
Abstract
Historically, the gold standard for management of ureteropelvic junction obstruction (UPJO) has been open pyeloplasty. However, continued technological and surgical advances have ultimately led to the robotic approach. Continued advances in minimally invasive surgery have led to shorter hospital stays and hastened recovery. Here we present our step by step guide and video to robotic-assisted laparoscopic pyeloplasty.
Indications
Historically the gold standard for management of ureteropelvic junction obstruction (UPJO) has been open pyeloplasty. However, since laparoscopic assisted pyeloplasty was first described by Schuessler et al. in 1993, the minimally invasive approach has gained wide popularity and acceptance among both academic and community urologists. Continued evolution has led now to the robotic approach with steady increase in dissemination. 1,2 The primary goals of correcting a UPJO are to prevent further deterioration in renal function and relieve symptoms.
Ureteral obstruction is defined as any restriction to urinary outflow, which if left untreated will lead to progressive kidney damage and potential loss of function. The causes of UPJO can be divided into congenital and acquired, with congenital causes being more common. Congenital causes are further divided into intrinsic and extrinsic causes. Intrinsic causes of UPJO include adynamic ureteral segment caused by ureteral smooth muscle maldevelopment (most common cause of pediatric UPJO), inadequate recanalization during fetal development, and persistent valvular mucosal folds. Extrinsic causes include crossing accessory lower pole vessel (most common cause of adult UPJO); high ureteral insertion into the renal pelvis; and horseshoe, ectopic, or malrotated kidney, causing kinking at the ureteropelvic junction (UPJ). Acquired causes of UPJO are severe vesicoureteral reflux leading to ureteral tortuosity and kinking at the UPJ and inflammation and scarring from trauma, urolithiasis, instrumentation, infected urinoma, or retroperitoneal fibrosis.
The indications for pyeloplasty include progressive impairment of renal function and the development of upper tract infection or calculi. The risk for progressive renal impairment is best demonstrated with a Lasix renogram, MAG-3, typically showing a T 1/2 time >20 minutes and differential function <40% on the affected side. Episodic abdominal complaints or ipsilateral colicky flank pain is the typical presentation in older infants and children. Adults may present with episodic ipsilateral colicky flank pain, classically after diuretic or alcohol intake, otherwise known as the Dietl crisis. In situations of T ½ between 10 and 20 minutes in the equivocal range, presence of symptoms or decrease in function may aid in treatment options.
Laparoscopic or robot-assisted laparoscopic pyeloplasty is indicated over endopyelotomy in the following circumstances: severe hydronephrosis, poorly functioning kidney (<25%), previous failed endopyelotomy, presence of a crossing vessel, and presence of a stricture >1 cm. There are several contraindications to robot-assisted laparoscopic pyeloplasty. Active urinary tract infection is a contraindication as there is a higher risk of subsequent pyelonephritis, sepsis, and abscess development. The presence of a collecting system defect not consistent with urolithiasis is another contraindication. Ureteroscopy should be performed before pyeloplasty to rule out neoplasm. A high suspicion for malignancy must be maintained in elderly patients. Finally, a poorly functioning kidney is a contraindication to pyeloplasty as the patient would benefit more from a laparoscopic nephrectomy if symptoms are present or recurrent infection occurs.
Preoperative Preparation
Preoperative urinalysis and urine culture are obtained before proceeding with surgical intervention, with positive urine cultures treated with appropriate antibiotics. Routine laboratory and imaging studies, including complete blood count, basic metabolic panel, and chest radiograph, are also ordered preoperatively. Appropriate imaging studies are obtained preoperatively to assess the degree of hydronephrosis associated with the UPJO. It is prudent to determine the function of the affected kidney to decide whether laparoscopic reconstructive or extirpative surgery should be performed. If the function of the affected renal unit is <15%–20% of total renal function, then laparoscopic nephrectomy should be performed. A nuclear medicine renal scan with furosemide washout can be used to determine the degree of obstruction and help assess postoperative outcomes.
Cystoscopy with retrograde pyelogram, ureteral stent placement, and Foley catheter placement before ureteral reconstruction is optional. The authors prefer to perform this step initially as it allows for accurate delineation of ureteral anatomy, exclusion of distal stricture, and detection of any possible filling defects. If no unexpected findings are encountered, a double pigtail ureteral stent is placed under fluoroscopic and cystoscopic guidance. This step is shown in the Supplementary Video S1 for step 1 (Supplementary Data are available online at
Patient Positioning
The patient is placed in the modified lateral position. A bump is placed under the shoulder and hip. The patient is then secured in place using silk tape over the patient's arms, hips, and legs (Fig. 1). The table is rotated to ensure the patient remains in the proper position and does not slide.
