
Abstract
Introduction:
Radical cystectomy and extended pelvic lymph node dissection (ePLND) are the gold standard treatment for muscle-invasive bladder cancer and BCG unresponsive nonmuscle-invasive bladder cancer. In this article, we review the rationale for ePLND in the treatment of bladder cancer and the evidence supporting the equipoise between robot-assisted (RA) and open ePLND. A step-by-step guide of robot-assisted ePLND (RA ePLND) is provided to illustrate the techniques currently employed at our institution.
Materials and Methods:
Medline and PubMed electronic databases were queried for English language articles on bladder cancer, ePLND, and RA ePLND. In addition, a step-by-step video of RA ePLND was assembled with narration and accompanying explanations of each step to illustrate our current techniques. Key images from the video were selected for illustration of the relevant anatomical landmarks.
Results:
ePLND with a minimum nodal yield of 10 to 14 is tantamount in the treatment of bladder cancer. The number of lymph nodes resected influenced survival in both pathologically node positive and negative patients. In addition, RA ePLND was found to have equipoise as open ePLND by several groups. In our surgical atlas video, we illustrate key surgical steps, including port placement and exposure. Also, anatomic landmarks of dissection for the internal iliac, external iliac/obturator, and higher nodal packets are described in detail.
Conclusions:
We illustrate the techniques for a thorough RA ePLND, with the intention to help the robotic surgeon to meet the 10 to 14 nodal yield mandated by the Bladder Cancer Collaborative Group.
Rationale and Indications
Radical cystectomy (RC) and extended pelvic lymph node dissection (ePLND) are the gold standard treatment for muscle-invasive bladder cancer and high-grade nonmuscle-invasive bladder cancer after failure of intravesical therapy. 1 ePLND not only provides valuable prognostic information but has also been shown to confer clinically significant therapeutic benefit. 2 Furthermore, the quality of the PLND, as measured by the number of nodes retrieved, is directly linked to postsurgical survival.
In a large cystectomy series from Europe, Leissner et al. found significant correlation between the number of lymph nodes (LN) resected and 5-year recurrence-free survival in pT1–3 patients, as well as those with 1 to 5 metastatic LN. 3 Similar findings were mirrored in another North American study by Herr et al., who found improvement in survival in both pathologically node-positive and node-negative patients with increased nodal retrieval. 4 A corollary finding in SWOG 8710 was the paramount importance of surgical factors (including PLND quality) in influencing bladder cancer outcomes. In a secondary analysis, Herr and colleagues pinpointed 10 nodes as the minimum requirement for conferring higher recurrence-free survival and overall survival in pN0 and pN1 patients. 5 Using data from two large comprehensive cancer centers, Kassouf and colleagues found lymph node density (LND) to be the best prognostic metric. 6 LND improves upon pathologic nodal staging as it not only accounts for positive LN metastasis but also reflects the quality of the PLND. For example, two patients with a single positive LN would both be classified as pN1 according to the eighth edition of the AJCC Cancer Staging System. However, the prognosis may be different given a poorly performed PLND yielding a single node vs a good-quality PLND yielding 20 nodes. Although the patient with 1/1 positive LN may harbor unresected metastatic LN, this is unlikely in the patient with 20 LN dissected. 7 In addition, thorough PLND may also eradicate micrometastatic disease, which may impair post-RC survival.
Despite the compelling evidence from the retrospective studies, the benefit of ePLND will only be elucidated by the results from the ongoing Phase III SWOG S1011 trial, in which survival is compared in patients subjected to ePLND vs standard PLND at the time of RC. Nevertheless, the Bladder Cancer Collaborative Group proposed using LN yield of 10 to 14 as a metric for quality RC. 8 With that in mind, this step-by-step visual atlas aims to provide the necessary guidance for all robotic surgeons performing robot-assisted radical cystectomy (RARC) to achieve this standard.
