
Abstract
The incidence of symptomatic benign prostate hyperplasia and bladder outlet obstruction has increased during the last two decades. Most of men are treated conservatively. When medical therapy is inadequate to relief symptoms, surgical treatment is necessary. Absolute indications for surgical treatment are gross hematuria, recurrent urinary infections and retentions as well as bladder stones. With advent of minimally invasive surgery, large prostates tend to be treated either endoscopically or laparoscopically (including robotic assistance). Herein, the robotic-assisted simple prostatectomy is described.
Indications
Symptomatic benign prostatic hyperplasia (BPH) is surgically treated according to specific indications. The absolute indications include recurrent or refractory urinary retention; incontinence due to overflow; recurrent urinary tract infections, stones, or diverticula of the bladder; refractory gross hematuria due to prostatic hyperplasia; and dilatation of the renal collecting system related to the condition. Similarly, insufficient symptom relief and persistent postmicturition residual urine volume (PVR) despite medication are relative indications for surgical treatment. Selection criterion for the surgical method is the volume of the prostate gland. For glands <80 cc, the method of choice is the transurethral prostatectomy. Open simple prostatectomy (OSP) is recommended for prostates >80–100 cc. 1 For decades, the OSP was the gold standard for the management of BPH. Basic technical approaches are the retropubic OSP, which is performed by a transverse capsular incision (Millin procedure). The suprapubic prostatectomy is performed by a vesicocapsular incision (Freyer's procedure) while the procedure could be done only with a longitudinal bladder incision (modified Freyer's procedure). In an attempt to reduce complications and morbidity, minimally invasive methods (laparoscopic and robot-assisted prostatectomy) were introduced for the management of BPH. The dissemination of robotic surgery in urology has allowed the urologists to simulate the open surgery and to apply the same methods of open surgery in a minimally invasive manner. 2 We, herein, describe the technique of robot-assisted simple prostatectomy (RASP).
Preoperative Preparation
Patients who are candidates for RASP undergo clinical and imaging examinations. The digital rectal examination and the PSA measurement always precede surgery. In cases of high PSA, patients are further investigated to exclude prostate cancer. Uroflowmetry is routinely performed, whereas a complete urodynamics evaluation is considered according to clinical indications. Urinalysis and urine cultures are also routine investigations. On the admission day, an abdominal ultrasound, including the PVR takes place in patients without an indwelling Foley catheter. 3
Preoperatively, any anticoagulants are discontinued and the day before surgery a complete blood count, a chemistry panel, and coagulation studies are performed. Typed and cross-matched blood products are available for intraoperative or postoperative transfusion. Within 1 hour before the incision, a second-generation cephalosporin is intravenously administered in uncomplicated cases. Patients with prosthetics or an indwelling Foley catheter are managed with the administration of broad-spectrum antibiotics. 3
Patient Positioning
The patient is set to supine position with his legs abducted. A Trendelenburg angle of 10–15° is sufficient for the extraperitoneal approach and allows extension of the operation time without cardiopulmonary restrictions (Fig. 1A). An intraperitoneal approach would require a steeper Trendelenburg angle of 20–25°.

Surgical Steps
Development of extraperitoneal space and trocar placement
Development of the extraperitoneal space
The skin is incised (15 mm incision) about 1 cm below and laterally right of the umbilicus (right paraumbilical incision). Blunt dissection is performed to the level of the anterior rectus sheath. The anterior rectus sheath is incised horizontally and the opening is enlarged, while the muscle fibers are dissected and the posterior rectus muscle sheath is visible. With the surgeon's finger, the space between the posterior rectus sheath and the rectus muscle is bluntly developed toward the preperitoneal space. Then, a balloon trocar is placed through the incision and under visual control it is insufflated. The preperitoneal space is prepared and the appropriate landmarks for orientation are the pubic arch and the epigastric vessels. The balloon trocar is deflated and removed. Stay sutures are placed on the anterior rectus sheath and the optical trocar (Hasson 10 mm trocar) is introduced.
