
Abstract
Objective:
To evaluate the efficacy and safety of laparoendoscopic single-site surgery (LESS) in the repair of intraperitoneal bladder rupture.
Patients and Methods:
All consecutive patients who underwent LESS for intraperitoneal bladder rupture in three hospitals in Korea were included prospectively in this study. LESS was performed using a homemade single-port device composed of an Alexis wound retractor and a surgical glove.
Results:
Of the 22 patients, 18 were male. The mean age was 40.50 ± 11.83 years. The mean body mass index was 24.19 ± 2.61 kg/m2. The cause of rupture was trauma (n = 21) or iatrogenic injury (n = 1). The mean bladder rupture diameter was 3.41 ± 1.01 cm. LESS bladder rupture repair was completed effectively in all patients. The mean operative time was 89.05 ± 11.29 minutes. The mean length of hospital stay was 2.91 ± 0.53 days. Postoperatively, none of the patients required patient-controlled analgesia, and none developed major complications. The urethral Foley catheter was removed 7.68 ± 2.08 days after surgery.
Conclusions:
LESS repair of intraperitoneal bladder rupture, which involves a homemade single-port device, was a feasible and safe alternative to conventional laparoscopy in this case series.
Introduction
T
Bladder rupture can be extraperitoneal (50%–71%), intraperitoneal (25%–43%), or both (7%–14%). 5 Intraperitoneal bladder rupture is conventionally managed by laparotomy. However, procedural and technical advances over the last decade mean that open procedures are steadily being replaced with laparoscopic surgery. 6 This is because laparoscopic procedures are less invasive and consequently associate with less postoperative pain, shorter hospital stays, and an earlier return to normal activity. 7 In relation to intraperitoneal bladder rupture, Matsui and colleagues showed that laparoscopic suturing of the bladder laceration is an efficient and feasible procedure. 8
Laparoendoscopic single-site surgery (LESS) is a recently introduced procedure in which the laparoscopic instruments are all inserted through a single-incision site. 9 Lee and colleagues showed that LESS improves esthetic outcomes. 10 Moreover, LESS has been shown to be feasible for several disorders that are usually treated with conventional laparoscopic surgery. 11,12 In addition, Choi and colleagues showed recently that LESS is an effective method for treating benign urologic disease. 13 However, to date, the usefulness of LESS for treating intraperitoneal bladder rupture has not been reported.
This prospective study was performed to determine the efficacy and safety of the LESS procedure for repairing intraperitoneal bladder rupture.
Patients and Methods
Patients
All consecutive patients who underwent LESS for repair of intraperitoneal bladder rupture between February 2014 and August 2016 in three hospitals in Korea (Hanyang University Hospital, Guri; Hallym University Hospital, Pyeongchon; and Dong-A University Hospital, Busan) were included prospectively in this study. Intraperitoneal rupture was confirmed by conventional cystography (Fig. 1). The three medical centers followed the same study protocol. The study was approved by the Institutional Review Boards of the hospitals.