Equipoise of robot-assisted ePLND
Early on, many experts questioned the ability of robot-assisted ePLND (RA ePLND) to replicate the quality and extent of open ePLND. 9 Given the importance of adequate nodal dissection in the control of bladder cancer, robotic or laparoscopic surgery for bladder cancer was relegated to surgical research. Indeed, the suboptimal reach of the original da Vinci® surgical system (Sunnyvale, CA) impaired cephalad nodal dissection. Improvements in later iterations, as well as adjustments in port placement, have been used to overcome this barrier. 10,11
In 2011, Davis and coworkers allayed concerns regarding RA ePLND's equipoise with a study examining the incremental nodal yield from a “second-look” open ePLND after RA ePLND was performed. 1 In this study, open ePLND yielded a minimal increment of 7% to the nodal yield. Importantly, none of the additional LN found on open ePLND harbored metastatic disease. The authors concluded that RA ePLND is capable of complete PLND. Another group came to the same conclusion in a study of 15 patients undergoing RARC and ePLND, with a mean (range) nodal yield of 41.8 (18–67). 12 These results have since been corroborated by other retrospective studies, 13 –16 a prospective randomized controlled trial, 17 as well as meta-analysis of these studies. 10
Several open radical cystectomy (ORC) series have demonstrated comparable incidences of postoperative complications, including lymphocele formation, lymphedema, and mortality rates, in RC with or without ePLND. 3,18,19 In 2015, the much anticipated prospective randomized trial comparing RARC vs ORC also showed similar short-term complication rates. 17 Although no study has specifically assessed the incremental increase in morbidity from RA ePLND, it can be inferred that RA ePLND adds little morbidity to RARC.
Because of its recent adoption, few studies have examined the equipoise of RARC in terms of oncologic outcomes. Furthermore, any comparison between RARC and ORC should be made with the understanding that the quality of the ePLND is but one of two surgical factors affecting oncologic outcomes. Surgical margin status has been established to be equally important. 5 With this in mind, Mmeje et al. studied the outcomes of 50 RARC patients with pathologic LN metastasis 20 and found similar 5-year recurrence-free survival rates as described in several notable ORC series. 21,22 Ultimately, results from the randomized open vs robotic cystectomy (RAZOR) study are awaited to be the final arbiter of whether similar oncologic outcomes can be achieved. 23
Preoperative Preparation
Akin to the preparation for any major intra-abdominal surgery, appropriate preoperative evaluation for general fitness, cognition, cardiopulmonary function, renal function, immune function, allergy status, current medications, and smoking status needs to be established before RARC. In addition, the preoperative assessment of patients undergoing RARC needs to also account for the patients' ability to tolerate prolonged pneumoperitoneum and steep Trendelenburg position. Specific unfavorable factors for RA ePLND include high body mass index, positive examination under anesthesia indicating locally advanced disease status, bulky lymphadenopathy on imaging, previous vascular surgery, previous pelvic radiation, previous colorectal surgery, or previous history of pelvic trauma.
Positioning
Surgical team positioning
In our practice, the bedside assistant stands on the patient's right, whereas the third robotic arm is placed on the patient's left side. However, if a robotic urinary diversion is planned, the third arm/assistant is reversed, such that a left side assistant has an ideal angle for Endo-GIA stapling. The scrub nurse and the surgical instrument table are both placed on the side of the surgical assistant to facilitate instrument exchange. Console surgeon has ready access to the operating table so that he can scrub into the procedure at a moment's notice.
Patient positioning
Standard egg crate foam padding is used on the surgical bed to prevent the patient from sliding. The patient is placed in dorsal lithotomy position using standard operative stirrups. Bilateral sleds are used for tucking of the arms. All pressure points are protected using egg crate foam paddings. Paddings are also applied over the face, hands, and any other areas in close contact with the robotic instrument to protect against inadvertent instrument collisions during the procedure. An orogastric tube is placed by the anesthesia team and connected to low wall suction for the duration of the surgery. Once the patient is secured, the surgical bed is tilted to a 25° steep Trendelenburg position. The da Vinci Surgical System Si is docked between the patient's legs, although more liberal positioning of the da Vinci Surgical System Xi can be used, including a side-dock position.
Surgical Steps
Port placement
As mentioned previously, adjusted port placement is used to overcome the shortfall in cephalad reach. The camera port is placed 5 cm above the umbilicus. Instead of the usual two fingerbreadths above the anterior superior iliac spine (ASIS), the robotic third arm is placed three to four fingerbreadths (6–8 cm) above the right ASIS (if robotic urinary diversion is anticipated). The more cephalad placement allows higher retraction and provides additional room for the first and second arms to maneuver beneath. The first and second robotic arms are placed at the level of the umbilicus, approximately one-hand breadth lateral to midline at the edge of the rectus muscle. Two additional 12 mm assistant ports are used. One is placed 2 cm above the left ASIS. Another is placed superomedially, 3 cm below the right costal margin, directly traversing the rectus muscle. Curved monopolar scissors and the Maryland dissector are used on the right and left robotic arms, respectively.
