
Abstract
Neurogenic bladder occur as a consequence of several conditions, most commonly posterior urethral valves syndrome, spina bifida, tethered cord, sacral agenesis, and Arnold-Chiari malformation. It is characterized by diminished bladder capacity and/or reduced compliance, associated with high-pressure voiding that can lead to deterioration of renal function if left untreated. When medical management fails, bladder reconstruction with bowel (aumentation ileocystoplasty) becomes the treatment of choice for these patients. In most cases, it is accompanied by the creation of a continent catheterizable channel, with the appendix being the most commonly used conduit (Mitrofanoff appendicovesicostomy). Conventional open surgery has proven to be an efficient and safe approach in these patients. However, robot-assisted surgery not only offers a cosmetic advantage, but also results in a shorter hospital stay, less postoperative pain, and even decreased number of adhesions (as shown in porcine models). Nevertheless, the complexity of this technique has limited the wide adoption of this approach. We seek to provide a technical guide to robot-assisted laparoscopic ileocystoplasty and Mitrofanoff appendicovesicostomy in pediatric patients, as well as a critical review of literature about the perioperative care of these patients.
Introduction
Bladder reconstruction with bowel (augmentation ileocystoplasty) is the treatment of choice for patients with neurogenic bladder that failed medical management. Impaired bladder function leads to a diminished bladder capacity and/or reduced compliance, associated with high-pressure voiding. If not corrected, chronic high-pressure voiding could cause deterioration of renal function. The underlying abnormalities that account for this dysfunction are most commonly posterior urethral valves (PUV) syndrome, spina bifida, tethered cord, sacral agenesis, and Arnold-Chiari malformation. 1,2
In the vast majority of cases, an augmentation ileocystoplasty is accompanied by the creation of a continent catheterizable channel (CCC). The augmentation results in an increase in bladder capacity and compliance, as well as a decrease in voiding pressures, whereas the CCC allows the patient to achieve social continence and avoid the need of urethral catheterization, which can lead to discomfort in a sensitive urethra, or complications like trauma, stricture formation, and ultimately noncompliance. 1,2 The appendix is the most commonly used conduit for a CCC (Mitrofanoff appendicovesicostomy), but others prefer using a transversely tubularized bowel segment as a channel (Yang-Monti technique). Less popular, but also described alternatives for urinary conduits, are the fallopian tubes, ureter, and tubularized colonic or bladder flaps. 3
Conventional open surgical approach for augmentation ileocystoplasty, with or without appendicovesicostomy, has proven to be an efficient and safe approach for these patients. Nevertheless, since robot-assisted laparoscopic (RAL) surgery was introduced as a feasible technique for this procedure, more pediatric urologists are favoring this approach, although its high complexity has limited the wide adoption of this technique. Robot-assisted surgery not only offers a cosmetic advantage by avoiding a large midline or Pfannenstiel incision, but also results in a shorter hospital stay and less postoperative pain. In addition, the postoperative recovery and pain management are particularly challenging in patients with poor lung reserve secondary to kyphoscoliosis, so a minimally invasive approach is favored in these cases. Finally, we showed that in a porcine model of RAL ileocystoplasty, the number of adhesions was lower compared to open approaches, which decreases the risk of postoperative small bowel obstruction in this vulnerable group of patients who will probably need multiple surgeries in the future. 4
In this review, we will provide a technical guide to robot-assisted laparoscopic ileocystoplasty and Mitrofanoff appendicovesicostomy (RALIMA) in pediatric patients based on our experience, a critical summary of some of the current literature regarding the surgical indications, procedure and postoperative care and follow-up, and a summary of our published interim results with this technique.
Indications and Contraindications
An augmentation ileocystoplasty is indicated in patients with neurogenic bladder if they fail medical management, have severe hydronephrosis, and/or if concerning urodynamic parameters are present (unstable detrusor contractions, reduced bladder compliance, and detrusor leak point pressure ≥40 cm H2O). The most common underlying conditions that lead to an augmentation ileocystoplasty are posterior urethral valve syndrome, spina bifida, tethered cord, sacral agenesis, and Arnold-Chiari malformation. 1,2 The decision for performing a Mitrofanoff appendicovesicostomy (or another type of CCC) is centered on patient/family preferences and difficulties encountered while doing clean intermittent catheterization (CIC) through the native urethra. 5 Other causes of bladder dysfunction, such as nonneurogenic neurogenic bladder and Prune Belly syndrome, are usually managed with an isolated CCC.