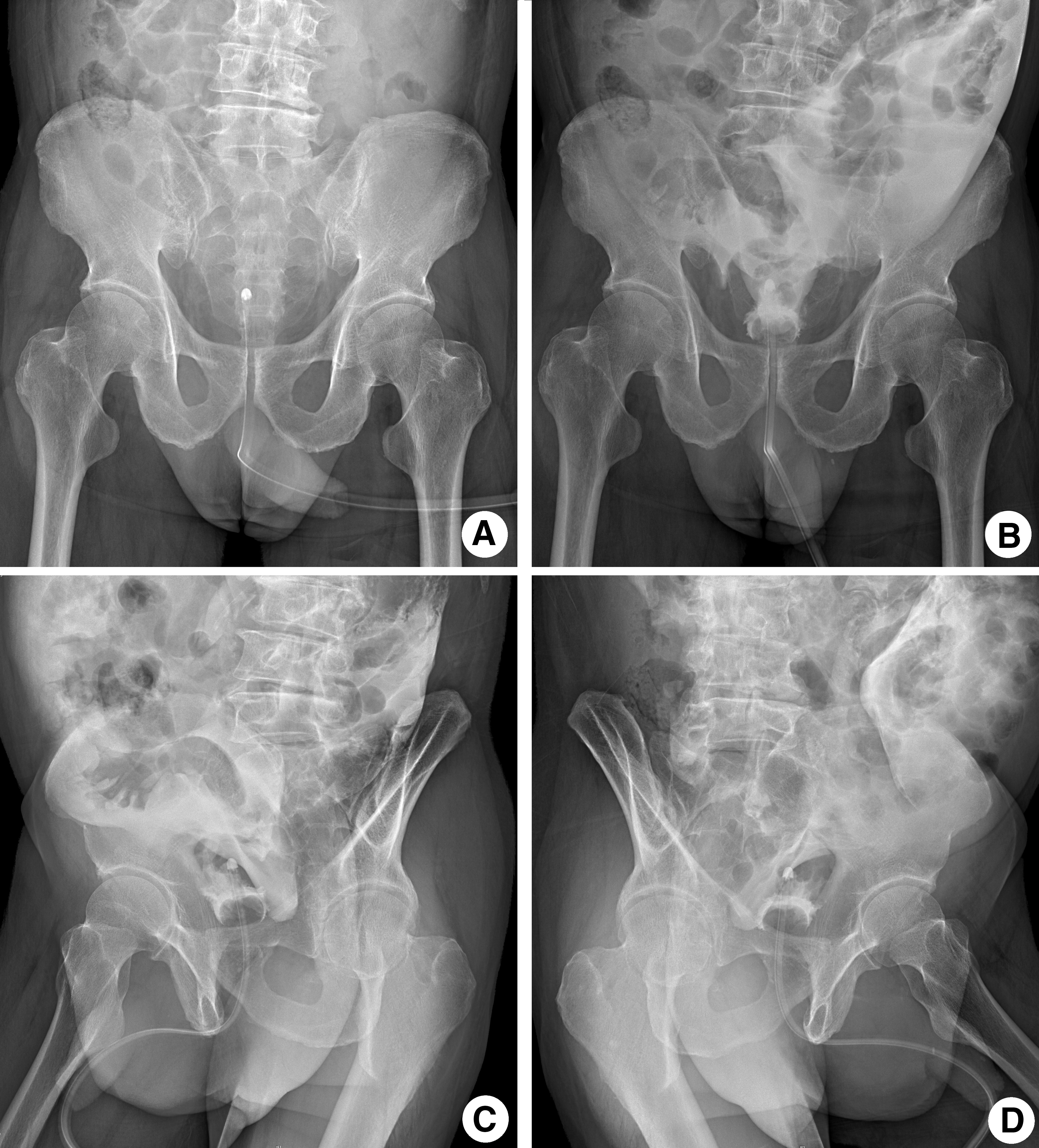
Preoperative cystography in a patient with intraperitoneal bladder rupture.
All patients provided written informed consent to undergo the LESS procedure after they were given a detailed explanation of all available surgical options, namely, open surgery, laparoscopic surgery, or LESS, and the homemade nature of the single-port device. The patients were considered to be suitable for LESS on the basis of conventional inclusion criteria for conventional laparoscopic or robotic surgery, namely, they had isolated intraperitoneal bladder rupture and they voluntarily signed the written consent form after being informed of the objective, methods, effects, and risks of the procedure.
Patients were excluded if they were in a state of shock or had chronic heart disease, chronic obstructive pulmonary disease, cerebrovascular disease, and/or a history of hemorrhagic disease. The operative time, duration of hospital stay, duration of Foley catheterization, and the intraoperative and postoperative complications were recorded prospectively.