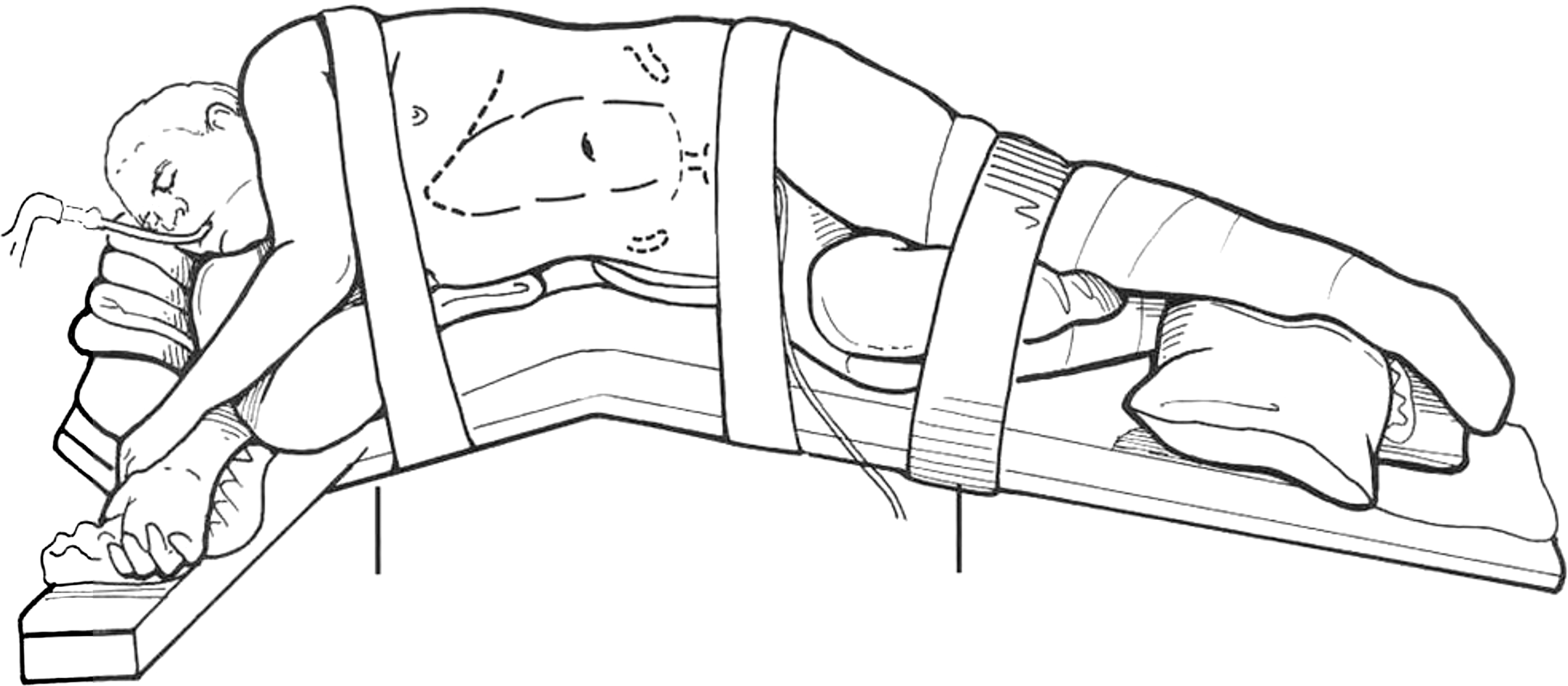
Patient positioning for laparoscopic pyeloplasty. Reproduced from Bishoff et al. 9
Pneumoperitoneum is created typically using Veress needle technique. Correct Veress needle placement in the peritoneum is confirmed by aspiration with no withdrawal of blood or fecal matter and more commonly with maintenance of a low pressure (<10 mm Hg) pneumoperitoneum with slow insufflation of carbon dioxide. After establishment of pneumoperitoneum, one can proceed with trocar placement. With the Xi configuration, the robot trocars are then placed in a straight line configuration in a paramedian position with 8 cm between each trocar. The second port is placed over the renal hilum. A 12-mm assistant port is also placed to allow for passage of needles (Fig. 2). Trocar placement is seen in step 2 video.