There are absolute and relative contraindications for performing a RAL augmentation ileocystoplasty. Absolute contraindications include inability to perform catheterization and poor access to caregivers. On the other hand, relative contraindications include inflammatory bowel disease, short or irradiated bowel, and significant renal impairment, although a recent study reported no decline in renal function secondary to augmentation ileocystoplasty in children with chronic kidney disease and neurogenic bladder. 6
Specific to the robotic approach, having a history of multiple abdominal surgeries and/or severe kyphoscoliosis increases the likelihood of conversion to open surgery. Although exceptions may happen, we recommend this approach for children older than 6 years of age, without multiple prior abdominal surgeries, severe kyphoscoliosis, and/or an underlying severe illness that would affect positioning and surgery duration (Fig. 1). If the patient had a prior appendectomy, we recommend performing a CCC with small bowel with an open approach, since it may be difficult to accomplish this robotically early in the learning curve for RAL surgery. (see Supplementary Videos S1 and S2; Supplementary Data available online at

Indications for RALIMA and limitations. RALIMA = robot-assisted laparoscopic ileocystoplasty and Mitrofanoff appendicovesicostomy. PUV = Posterior urethral valves.
Preoperative Preparation
Preoperative evaluation consists of urodynamics, renal ultrasound (RUS), and DMSA renal scan. By performing videourodynamics, we assess bladder function and bladder neck competency. The RUS and renal scan are aimed to evaluate the kidneys both anatomically and functionally. A voiding cystourethrogram is performed as necessary to evaluate for secondary vesicoureteral reflux (VUR), although if present, we prefer to not treat the VUR, as it is immediately as it is highly likely to self-resolve due to the diminished pressure of the newly augmented bladder.
We admit the patient the same day of the surgery, without previous bowel preparation or prophylaxis with oral antibiotics. 7 We also do a urine culture preoperatively, as it is important to treat any concomitant urinary tract infection before undergoing surgery. Prophylactic antibiotics are administered intravenously within 1 hour of incision to all patients; our institutional protocols consist of cefazolin, gentamicin, and metronidazole (unless allergies are present). 1 If the patient has a ventriculoperitoneal (VP) shunt in place, we recommend using vancomycin instead of cefazolin. 8
It is imperative that both the patient and caregivers are properly educated about the surgery and postoperative care. With the help of the nurse practitioner, we teach the patient and family the importance of CIC to empty the bladder periodically. We also give the option to the patient to choose between an umbilical or right iliac fossa appendicovesicostomy. Answering all the questions and thoroughly counseling the patient and family about their condition and care, facilitates postoperative compliance and improves outcomes (Fig. 2).
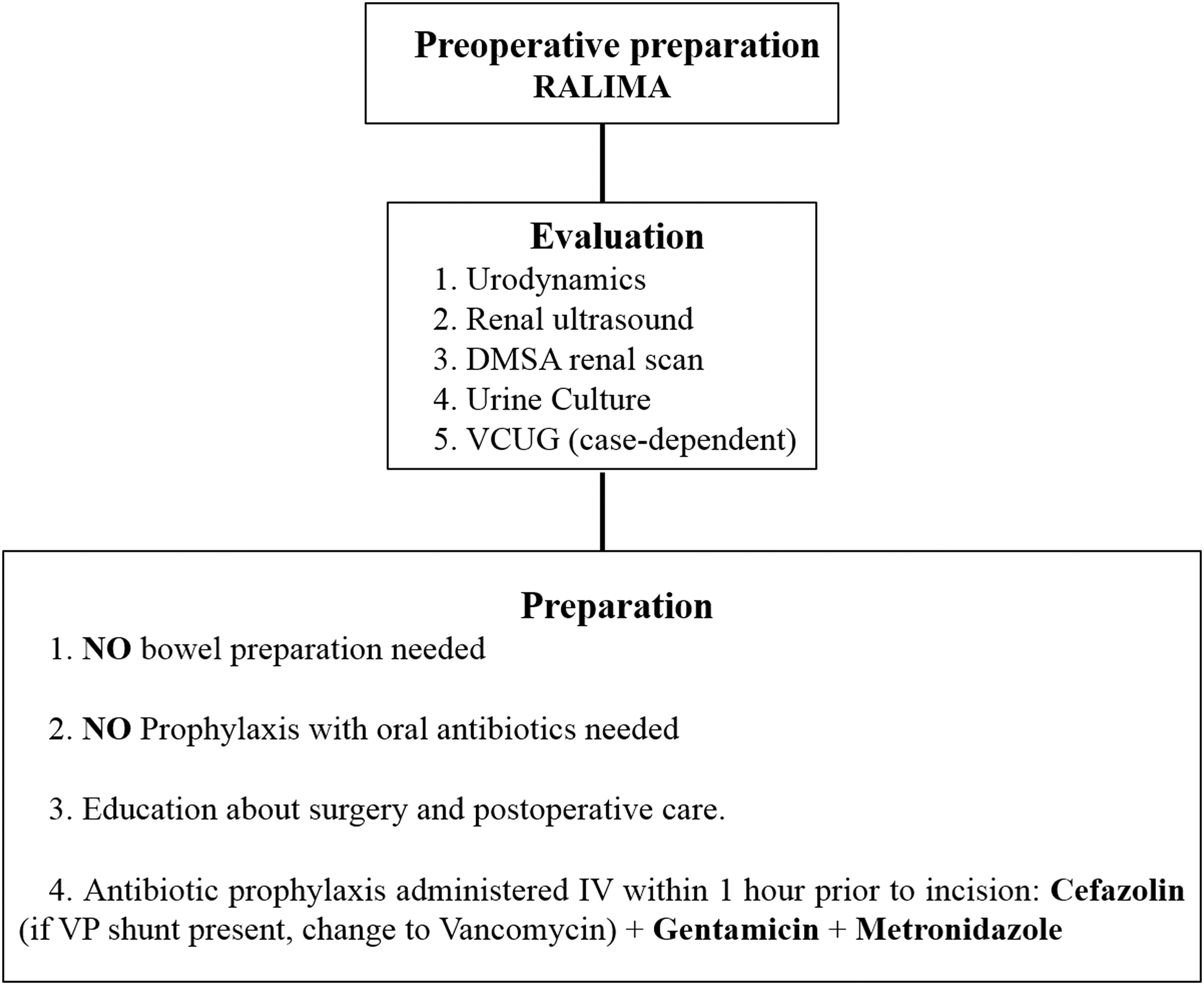
Preoperative preparation. DMSA = dimercaptosuccinic acid; VCUG = Voiding Cystourethrogram.