Operative technique
A homemade single-port device was prepared using a small Alexis® wound retractor (Applied Medical, Rancho Santa Margarita, CA) and a powder-free surgical glove (Triplex P-free Glove®; KM Healthcare, Guri, Korea), as described elsewhere. 14
General anesthesia was administered, and the patient was placed in a supine modified lithotomy position. A urethral Foley catheter was then inserted into the bladder. To avoid scarring, a crescent-shaped 2 to 3 cm incision was made along the lateral margin of the umbilicus. The wound retractor was then inserted at the site of the single incision by Hasson technique. The homemade single-port device was constructed by fixing and rolling the surgical glove to the outer ring of the wound retractor so that it would not fall off. Three fingers of the surgical glove were cut off. Two 12 mm trocars and one 5 mm trocar, or one 12 mm trocar and two 5 mm trocars, were then fixed using a silk 1-0 suture. A 10 mm rigid laparoscope (30°) was inserted through the middle 12 mm trocar, and the laparoscopic instruments were inserted through the other two trocars. Two flexible laparoscopic instruments (LaparoAngle®; CambridgeEndo, Framingham, MA) were inserted and configured in reverse alignments (“mirror-imaging”); conventional rigid instruments were used occasionally (Fig. 2). Intra-abdominal CO2 pressure was maintained at 12 mmHg. A 10 mm rigid laparoscope was inserted through one of the three trocars. Flexible laparoscopic instruments (LaparoAngle; CambridgeEndo, Framingham, MA) were inserted through the remaining two trocars. These laparoscopic instruments were passed into the abdomen through the single incision in a staggered manner.
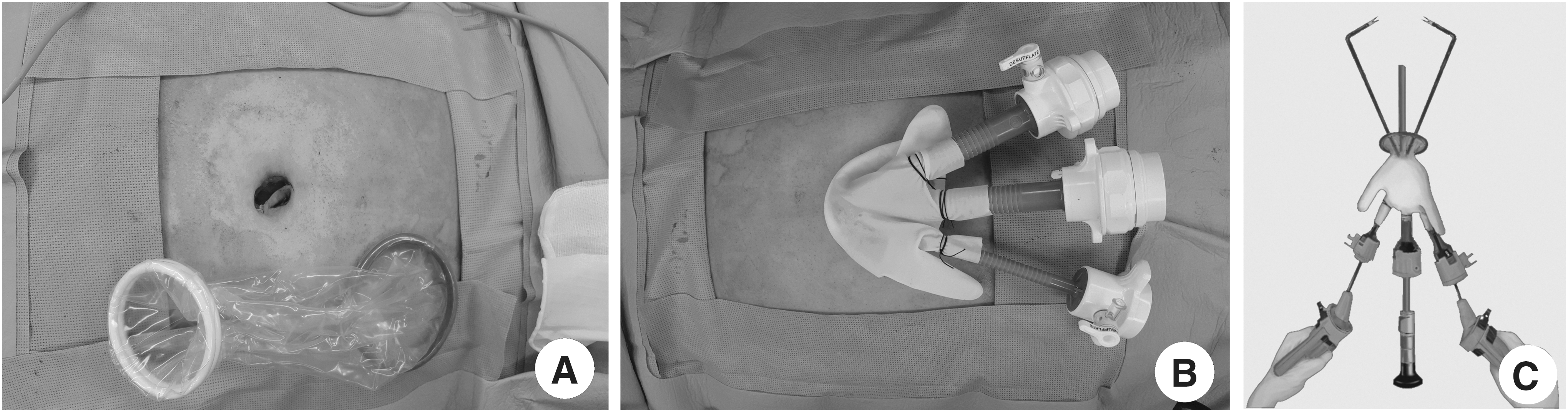
Laparoendoscopic single-site surgery for the repair of intraperitoneal bladder rupture.
The endoscopic instrument was placed on the rupture site to measure the length of laceration. The length of the measured section of the instrument was assessed with a sterilized paper ruler. LESS bladder rupture repair was performed by two-layer interrupted suturing with 4-0 polyglactin and 3-0 Vicryl (Fig. 3). A diluted indigo-carmine solution test was used after the suture was placed to confirm that the repair was watertight.
