the surgeon as they reach their respective limits. To view full video, “SP1098 prostatectomy with voiceover full video.mp4,” click here.
Footnotes
Author Disclosure Statement
Dr. Kaouk is a consultant for HealthTronic, Inc. and Intuitive Surgical, Inc.
Abbreviation Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.