Patient Positioning
Having a broad perspective of the whole process and superior manual dexterity are very important aspects of a surgeon's skillset. Nevertheless, a proper patient positioning is arguably the most critical step of any surgery, especially when dealing with pediatric population due to the limited working space. When positioning a patient for any RAL surgery, the main goals are to ensure patient safety, avoid unintentional injuries, and allow for a wide range of movement of the robotic arms. This will guarantee a more efficient and safe surgery.
Once the patient is under general anesthesia, a cystoscopy and bilateral stent placement should be performed to aid in the intraoperative identification of both ureters in patients undergoing bladder augmentation. Of note, we do not routinely perform this step in our center, although we recommend it for those performing initial cases.
The patient is then placed in dorsal lithotomy position, with a Trendelenburg of ∼25° to 30°, keep the small bowel away from the surgical field, while allowing access to the appendix (Fig. 3). 9 The knees must be low lying to prevent collisions with the robotic arms, and the patient's arms are tucked to the sides. Foam padding should be used copiously on all pressure points to avoid injury, including hands, elbows, chest, and face (Fig. 4). The patient is then secured to the operating table using plastic sleds and security belts. 10

Patient in dorsal semilithotomy position.
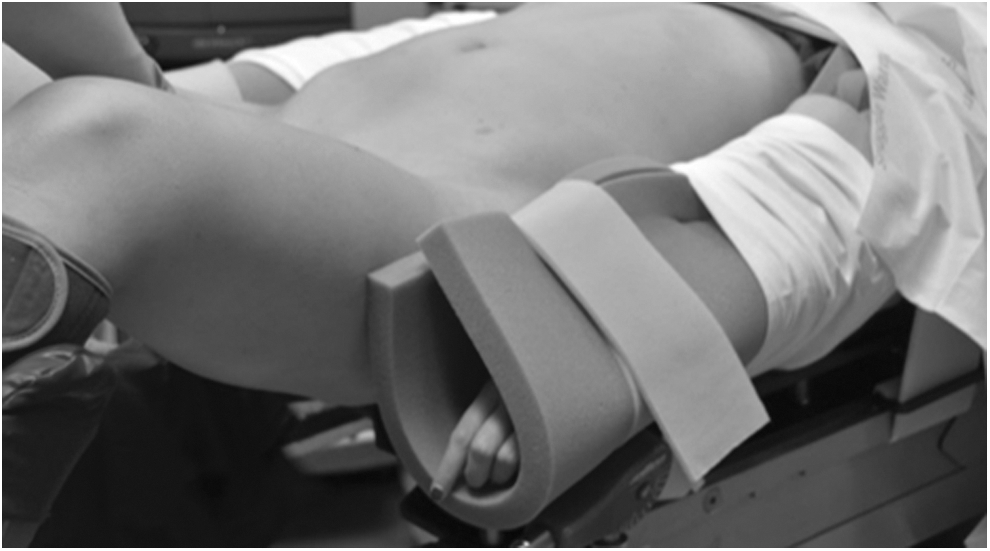
Copious foam padding in pressure points.