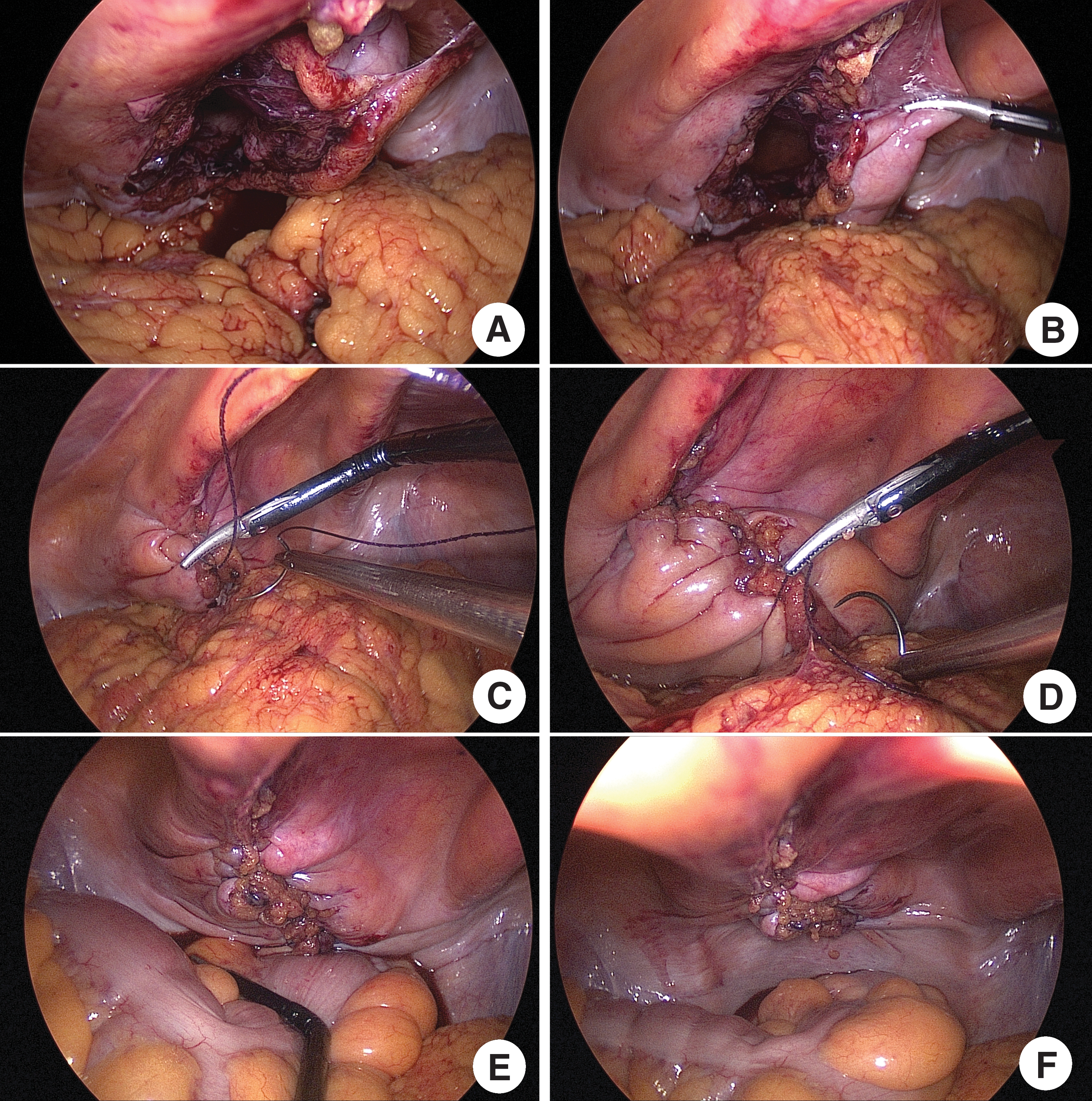
Laparoendoscopic repair of a bladder rupture.