Trocar placement
(Fig. 1B) An 8 mm robotic trocar is inserted four fingertips laterally and to the left of the midline of the hypothetical line between the pubic arch and the umbilicus. Then, a 12 mm conventional laparoscopic trocar is placed two fingers medially to the right anterior superior iliac spine. The cephalad insertion site depends on the free edge of peritoneum. This trocar is usually used by the assistant so that he can perform the suction, apply clips, and insert and extract sutures and needles. An 8 mm robotic trocar is inserted about five fingers on the right of a hypothetical line that links the umbilicus with the anterior superior iliac spine. Finally, another 8 mm trocar is placed three fingers medially to the left anterior superior iliac spine on the same hypothetical line as previously described, but on the left side of the patient. A sixth 5 mm port could also be inserted if it is deemed necessary by the surgeon. Robot docking follows with two robotic instruments at each side of the patient. The instruments that are used are Large Needle Driver, a Hot Shear™ (Monopolar Curved Scissors), a ProGrasp™ Forceps, and a Fenestrated Bipolar Forceps. The surgeon uses the Bipolar or ProGrasp forceps through the left robotic trocars and the Needle Driver with the Curved scissors through the right trocar.
Cystotomy incision
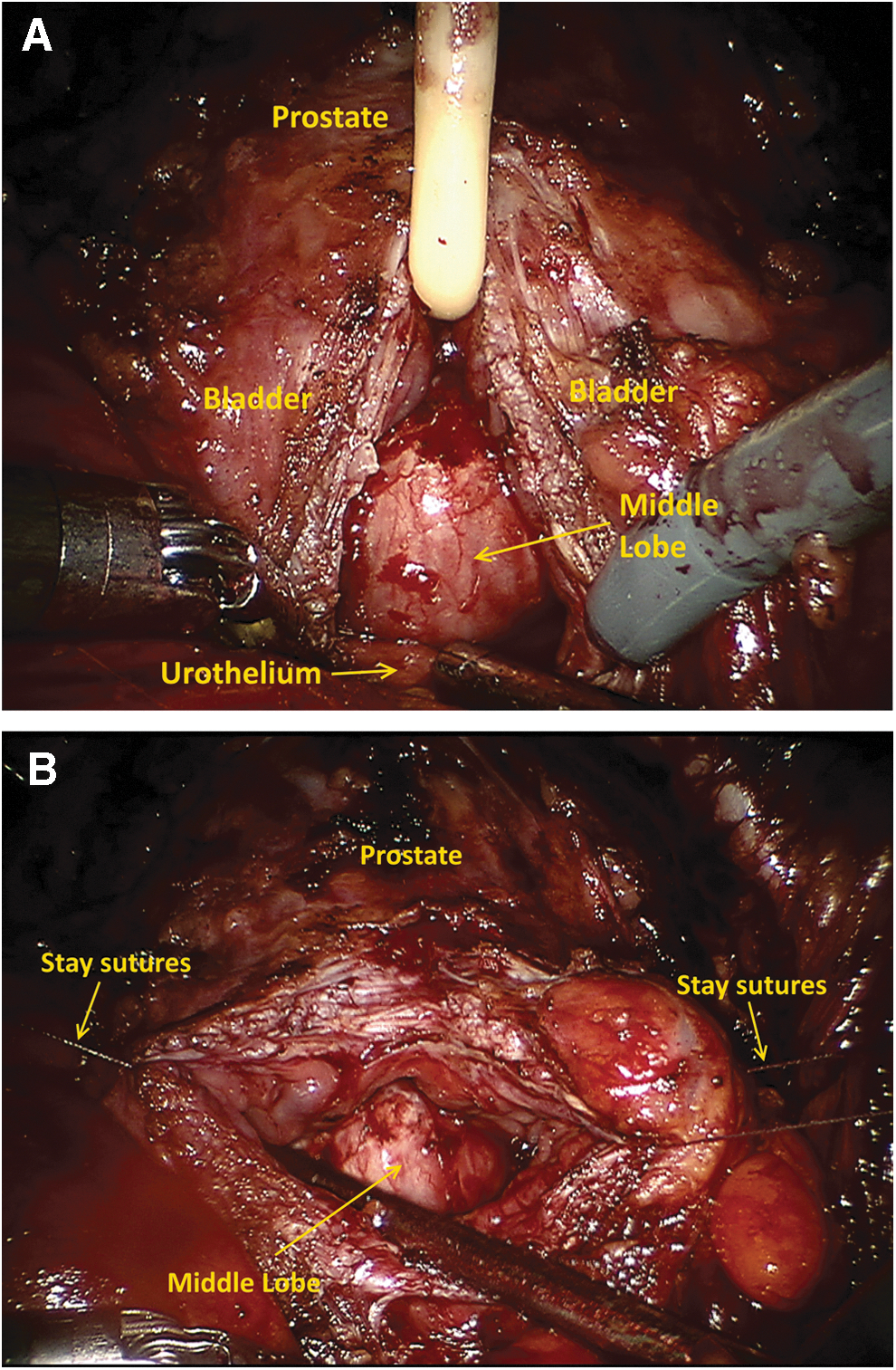
The overlying fat is being dissected exposing adequately the anterior bladder wall. A cystotomy incision is made longitudinally from the anterior bladder wall to the bladder neck with robotic scissors. Then, this incision is extended about 2 cm over the anterior bladder wall and about 2 cm over the capsule of the prostate Fig. 2A. The bladder wall is retracted with sutures on the ipsilateral abdominal wall and the cystotomy remains open during the operation Fig. 2B. At this point, the prostatic adenoma is seen from the exposed bladder neck, while the ureteral orifices are identified.
Enucleation of the adenoma
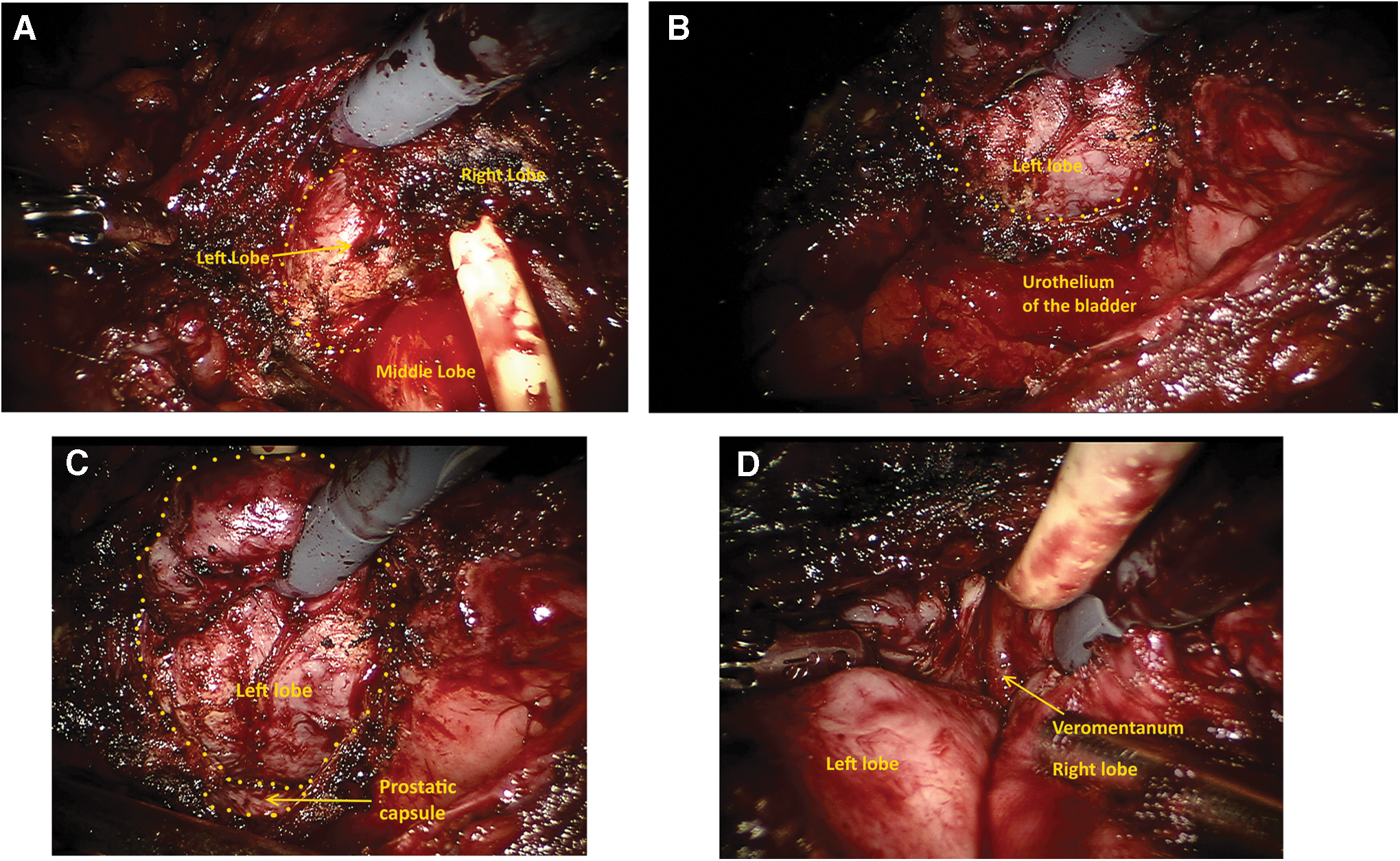
Ligating the dorsal venous complex (DVC) is not always required. An incision of the mucosa around the limits of the prostatic adenoma is circumferentially performed with the robotic monopolar scissors and the place between the prostatic capsule and the adenoma is gradually developed. The incision begins at 10 or 2 o'clock positions (for the left and the right side, respectively) and is extended circumferentially with blunt and sharp dissection