Once the patient is secured to the table, we use 3M™ Ioban™ 2 antimicrobial Incise Drape (3M) to better delineate the surgical field in a sterile manner. A clear plastic drape can be placed on the head of the patient to allow the anesthesia team to observe the surgery. Finally, it is recommendable to have a plastic pouch clamped to the side of the patient to place the instruments used by the assistant. (see Supplementary Video S3)
Surgical Steps
Port placement and docking of the robotic arms
For RALIMA cases, we recommend placing the camera port in a supraumbilical position to improve access to the appendix and bowel and facilitate their manipulation. Using an open Hasson technique to gain access, a 12 mm blunt tip balloon trocar is placed for the camera port. This trocar not only provides a superior anchoring system with the balloon, but also has a short intra-abdominal length, thus occupying the least space in an already limited working area. Initial peritoneal access under vision is preferred in children, given their short anterior-posterior diameter and proximity to the great vessels. 11
For the left and right robotic arms, we recommend using 8 mm ports; the impression of the port without its obturator can be used to better guide the incision length, to prevent the trocar from falling out during the procedure, and to prevent air leakage. We also recommend using local anesthesia in the port sites to minimize postoperative pain. The left arm port is placed 8 cm lateral to the umbilicus, the right arm port is placed 9 to 10 cm lateral to the umbilicus, and the port for the fourth arm is placed 7 to 8 cm lateral to the right arm port. A 12 mm assistant port is placed in the left upper quadrant, equidistant from the camera and left working port (Fig. 5). 10 In children taller than 5 ft, it is possible to use the fourth robotic arm, which will help in traction and counter traction during some crucial surgical steps.
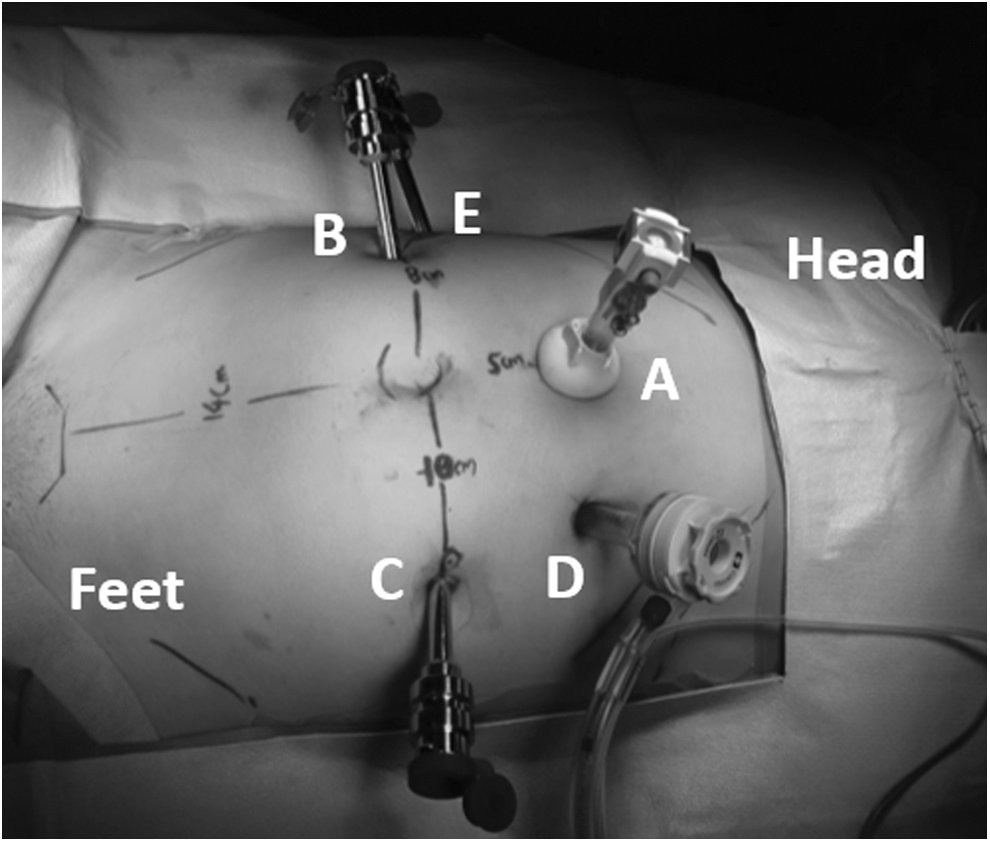
Ports placed.
The ports are inserted by using a twisting motion, while applying downward pressure against the abdomen. Some patients may have an elastic abdominal wall, making the port placement more challenging. In these cases, we recommend using a “trocar-in-port technique,” in which the trocar is more safely inserted by directing it into the camera port, minimizing the risk of unintentional bowel injury (see Supplementary Video S4).
Identification of the appendix
For initial identification of the appendix, we recommend to routinely perform a diagnostic peritoneoscopy before docking the robot, especially in patients with a VP shunt. If the appendix is not of adequate length, we recommend less experienced surgeons to convert to an open approach and perform a Monti CCC instead. 9
Appendiceal dissection
Once the appendix is identified, a stay suture placed at the tip can be helpful for traction and exposure while performing the appendiceal dissection. 12 A 3-0 polyglactin purse-string suture is placed at the base of the appendix and then the base is excised from the cecum. The purse-string is tied and the cecal opening closed in two layers with the same suture.