After the repair of the bladder rupture using endosuction, the peritoneal cavity was irrigated and a careful examination was done. The operation was completed with Dermabond® skin closure without drain placement.
Follow-up
Cystography was conducted 7 days after surgery. If leakage was found on the cystography, cystography was repeated 7 days later. When leakage was not detected, the urethral Foley catheter was removed. Six months after surgery, the voiding symptoms were assessed and urine analyses were performed.
Results
In total, 22 patients underwent LESS for intraperitoneal bladder rupture during the study period. The patients were on average 40.50 ± 11.83 (range 19–63) years old. The male-to-female ratio was 8:2 (18 males, 4 females). The mean body mass index was 24.19 ± 2.61 kg/m2 (Table 1). The cause of bladder rupture was trauma (n = 21) or iatrogenic injury during previous pelvic surgery (n = 1). An iatrogenically injured patient had undergone open hysterectomy by Pfannenstiel incision, and bladder rupture was diagnosed at 4 days after hysterectomy to reduce operative pain and risk of wound complications (Table 1).
Iatrogenic bladder rupture: previous gynecology operation.
BMI = body mass index.
LESS repair of bladder rupture was completed effectively in all 22 patients. In all 22 patients, the abdominal viscera were intact, but there was urinary ascites in the rectosigmoid pouch. Laceration of the posterosuperior portion of the bladder was confirmed visually through a laparoscope. The mean diameter of the bladder rupture was 3.41 ± 1.01 (range 2–5) cm. The mean operative time was 89.05 ± 11.29 (range 76–122) minutes. The mean duration of hospital stay was 2.91 ± 0.53 (range 2–4) days. Estimated blood loss could not be evaluated because the bleeding was minimal.
After surgery, none of the patients required patient-controlled analgesia and none developed major complications. The urethral Foley catheter was removed 7.68 ± 2.08 (range 6–14) days after surgery (Table 2). Cystography was performed 7 days after surgery (Fig. 4). Twenty patients lacked extravasation. Consequently, their Foley catheter was removed on the same day. On a second cystography 7 days later (14 days after LESS), none of the two patients exhibited extravasation and their urethral Foley catheter was removed. None of the patients experienced postoperative voiding problems 6 months after LESS bladder rupture repair.

Cystography at 1 week after operation.
Discussion
Since operations that leave visible scars can affect a patient's quality of life, there is increasing interest in minimally invasive surgeries, including LESS or operations through natural orifices such as the rectum or vagina: all of these approaches have excellent cosmetic outcomes. 15 –17 Recently, many researchers in the urologic field have sought to devise minimally invasive surgical techniques for not only this merit of minimal invasive surgeries but for also less pain and short recovery periods, offering good cosmetic effects. 18
The first LESS procedures in the field of urology were reported in 2007 by Rane and colleagues and Raman and colleagues. Both authors independently used LESS to perform nephrectomy. 19 Subsequent reports demonstrate that LESS is a feasible and effective procedure for benign and malignant disorders of the adrenal glands, ureter, bladder, prostate, and testis. Moreover, it associates with high levels of patient satisfaction. 20 Thus, in general, LESS can be considered in all patients who are eligible for laparoscopic surgery if the procedure will be performed by a suitably experienced surgeon. 21 Indeed, a recent international multicenter study reported the use of LESS for managing a wide range of major urologic procedures, including pyeloplasty, simple nephrectomy, donor nephrectomy, radical nephrectomy, simple prostatectomy, partial nephrectomy, nephroureterectomy, renal cyst decortication, adrenalectomy, varicocelectomy, and ureterolithotomy. 18 Moreover, LESS has recently become increasingly popular worldwide for the treatment of benign and malignant diseases.