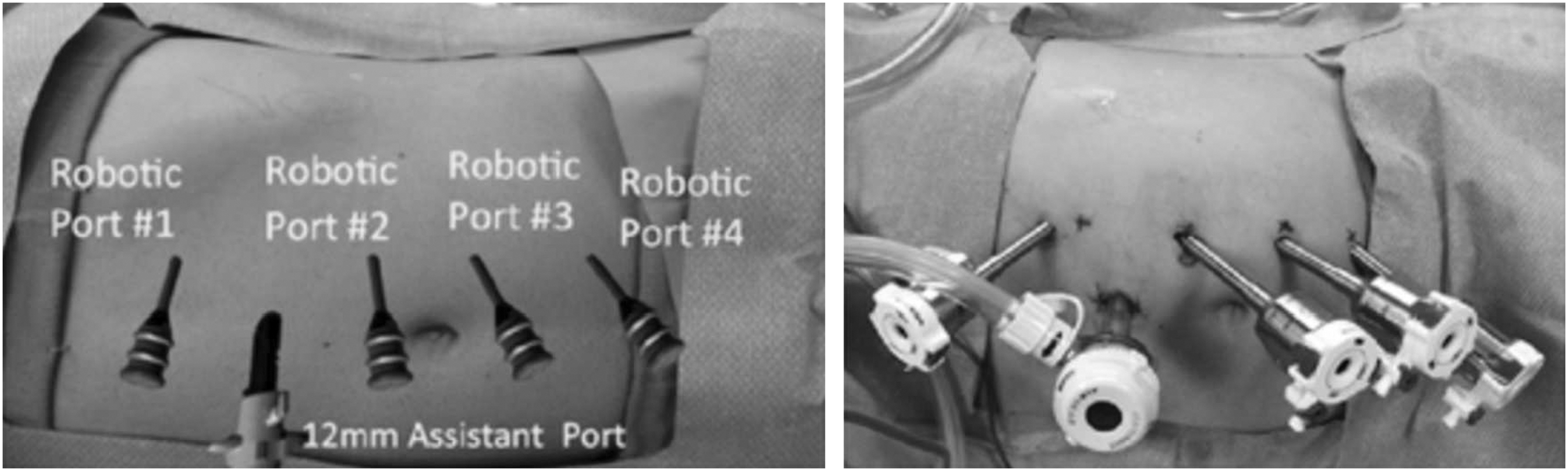
Trocar placement for the da Vinci Xi robot.
Surgical Steps
To begin the dissection, the white line of Toldt is reflected using the Maryland bipolar forceps and the monopolar scissors. This allows for access to the retroperitoneum (Fig. 3).
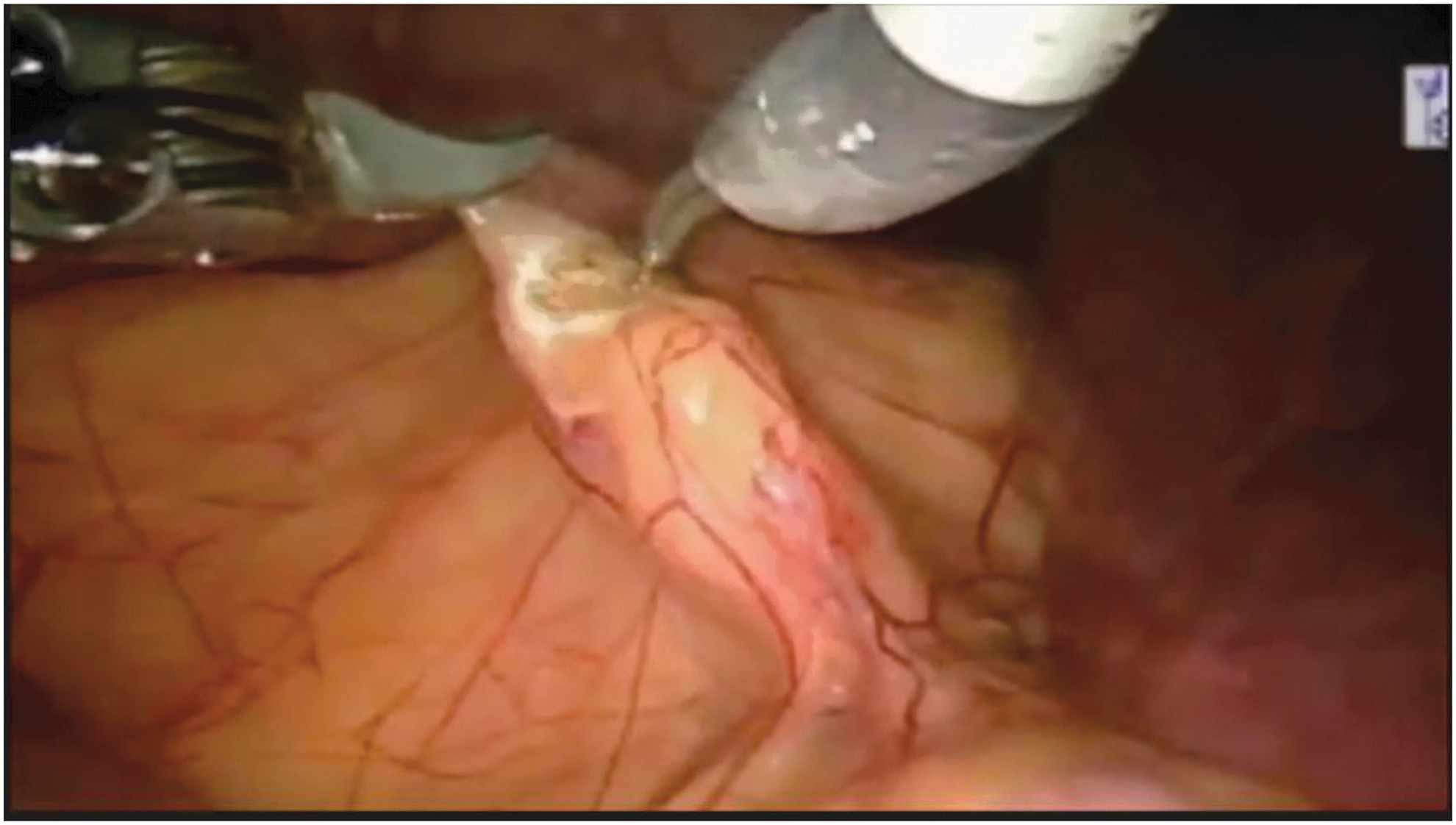
Reflection of the white line of Toldt.
After observation of the psoas muscle, the ureter is identified just medial