The appendiceal mesentery is mobilized and a window is made, carefully preserving the blood supply. The tip of the appendix is removed to create a proper lumen. Finally, the mobility of the appendix is evaluated to determine if it is suitable for creating a tension-free appendicovesicostomy (see Supplementary Video S5). 13
Bowel isolation and anastomosis
With a piece of premeasured silk, 20 cm of ileum is marked starting ∼15 to 20 cm from the ileocecal junction. We recommend using stay sutures at these points using a straight Keith needle introduced percutaneously (Fig. 6). The mesenteric window is created using electrocautery; we recommend using a Harmonic scalpel (Intuitive Surgical, Sunnyvale, CA), which maintains hemostasis efficiently. Finally, the ileo-ileal anastomosis is performed in an end-to-end manner using running 4-0 or 5-0 PDS suture (based on the diameter of the bowel), and the mesenteric window is closed (see Supplementary Video S6). 12
Bowel isolation and anastomosis.
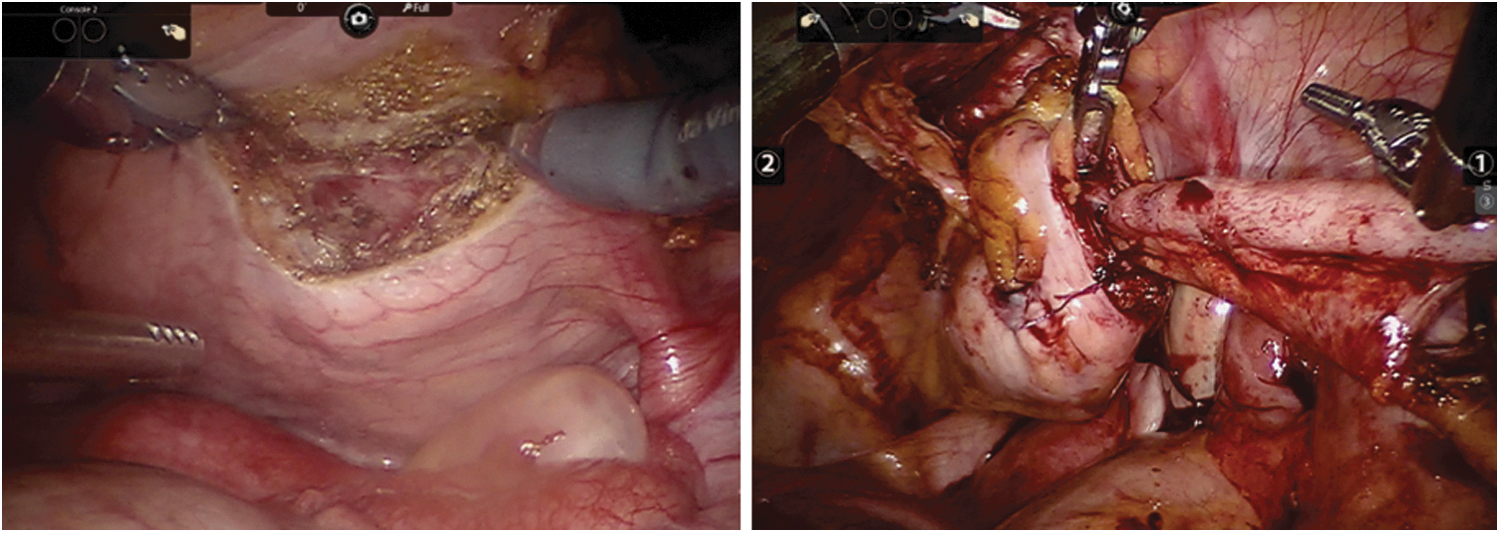
Cystotomy and appendicovesical anastomosis
To perform the detrusorotomy, we recommend to retract the bladder on the dome using a Keith needle, and then fill the bladder with saline to achieve proper distention to facilitate the incision. 12 If the plan is to create an umbilical stoma, this incision should be made in the midline. On the other hand, if a right lower quadrant stoma is to be made, then an oblique detrusorotomy is recommended. 9 Interestingly, some report using a second insufflator connected to the urethral catheter to control and adjust bladder distention more rapidly and avoid draining fluid into the field. 14
A critical part of this surgery is ensuring a proper bladder submucosal tunnel length when performing the appendicovesical anastomosis, but the ideal length is controversial. Although other reports suggest a tunnel between 2.5 and 5 cm, 15 –17 we at the University of Chicago recommend a submucosal detrusor tunnel, made in the direction of the future stomal site, of at least 4 cm to achieve stomal continence. 9,18
In cases of RALIMA, where augmentation ileocystoplasty is also performed, we recommend reimplantation of the appendix to the posterior bladder wall, either with an extravesical or intravesical approach, 5 given the orientation of the mesentery.
On the other hand, if the patient is undergoing an isolated CCC creation without ileocystoplasty, we prefer placing the channel in the anterior bladder wall with an extravesical anastomosis, 9 as it is technically easier to then place the stoma in the anterior abdominal wall and the length needed to reach it is less. 23 Although there is some concern that this approach increases the risk of urinary tract infections and bladder stones, 19 we have not found such increased risk in our experience.