Sequence of RA ePLND and cystectomy
The sequence of RA ePLND and cystectomy during RARC had been a topic of debate. 24 Proponents for prioritizing RA ePLND claim that as the most important and technically challenging part of the procedure, ePLND should be performed early on during the long procedure. In addition, the intact umbilical artery can be used as guide to finding the internal iliac vessels. The ePLND also exposes the vascular pedicles, setting up for an easy resection of the bladder. 24 On the other hand, removing the bladder first provides a more capacious surgical field to work in. We select the sequence of RA ePLND and cystectomy according to each patient's unique anatomy, although the ePLND-first technique is preferred as this helps to better set up the planes of dissection.
Exposure
Video 1 illustrates the landmarks used during the exposure and the internal iliac nodal dissection. First, the sigmoid colon is dissected free and rotated out of the surgical field. If the bladder is left intact, the anterior peritoneum is incised parallel to the umbilical ligaments from just lateral to the urachus, continuing to the bilateral vasa deferentia. The vasa deferentia and the accompanying deferential artery are sealed with bipolar energy and divided. Over the retroperitoneum, lateral incisions are made cephalad to the level at which the ureters cross over the iliac vessels, exposing the takeoff to the external iliac artery and the ureter (Fig. 1). Dissection of this plane is carried down, exposing the psoas muscle and the genitofemoral nerve (Fig. 2). If still intact, the urachus is then grasped using the third arm and pulled contralateral to the side of PLND. Simultaneously, the assistant can grasp the medial exposed edge of the retroperitoneum, enhancing the exposure of the pelvic nodal region.
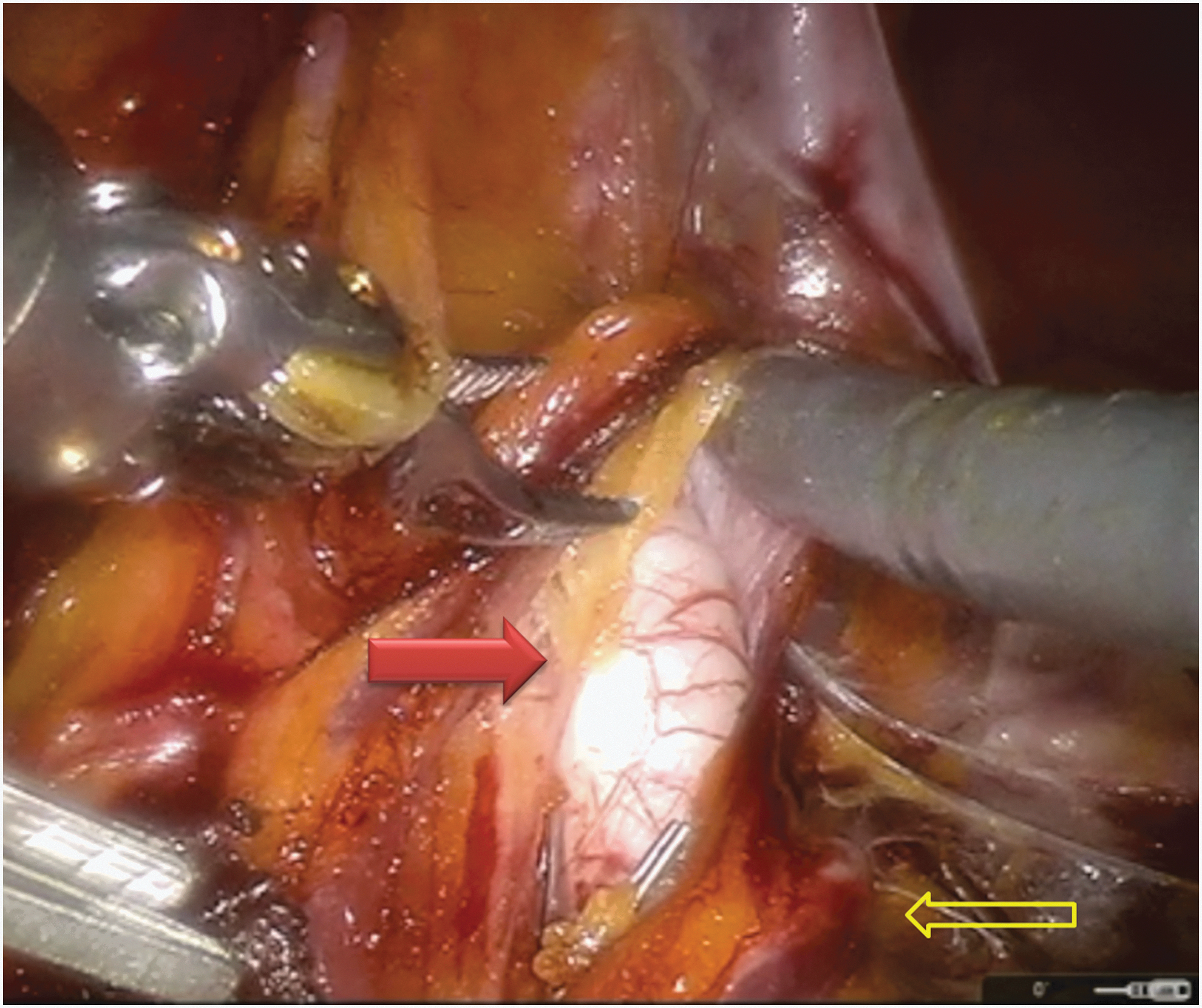
The retroperitoneum is incised lateral to the left external iliac artery (solid arrow), exposing the crossing of the ureter (open arrow) (Video 1: Mobilization of the colon and creation of the dissection planes around the pelvic vessels, 01:50).