to the lower pole of the kidney and traced cephalad toward the renal pelvis. The ureter can be distinguished from the gonadal vessels by peristalsis and by the presence of the internal stent. It is meticulously dissected in a manner as to not to disrupt the periureteral tissues carrying its blood supply (Fig. 4). The isolation of the ureter is seen in step 3 video.
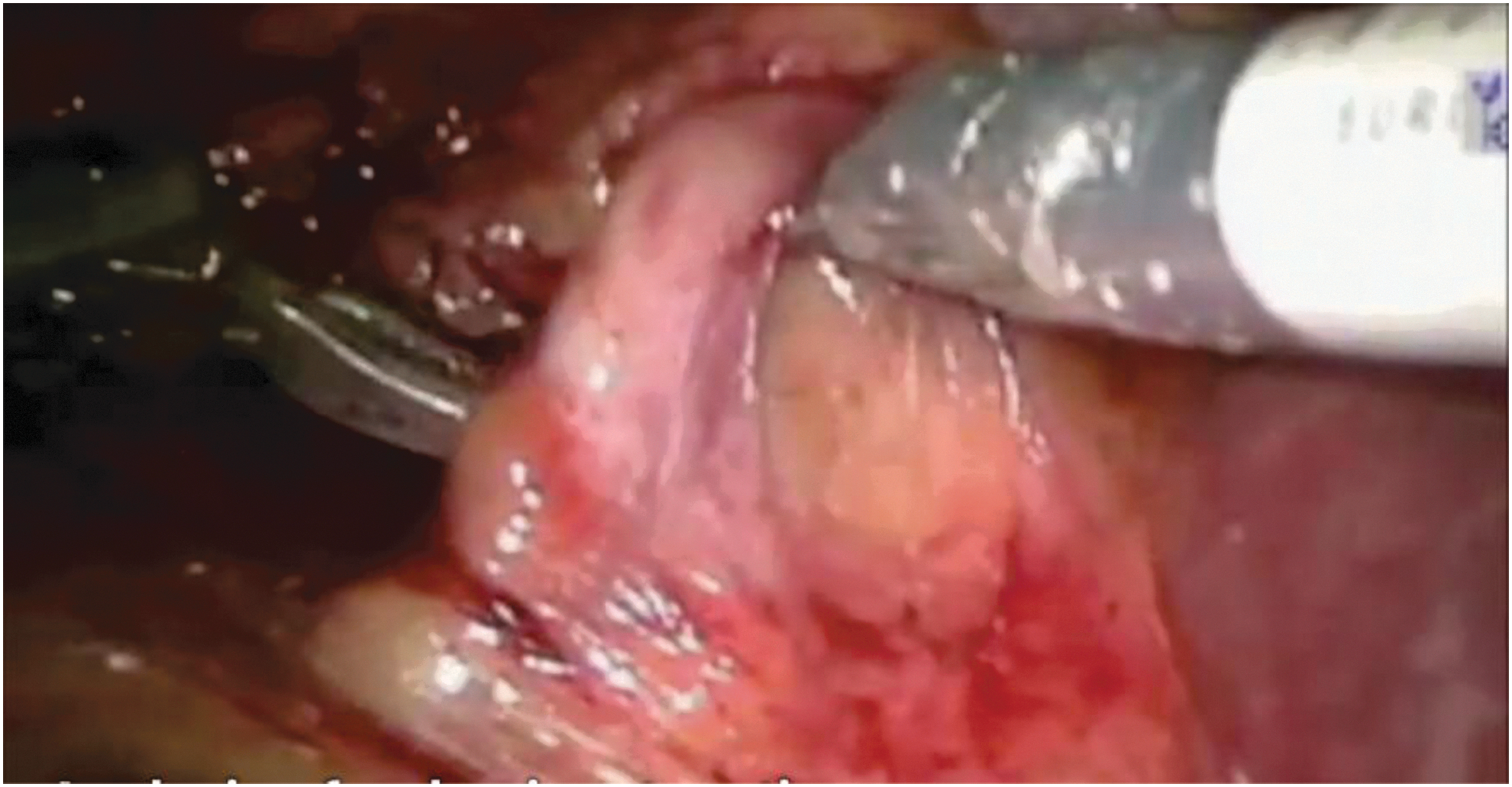
Ureter is traced cephalad.