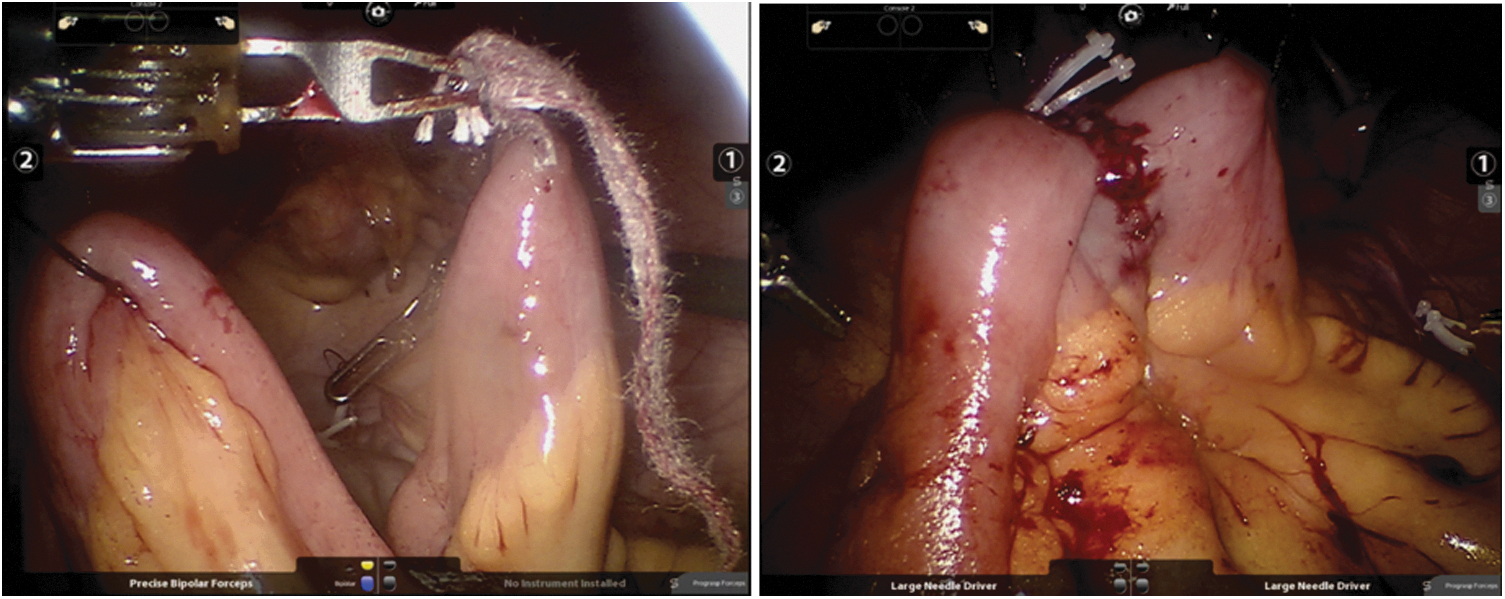
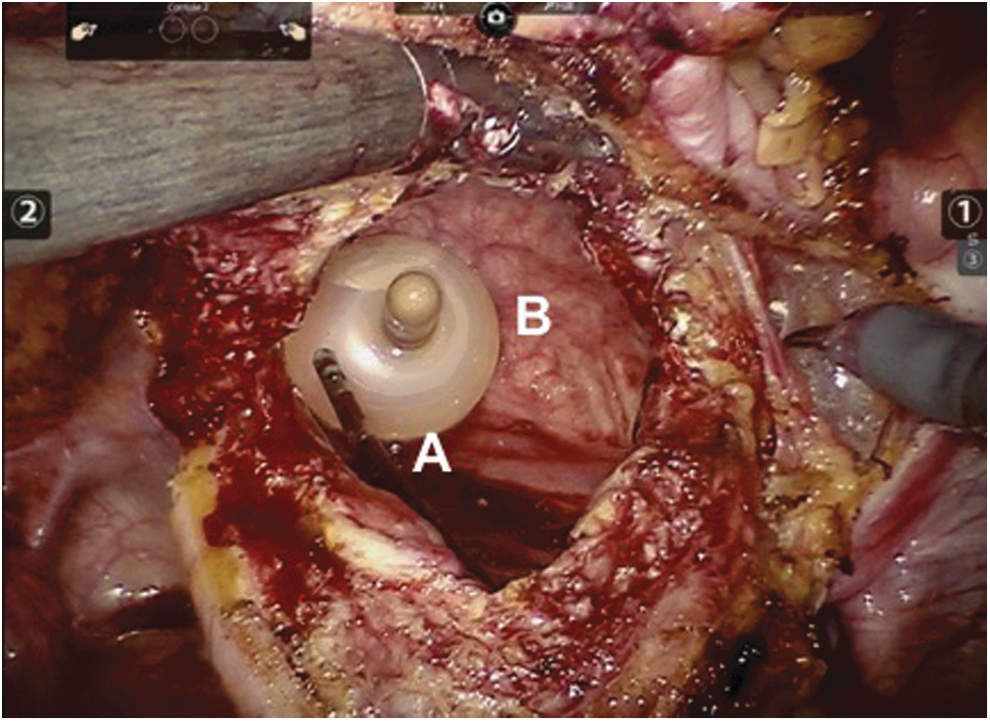
The anastomosis begins with suturing the apical tip of the appendix to the caudal apex of the detrusorotomy. The bladder mucosa is then incised to accommodate the appendix lumen, and the anastomosis is performed in a continuous manner with a running 5-0 PDS II (polydioxanone) suture (Johnson & Johnson Medical Ltd., Livingston, West Lothian, United Kingdom) over an 8F feeding tube placed through the appendix. Finally, the detrusor layer is reapproximated over the appendix with a continuous 4-0 polyglactin suture to provide an adequate continence mechanism (Fig. 7). The 8F feeding tube is secured to the bladder mucosa to prevent migration, and a stay suture is placed at the proximal end of the appendix for easier manipulation and prevention of twisting, while maturing the appendix to the skin. (see Supplementary Video S7) 12,18
Appendicovesical anastomosis.