Dissection lateral to the right iliac artery is carried down to the psoas muscle, exposing the genitofemoral nerve (open arrow) (Video 1, 03:17).
Internal iliac nodes
LN dissection is carried out over the internal iliac region, where the nodal tissue is the most difficult to reach. Starting from the ureteral crossing of the iliac artery, dissection proceeds caudally along the course of the internal iliac artery until the takeoff of the obliterated umbilical artery. This artery is transected at this time (Fig. 3) and dissection is carried further inferiorly, enabling visualization of the distal path of the internal iliac artery. Next, attention is turned to the perivesical fat 3 to 4 cm away from the takeoff of the obliterated umbilical artery, medial to the ureter (Fig. 4). A vague, but reproducible, plane can be developed here using gentle sweeping motions directed distally a few millimeters underneath the surface. Adequate tension on the urachus is key to facilitate this dissection. Once developed, this perivesical plane is extended distally toward the endopelvic fascia, ending in a pocket of perirectal fat. In addition, the plane is also extended superolaterally toward the obturator fossa beneath the obturator nerve. Finally, tissue interjecting the two developed planes is freed. The entire nodal packet is delivered into the obturator fossa and retrieved using Anchor™ Tissue Retrieval bag (Addison, IL).

Dissection over the right internal iliac artery (solid arrow) is carried caudally from the crossing of the ureter (open arrow). The obliterated umbilical artery (arrowhead) is identified and clipped (Video 1, 04:03).

Developing the perivesical space (solid arrow) medial to the cut end of the obliterated umbilical artery (arrowhead) (Video 1, 04:42).
Using this method, ∼70% to 80% of the nodal tissue over the internal iliac vessels can be retrieved. However, retrieval of nodal packets in several difficult-to-reach locations requires a second-look dissection. These include spaces between internal iliac sub-branches, beneath the obturator nerve, superomedial to the takeoff of the obliterated umbilical artery, and underneath the takeoff of the obliterated umbilical artery (Fig. 5).

A complete nodal dissection, with nodal tissue cleared from the external iliac zone (1), the obturator zone (2, 3), and the internal iliac zone (4). Regions of difficult to dissect nodal tissue are denoted (5). These include the spaces between the internal iliac sub-branches, as well as spaces superomedial to and underneath the takeoff of the obliterated umbilical artery (adopted from Williams et al. 11 ).
External iliac/obturator fossa
Video 2 illustrates the nodal dissection over the external iliac vessels. Unlike the ePLND performed in the treatment of prostate cancer, dissection of the nodal tissue is carried lateral to the external iliac vein to the genitofemoral nerve (Fig. 2). A particularly hard-to-reach area is the triangle of Marseille, which is accessed by separating the fascia between the external iliac artery and vein, and gently pulling the vein medially. Nodal tissue is freed from the psoas muscle. At the end of the dissection, the obturator nerve should be visualized through the gap between the external iliac vein and artery (Fig. 6). The packet is then delivered into the obturator fossa, and the nodal tissue herein is dissected to the “floor” of vascular tissue from the internal iliac vessels (Fig. 7). Care should be taken to not dig deeply toward the sacrum as the sacral nerves are in close proximity and can easily be injured, leading to postoperative neuropathy. The nodal packet is again retrieved by reusing the same Anchor Tissue Retrieval bag (Addison, IL).