The renal pelvis is dissected anteriorly and posteriorly up to the renal sinus to allow for optimal drainage and funneling. This also allows for complete mobilization of the pelvis (Fig. 5).

Renal pelvis is dissected.
Inspection of the UPJ should assess for the presence of a crossing vessel as it is present in ∼40% of all cases of UPJO and even higher in patients undergoing secondary pyeloplasty. 3,4 If a crossing vessel is identified as the cause of obstruction, it may be transposed posteriorly. However, transposition of the crossing vessel is not always necessary. A Keith needle is placed on the renal pelvis to help stabilize the renal pelvis and assist in the anastomosis. In addition, it makes placing another port unnecessary. The needle is placed through the abdominal wall, through the renal pelvis, and back through the abdominal wall. The stitch can be used to aid in the dissection of the cephalad-most aspect of the renal pelvis (Fig. 6). Dissection of the renal pelvis and placement of the hitch stitch are seen in step 4 video. Further mobilization of the renal pelvis is shown in step 5 video.

Keith needle placed through the renal pelvis.
The ureter is then transected from the renal pelvis. The ureter is divided at the level of the UPJ using care not to cut across the indwelling ureteral stent. Before complete transection, the ureter is spatulated on the lateral aspect. This will prevent spiraling of the ureter (Fig. 7). This will also help to maintain the orientation of the ureter. The ureter will need to be transposed anteriorly in the presence of a crossing vessel. Transection of the ureter is seen in step 6.
Spatulation of the ureter.
Using a 4-0 Vicryl on a tapered needle, the first stitch is placed at the apex of the ureter and brought out through the renal pelvis.
Once the anterior aspect of the anastomosis is completed, the stitch can be used to rotate the pelvis for complete exposure (Fig. 8). The ureteral stent is slid back and forth to ensure that there is no inadvertent entrapment of the stent within the stitch. The superior aspect of the stent is then placed within the renal pelvis.

Ureteral anastomosis.
If the renal pelvis is severely hydronephrotic, excess tissue may be trimmed and the pelvis tapered. Trimming of the renal pelvis is seen in step 7 (Fig. 9).

Redundant renal pelvis trimmed and tapered.
The ureteral anastomosis is then completed and the renal pelvis is closed. The ureteral anastomosis is shown in step 8. Fascial defects secondary to trocar placement are closed with 1-0 Vicryl using a Carter–Thompson device in an effort to minimize postoperative trocar site hernia. The skin is closed with a subcuticular closure and covered with a dry sterile dressing. A Foley catheter and a Jackson-Pratt (JP) drain are left in place.
Postoperative Care
The Foley catheter is removed on postoperative day 1. If the output from the JP drain is <50 cc, the drain is removed. If the output is >50 cc, the drain fluid is sent for creatinine and the drain is removed if the value is serum. The patient is discharged home on postoperative day 1. The ureteral stent is typically removed 4–6 weeks after surgery. A Lasix renal scan is obtained 1 month after stent removal. After that point, a scan is repeated every 6 months for the first year and then annually thereafter.