and also bipolar coagulation. The surgeon should pay attention to the correct plane as it is relatively avascular. The dissection of the lobes is carefully performed and ends at the prostate apex. The margin of dissection is carefully directed over the adenoma in an attempt to maximize the length of the urethra and to preserve the external urethral sphincter without damaging it Fig. 3(A–C). By identifying the verumontanum, the safety of the urethral sphincter is ascertained. The excision of one of the lobes initially and then the removal of the other facilitates the dissection Fig. 3(D). En bloc excision is possible, but could also be challenging. If a large middle lobe exists, it can be carefully dissected first by grasping the lobe and taking care of not injuring the ureteral orifices. The use of the bipolar coagulation achieves a bloodless surgical field Fig. 4. Nevertheless, it should not be used at the apex, where it could injure the external sphincter. Finally, the adenoma is removed in an endoscopic specimen bag.
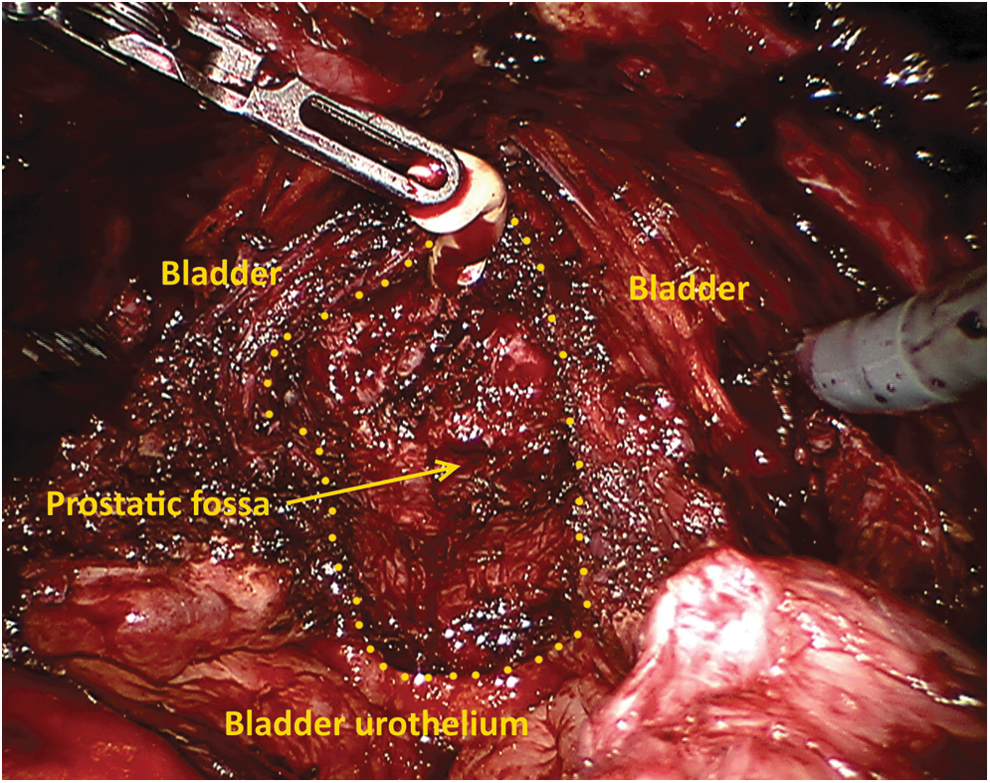
The adenoma has been excised and the prostatic fossa (dotted line) is visible. Notice the lack of any significant bleeding and that no hemostatic sutures are necessary.