Ileal de-tubularization and ileovesical anastomosis
Once the appendicovesical anastomosis is in place, we proceed to perform the ileocystoplasty. The initial step is to incise the bladder in a coronal plane, which will allow us to identify both ureteral orifices and the feeding tube inserted through the appendix (Fig. 8). Careful consideration should be taken to preserve both ureteral orifices; this is why we recommend the retrograde placement of bilateral ureteral catheters at the beginning of the procedure, especially early in the learning curve. An 18F Foley suprapubic catheter is introduced at this point at the left lower aspect of the abdomen, and then placed into the bladder through its anterior wall.
Bladder coronal incision.
The ileal de-tubularization is performed by incising along the antimesenteric border with the Harmonic scalpel, and then the proximal and distal ends are sutured to the left lateral and right lateral apices of the cystotomy, respectively. The posterior edge of the cystotomy is anastomosed to the ileal segment first, suturing from inside the bladder (Fig. 9). The anterior portion of the cystotomy is then sutured to the opposite edge of ileum with an extravesical view of the bladder. We recommend using a 2-0 braided absorbable suture and a Mega™ Needle Driver (Intuitive Surgical), as well as Lapra-Ty clips (Ethicon Endo-surgery) to reduce tension on the continuous suture line (Fig. 10; see Supplementary Video S8). 12

Ileal de-tubularization and ileovesical anastomosis.
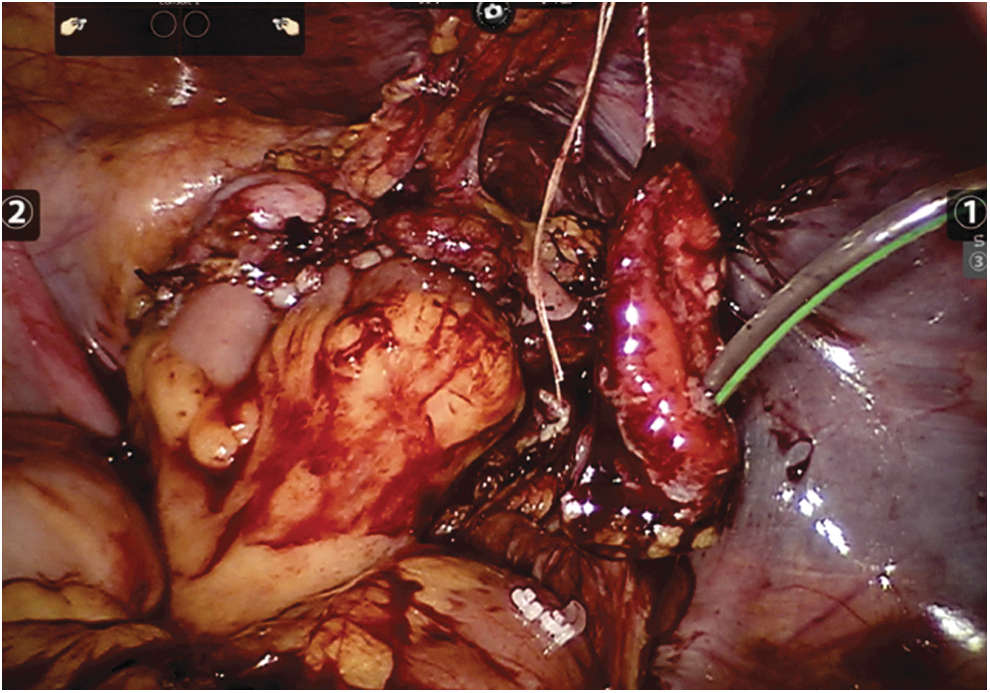
Augmented bladder and appendicovesicostomy.