Troubleshooting
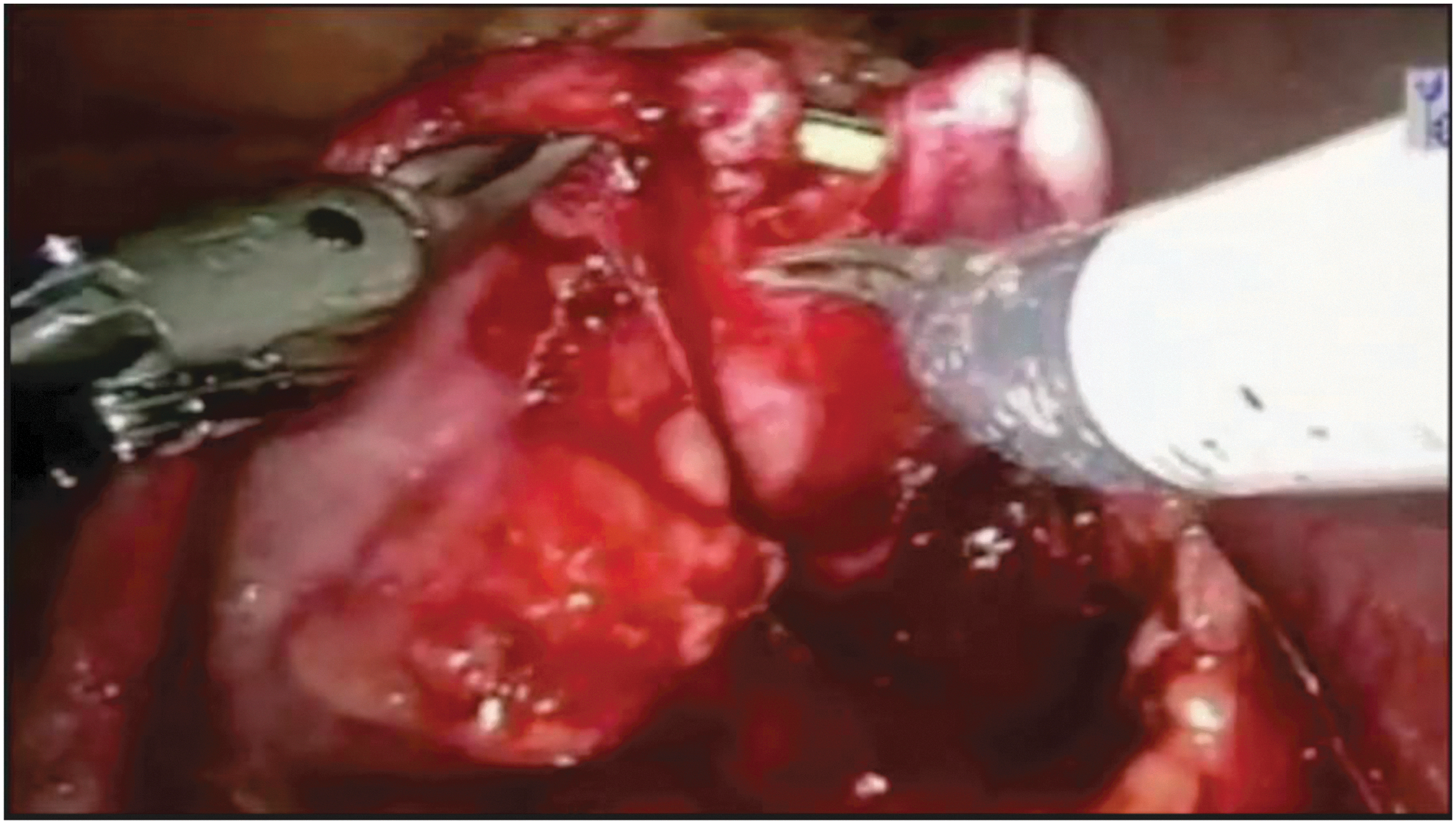
The concomitant presence of renal calculi and UPJO can be managed at the time of ureteral reconstruction using laparoscopic grasping forceps or a 16F flexible cystoscope placed through the 12 mm assistant port with nitinol endoscopic basket to render the patients stone-free (Fig. 10). 5 –7

Robotic pyeloplasty with concomitant pyelolithotomy.
For obese patients, the trocar placement is shifted laterally to maintain ease of access to the renal pelvis.
Robot-assisted laparoscopic pyeloplasty in horseshoe kidney is feasible. 8 Positioning of the trocars more inferior is necessary for optimal dissection. Bowel retraction may be aided by Trendelenberg position and assistant retraction with a fan retractor. It is critical to identify and preserve any aberrant renal vessels.