However, it is important to ensure that the patients are selected appropriately. In particular, LESS should be restricted to normal-weight patients with limited prior abdominal surgery who lack serious diseases. 22
To our knowledge, the use of LESS for urologic trauma has not been reported previously. The inclusion and exclusion criteria for LESS in cases of bladder injury should be similar to those used for benign urologic disease. In 1994, Parra described the first case of laparoscopic repair of an intraperitoneal bladder rupture following iatrogenic bladder injury. 6 The subsequent increase in experience and familiarity with laparoscopy has encouraged urologists to treat isolated intraperitoneal bladder rupture with a minimally invasive approach. 3
Kim and colleagues reported six such cases: all involved conventional laparoscopy and single-layer running suturing. 23 Notably, the authors concluded that the one-layer bladder closure approach was fast, safe, and effective when compared with the two-layer closure. However, conventional surgical management of intraperitoneal bladder rupture involves exploratory laparotomy and closure of the bladder in two layers with absorbable sutures. 24 Consequently, in the present study, LESS bladder rupture repair was performed using two-layer interrupted suturing. Although two-layer interrupted suturing may be more technically challenging than single-layer running suturing in LESS, the present study suggests that LESS with two-layer interrupted suturing is not inferior to conventional laparoscopy in terms of repairing bladder rupture. Specifically, when compared with conventional laparoscopy, LESS repair of bladder rupture at our three clinical centers was effective and associated with reasonable operative times (89 minutes on average), little pain (none of the patients required patient-controlled analgesia), and fast recoveries (the hospitalization stay was only 2.9 days on average) (Table 3). It was also safe, as no major complications were observed.
EBL = estimated blood loss; NS = nonspecified.
Moreover, a recent study by Park and colleagues comparing the patient-reported body image and cosmetic outcomes after LESS, conventional laparoscopic surgery, and open surgery for renal pathology showed that LESS associated with superior cosmetic outcomes. 25 Thus, it is likely that LESS for intraperitoneal bladder rupture also associates with better cosmetic outcomes than conventional laparoscopic surgery. These observations suggest that LESS may be more suitable than conventional laparoscopy or open laparotomy for patients with isolated intraperitoneal bladder rupture with no other traumas that require intra-abdominal surgery.
However, LESS does associate with some procedural difficulties. First, bladder repair suturing using a one-layer running or a two-layer interrupted suture is more difficult in LESS than in conventional laparoscopic surgery. 26 Moreover, our homemade single-port device is easily damaged by needles. 27
Despite there being some ready-made single-site ports, we used our homemade single-site port. With only Alexis wound retractors and surgical gloves, all institutions of the world can operate in single-site laparoscopic surgery with this port without difficulty.
This case series study has some limitations. First, although it involved three medical centers, the inclusion criteria were relatively narrow: we only performed LESS on patients with isolated bladder rupture who lacked chronic diseases. While these tight eligibility criteria were needed to determine the feasibility and safety for LESS repair of bladder rupture, they limit the generalizability of our observations to other patient populations. Thus, a large-scale comparative prospective study on LESS repair of intraperitoneal bladder rupture is warranted. Second, we had no control group, such as a traditional laparoscopic repair of bladder rupture group, to evaluate the pain scale and recovery periods. Nonetheless, LESS is one-step more minimally invasive surgery than traditional laparoscopic surgery. To overcome this limitation, we had assessed the previous studies about laparoscopic bladder ruptures, shown in Table 3. Also, we did not dissect the posterior bladder wall from its lining peritoneum for identification of the potential bladder rupture site. However, the potential rupture site was confirmed by a bladder filling test with diluted indigo-carmine solution after the repair. Nevertheless, the results of the present study suggest that the indications for LESS may be extended to include urologic trauma.
Conclusion
LESS repair was effective in all 22 patients with intraperitoneal traumatic or iatrogenic bladder rupture. Thus, LESS repair of bladder rupture using a homemade single-port device can be considered to be a feasible and safe alternative to conventional laparoscopy for carefully selected patients with hemodynamic stability.
Footnotes
Author Disclosure Statement
No competing financial interests exist.