The left external iliac vein (blue arrow) is retracted medially, exposing the triangle of Marseille. With complete nodal dissection, the obturator nerve (blue arrowhead) as well as the psoas muscle (red arrowhead) should be visualized through the window between the iliac artery (red arrow) and vein (Video 2: Dissection of the external iliac, obturator, internal iliac and common iliac nodal packets, 02:41).
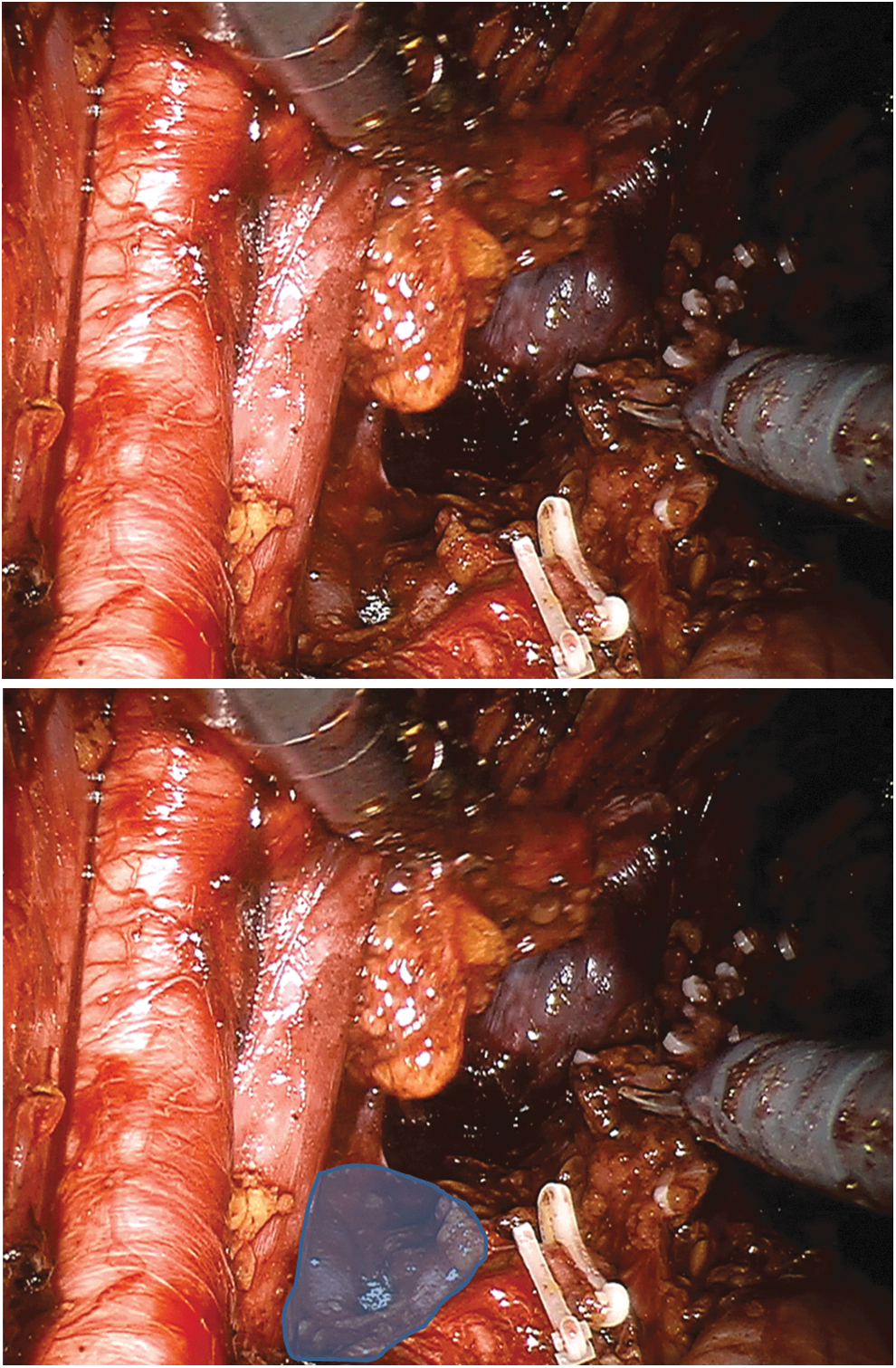
Nodal tissue removed from the floor of the dissection composed of vascular tissue from the internal iliac vessel (shaded region). The surgeon should note that sacral nerves lay in close proximity, thus taking care not to dissect deep to the marked plane (Video 2, 03:22).