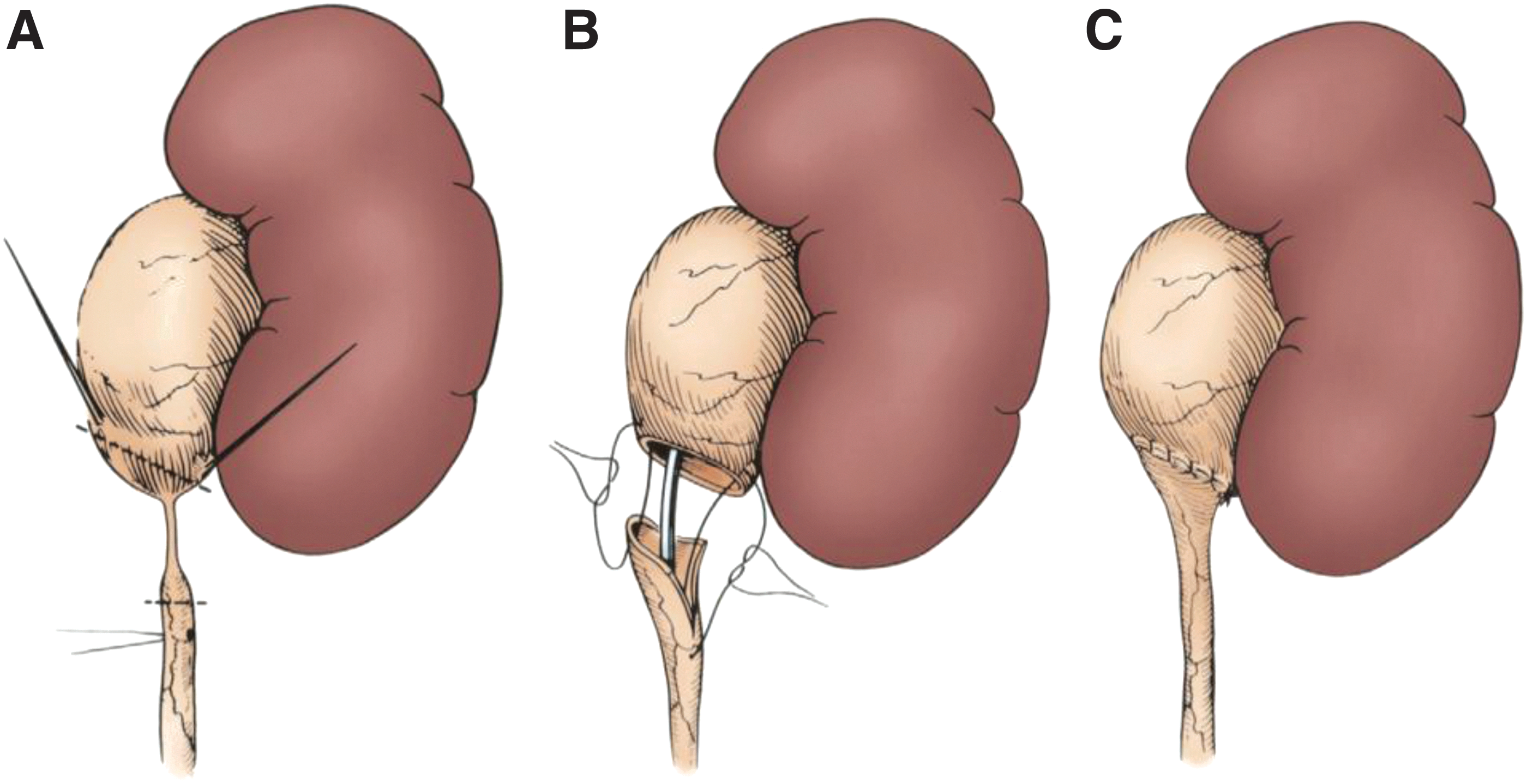
The Anderson–Hynes dismembered pyeloplasty is the preferred technique and is considered the gold standard for UPJO repair (Fig. 11). The advantages of this technique include the ability to correct the obstruction while preserving a vessel crossing the lower pole, the adynamic segment of the ureter is resected, and redundant pelvic tissue is reduced.