Appendicovesicostomy
The location of the stoma on the abdomen for the appendicovesicostomy will vary according to the direction of catheterization, as well as the size and elasticity of the appendix. The appendix is then delivered through the skin using the stay suture previously placed, and finally a VQZ stomal flap is created to optimize aesthetic outcome. 12 .
Port site closure
The augmented bladder is drained with the 18F suprapubic catheter; a Foley urethral catheter and an 8F feeding tube by way of the appendicovesicostomy are also left in place. Finally, a pelvic drain is also placed to control postoperative bleeding. 12
Port-site fascial closure should be performed under direct vision to prevent omental hernias, since omentum can follow the direction of the trocar when this is removed and herniate through the incision (see Supplementary Video S9).
Postoperative Care
During the postoperative period, special efforts should be made to minimize narcotic use in pain management, encourage early diet advancement, and promote ambulation. For pain management, we recommend scheduled acetaminophen and NSAIDs with opiates as necessary. 2 Opiates should be restricted to avoid exacerbation of restrictive lung disease in patients with kyphoscoliosis. 5
Those patients bound to a wheel chair receive a dose of subcutaneous heparin before the surgery and another one afterward, to prevent deep venous thrombosis secondary to immobilization.
In regard to diet, patients with isolated Mitrofanoff appendicovesicostomy start with regular diet immediately, while those undergoing CCC and aumentation ileocystoplasty can start regular diet within 24 hours.
The patient is discharged home when regular diet is tolerated, pain adequately controlled, and the patient and family are comfortable with drainage tubes. Both suprapubic and appendicovesicostomy catheters are left in place for ∼4 weeks, then the latter is removed and independent CIC is initiated. The suprapubic catheter is capped and maintained for as much as one week or until the family is comfortable performing CIC.
The patient is followed in the clinic two weeks postoperatively, to assess for perioperative complications and reinforce education on CIC. The next visit is four weeks after surgery for RUS and physical evaluation. If the patient has an uneventful postoperative course, follow-up visits are scheduled on a yearly basis with an RUS and basic metabolic panel. After five years, we also assess vitamin B12 levels (see Supplementary Video S10).
Troubleshooting
Patients with VP shunts
The main concern in these cases is the risk of introducing bacteria and/or carbon dioxide (CO2) into the shunt, leading to shunt malfunction. Before starting intestinal manipulation, the VP shunt distal end should be placed in a 5 mm Endopouch bag (Ethicon Endo-Surgery). The pouch in cinched around the tube and placed in the subhepatic space for the entire surgery. To minimize the risk of pressure-induced changes in the VP shunt, we recommend to keep the pneumoperitoneum pressure at or below 12 mm Hg, although recent shunts have pressure-resistant valves. 8
In our experience, a VP shunt can have adhesions and displace the appendix from its traditional location, which can be found even in the subhepatic space. This is why, in patients with VP shunts, we recommend to perform a conventional diagnostic laparoscopy to locate the appendix, perform adhesiolysis if necessary, and place the appendix in a more accessible location before placing the ports and docking the robotic arms (see Supplementary Video S11).
Managing patients with kyphoscoliosis
We recommend against performing RALIMA in patients with severe kyphoscoliosis and concomitant conditions, given the limited space for the robotic arms to work and the difficulty to achieve a proper pneumoperitoneum.
Our interim Results
We reported the first intracorporeal RALIMA in 2007 and have been performing this procedure since then. We have also reported our short and interim outcomes throughout the years, more recently in 2015. In this study, we concluded that even though the operative time was longer in the robotic approach, it decreases the length of stay and avoids epidural use. 5
Summary
The use of RAL surgery in pediatric urology has increased in recent years, and its benefits, such as improved cosmesis, decreased postoperative pain, estimated blood loss, and hospital stay, are extremely appealing for some. Nonetheless, these should be weighed against the learning curve, costs, and operative time, to decide if adopting this approach.
One of the largest sources of morbidity in RALIMA is the use of bowel segments for cystoplasty 21,22,25; thus tissue engineering remains a challenging and promising area for researchers.
Currently, more parents opt for minimally invasive procedures for their children, and robot-assisted surgery is becoming more widely adopted by pediatric urologists. This atlas of minimally invasive surgery serves as a valuable tool for the standardization of surgical techniques, as well as to ameliorate the steep learning curve of RAL surgery in pediatric patients. To view full video, “RALIMA – Mohan S. Gundeti.mp4,” click here.
Recommended Video from Videourology
1. Videourology 2012; Vol. 26, No. 6
Simultaneous Robot-Assisted Laparoscopic Continent Catheterizable Channels: The Split Appendix Technique
Thomas W. Mader, Dennis Liu, Marcelo A. Orvieto, Beverly Dooley, and Mohan Gundeti
Footnotes
Author Disclosure Statement
Dr. Gundeti: course director, Intuitive Surgical.