Higher planes
Video 3 illustrates dissection of the higher planes cephalad to the crossing of the ureters over the common iliac arteries. This is performed in patients at high risk for nodal metastases, in whom the dissection may be extended as high as the inferior mesenteric artery (Fig. 8). Dissection commences over the right common iliac artery, proceeds to the aortic bifurcation, and terminates over the left common iliac artery. Using the ProGrasp in the third arm, the colon is hyper-rotated off the plane of dissection and pushed contralateral to the side of dissection. The presacral zone in between the common iliac artery is cleared. Caution is exercised to prevent injury to the left common iliac vein (Video 3). Upon reaching the bifurcation, the ProGrasp is adjusted to expose the plane of dissection over the right common iliac artery. Adequate exposure must be obtained to access the para-aortic nodal tissue, as well as to facilitate transposing the left ureter through the sigmoid mesentery.

Exposure extended to the inferior mesenteric artery (red arrow). Blue arrow denotes the aortic bifurcation (Video 3: Dissection of the paraaortic, interaortocaval, paracaval, presacral and proximal common iliac nodal packets, 02:33).
Tricks of the trade
To prevent lymphoceles, attempts are made to seal the proximal and distal severed lymphatic vessels using surgical clips. Proximally, Hem-o-lok® clips (Teleflex, Morrisville, NC) are applied at the lymphatic division lines near the branch point of the internal and external iliac arteries from the common iliac artery. Distally, clips are placed distal to the node of Cloquet. Additional clips are placed in the triangular space underneath the external iliac artery. Where lymphatic vessels retract out of view, making clipping impossible, bipolar sealing can be liberally used. We do not routinely use hemostatic agents for lymphocele prophylaxis. However, Fibrillar® product (Ethicon, Somerville, NJ) can be used to enhance hemostasis.
LN tissue should be passed off as separate packets designated internal iliac, external iliac/obturator, and common iliac for either side, along with preaortic and presacral nodes. Our preferred produce is the Anchor Tissue Retrieval system—a reusable bag to keep the nodes organized into subpackets. Finally, a Jackson-Pratt drain is left in the pelvis.
Postoperative Care
Postoperatively, compression stockings and sequential compression devices are applied to the lower extremities. In addition, physical therapy is ordered to encourage early ambulation. Jackson-Pratt drain output is closely monitored. Drains are removed when output is less than 100 mL per 8 hours for 24 hours. In case this is not achieved by discharge, the drain will be placed to gravity and further management continued on an outpatient basis.
Troubleshooting
In select cases, redundant sigmoid colon or cecum obstructs access to the surgical field and needs to be dissected free and moved cephalad. If this is inadequate, externalized sutures can be used to retract the urachus contralateral to the field of dissection, while freeing up the third arm to retract the obstructing bowel.
Untreated hernias need to be reduced to provide complete access to the surgical field. In case a prior hernia mesh is encountered, sharp dissection of the mesh is sometimes needed to free up the nodal tissue for extraction.
Video 3 illustrates repair of an inadvertent vascular injury. Ideally, proximal vascular control is obtained before repair. However, in cases where vascular control is not feasible, repair may proceed with adequate exposure and site of injury being clearly identified. Pledgets can be used to prevent bleeding from the needle passage holes. Floseal (Baxter, Houston, TX) is used to reinforce the repair site.
Recommended Videos from Videourology
Pelvic Lymph Node Dissection in Laparoscopic Radical Cystectomy: Three-Year Results Kan Raymond Wai-Man, Kan Chi-Fai, Ngai Ho-Yin, Hung Hing-Hoi, Ho Lap-Yin, Chan Steve Wai-Hee, and Au Wing-Hang
2014;28:DOI: 10.1089/vid.2013.0106
Laparoscopic Extended Pelvic Lymph Node Dissection During Radical Cystectomy: Technique and Outcomes
Jairath Ankush, S Balaji Sudharsan, Mishra Shashikant, Sabnis Ravindra, and Desai Mahesh
2015;29:DOI: 10.1089/vid.2014.0057
Footnotes
Author Disclosure Statement
No competing financial interests exist.