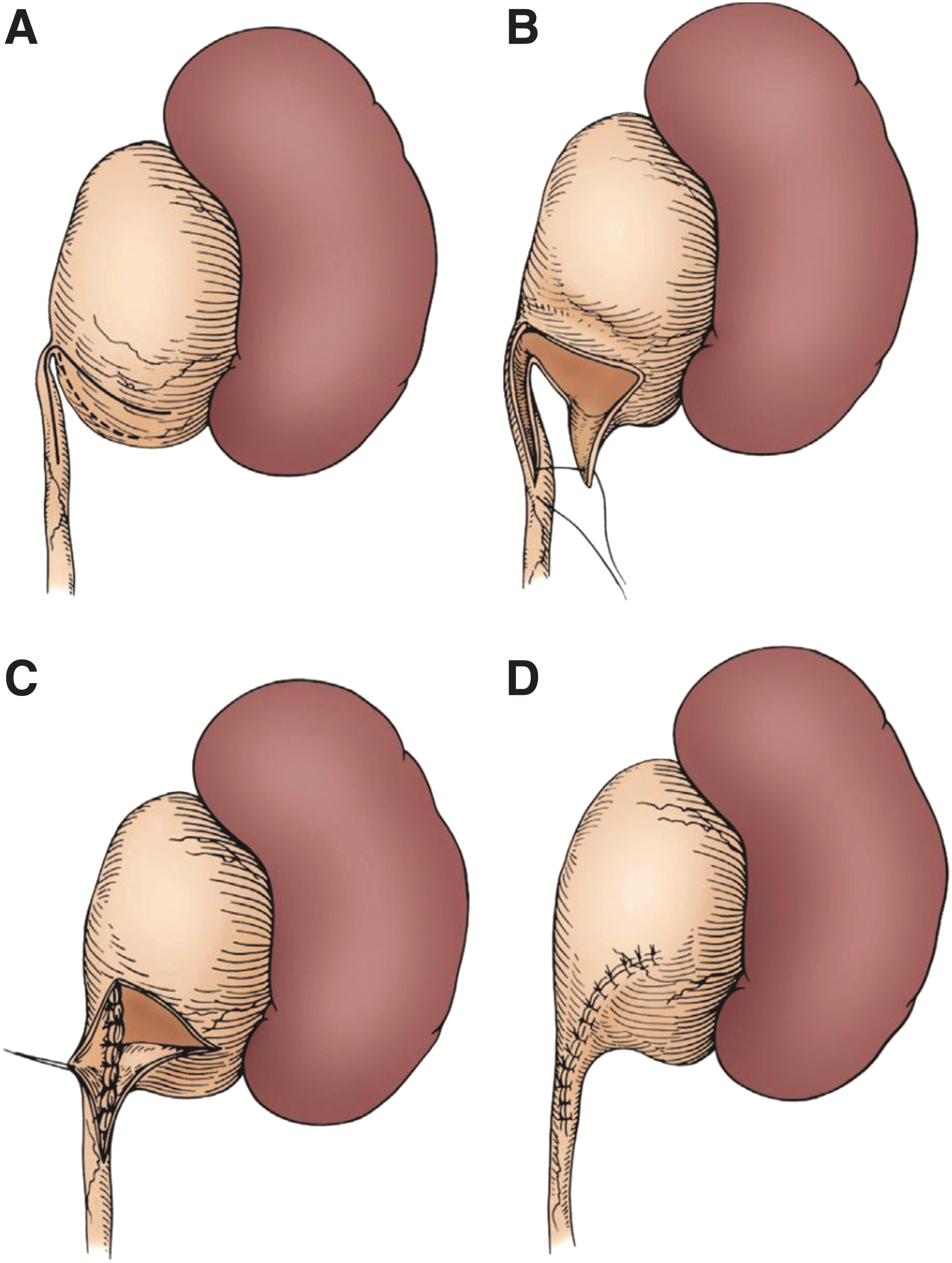
The Foley Y-V plasty is a nondismembered technique that can be utilized in cases with a high insertion of the ureter and no crossing vessel (Fig. 12).
Recommended Videos from Videourology
1. Lee BR, Maddox M, Thomas R. Robotic Pyeloplasty Step by Step. . January 2014, 28.
2. Roth E, Larson J, Patel A, Figenshau RS. Robot-Assisted Retroperitoneal Pyeloplasty. November 2014, 28.
3. Lucas SM, Sundaram CP. Transperitoneal Robot-Assisted Laparoscopic Pyeloplasty. Journal of Endourology Part B, Videourology. January 2011, 25.
4. Mufarrij PW, Rajamahanty S, Krane LS, Hemal AK. Intracorporeal Antegrade and Retrograde Stenting During Robot-Assisted Urinary Tract Reconstruction: Is It the Ideal Choice?. Journal of Endourology Part B, Videourology. March 2012, 26.
5. Shah AB, Dangle PP, Llarena NC, Gundeti MS. Robot-Assisted Laparoscopic Pyeloplasty in the Infant: Critical Steps for Successful Completion. November 2013, 27.
Footnotes
Supplementary Videos
Click here for Supplementary Videos: Robotic Pyeloplasty Step 1.mp4; Robotic Pyeloplasty Step 2.mp4; Robotic Pyeloplasty Step 3.mp4; Robotic Pyeloplasty Step 4.mp4; Robotic Pyeloplasty Step 5.mp4; Robotic Pyeloplasty Step 6.mp4; Robotic Pyeloplasty Step 7.mp4; Robotic Pyeloplasty Step 8.mp4; Robotic Pyeloplasty Step 9.mp4; Robotic Pyeloplasty Closing.mp4; Robotic Pyeloplasty Title Screen.mp4
Author Disclosure Statement
No competing financial interests exist.