Hemostasis and bladder closure
Any bleeding vessels within the prostatic fossa must be accomplished by cauterization with the bipolar diathermy. Sutures at 5 and 7 o'clock positions of the prostatic capsule might be required (2-0 Vicryl suture with UR-6 needle). Sutures are placed to the posterior bladder urothelium deep in the prostatic fossa near the urethra, so that the bladder neck is trigonized. This facilitates the indwelling catheter placement as it smoothens the posterior contour avoiding the “step” between the bladder and prostatic fossa. A three-way indwelling Foley catheter is then inserted and the bladder incision is closed by running 3-0 Vicryl (UR-6 needle) or a 3-0 V-loc (Covidien, New Haven, CT) suture. It is recommended that the bladder is closed in two layers. The second layer could be either running or interrupted suturing. The sutured incision is checked for leakage by filling the bladder with 200 mL sterile water through the indwelling Foley catheter.
Specimen retrieval
A drain is inserted through the left 8 mm trocar and set behind to the pubic arch. The endobag with the adenoma is removed through the incision of the 12 mm trocar, which can be elongated according to the size of the specimen. Finally, the incisions are closed step by step until the skin closure.
Postoperative Care
The patient's vital signs should be monitored postoperatively. The patency of the indwelling Foley catheter should be often checked. The patient has continuous bladder irrigation until macroscopic hematuria ceases. The removal of the drainage takes place on the first or second postoperative day, whereas the catheter is removed the sixth day after a cystography. 3
Troubleshooting
Previous studies, including >160 cases of simple robotic prostatectomy, referred to low complication rates. 3 –15 Perioperative transfusions are encountered with a low incidence, whereas only two cases have been converted to open. 10,15 Two cases of urine leakage, a patient with umbilical hernia and a patient with narrowing of the bladder neck have been reported in the literature. 8,11,14 One case has been related to severe urinary incontinence. 11
Ligating the DVC is not always required, except the cases of troublesome bleeding of the anterior prostatic surface when the plexus is ligated with a 2-0 Vicryl suture (MH plus needle) underneath from right to left. Another important detail is that the adenoma is not removed en bloc, but each lobe is subtracted separately. If a large middle lobe exists, it can be carefully dissected first by grasping the lobe taking care of not injuring the ureteral orifices. The dissection of the lateral lobes follows. 3
The experience with the extraperitoneal approach for endoscopic radical prostatectomy showed that the inferior epigastric vessels represent one of the most common sites of bleeding. 16 Careful inspection of the inner abdominal wall with the use of the endoscopic camera before insertion of trocars is important for the prevention of any injury to the epigastric vessels. Prepuncture of the site intended for trocar placement with the use of a fine needle is helpful in the visualization of the site. A laparoscopic grasper could be used to point from the inner side of the abdominal wall a site of trocar puncture away from the epigastric vessels. An incision could be made right over the grasper and the trocar could be inserted. Bipolar coagulation and clipping are adequate for controlling any bleeding of the epigastric vessels. In case of failure of these manipulations, a straight needle is passed through the abdominal wall, around the bleeding epigastric vessel, and suture is tied outside the abdomen on the abdominal wall. The suture can be removed with safety on the second postoperative day.
Footnotes
Supplementary Videos
Click here for Supplementary Videos: 1. Patient positioning and trocar placement.mp4; 2. Cystotomy.mp4; 3. Enucleation of the adenoma.mp4; 4. Hemostasis and Baldder closure.mp4
Author Disclosure Statement
No competing financial interests exist.