
Abstract
Objective:
To assess the clinical efficacy of dual-lumen catheter technique in retrograde intrarenal surgery (RIRS) in terms of stone-free rate.
Methods:
The data of 172 patients who underwent RIRS for renal stones between 2010 and 2017 were retrospectively reviewed. Patients were classified into two groups depending on whether the dual-lumen catheter technique was used (group 1, n = 25) or not (group 2, n = 147) during RIRS. In turn, all patients of group 1 were compared with those of group 2 using propensity score analysis methods. Clinical variables, including post-RIRS residual fragments (RFs) (≥2 mm) and dusts (sandy stones) (≤1 mm), were compared between both groups. Logistic regression analyses were conducted to identify the predictors of postoperative RFs and dusts.
Results:
According to propensity score analysis, no other clinical variables were significantly different between the two groups, except the dust-free rate was significantly higher in group 1 than in group 2 (92% vs 40%, p < 0.001). In multivariate analysis, the performance of dual-lumen catheter technique was an independent predictor of the absence of dusts after RIRS (odds ratio [OR], 0.040; 95% confidence interval [CI], 0.070–0.220). In addition, on performing multivariate analyses in another matched population, it was found that although the technique adversely affected the removal of RFs (OR, 4.711; 95% CI, 1.203–18.447), it showed an excellent effect on the evacuation of dusts (OR, 0.049; 95% CI, 0.007–0.347).
Conclusion:
Our analyses suggest that the use of dual-lumen catheter during RIRS can facilitate the evacuation of sandy stones. However, further prospective randomized trials are required to verify the usefulness of this technique in real clinical practice.
Introduction
N
Because renal stones may adversely affect the quality of life of patients owing to deterioration of renal function resulting from stone-induced obstruction and stone-related pain, they are managed with various interventional modalities, such as extracorporeal shockwave lithotripsy (SWL), percutaneous nephrolithotomy (PCNL), and ureterorenoscopy (URS). Based on the recent introduction and development of endourologic instruments, such as flexible URS (fURS), ureteral access sheath (UAS), holmium laser fiber, and stone basket, in the management of renal stones, minimally invasive retrograde intrarenal surgery (RIRS) is currently being widely performed as the possible first-line treatment of choice, especially in medium-sized renal stones of 10–20 mm. 4 –6
The presence of residual fragments (RFs) after RIRS for nephrolithiasis may be stressful and a concern for both the physician and the patient given that RFs can cause flank pain, urinary tract infection, and obstruction. 7,8 Although there is no unified definition of stone- free status after RIRS, urologists have defined stone-free status as either no evidence of residual stone or the presence of tiny dusts and RFs <4 mm, usually considered clinically insignificant. 9,10 However, an ∼20% incidence rate of stone events has been reported, which requires additional intervention even in case of RFs 4 mm or less following RIRS. 7,11 Besides, we recently reported that even dusts (sandy stones), defined as measuring 1 mm or less, after RIRS showed a long spontaneous passage time (9.0 months) and a high probability rate of growth in size (∼18%) during the follow-up period, which emphasizes the importance of complete removal of dusts through irrigation for an adequate time during RIRS. 12
Therefore, in an effort to facilitate the evacuation of RFs and dusts, we have used the dual-lumen catheter for irrigation and suction of stone fragments or particles during RIRS in our current practice, and we have named it the “dual-lumen catheter technique.” In this study, we aimed to report the clinical efficacy of this technique in terms of achievement of stone-free status.
Materials and Methods
Study population
After obtaining the institutional review board approval from our institution for the study design and the use of patients' information, we reviewed the data of 172 patients who were treated with RIRS for renal stones by a single surgeon (S.Y.C.) between January 2010 and August 2017 at a single institution. Due to the retrospective nature of the study, the requirement for obtaining written informed consent from each patient was waived by the institutional review board. Patients were included in this analysis if the maximal diameter of the main stone ranged from 10 to 25 mm. The patients who had febrile urinary tract infection, bleeding diathesis, and anatomical anomalies, including musculoskeletal deformities, horseshoe kidney, ureteropelvic junction obstruction, and ureteral stricture, were excluded from the present study. Finally, among the total 172 subjects, a total of 25 patients (group 1) underwent RIRS using the dual-lumen catheter technique and the remaining 147 patents were assigned to group 2 as control.
Details for dual-lumen catheter technique during RIRS
The dual-lumen catheter is designed for over-the-wire placement, providing two separate working channels for second wire placement or contrast injection. The caliber and working length of dual-lumen catheter are 10F diameter and 54 cm, respectively. The diameter of each lumen is 0.038 inch for guidewire lumen (green portion) and 0.05 inch for injection lumen (yellow portion). The detailed explanations for RIRS performed at our institution have already been provided in our previous reports. 9,10 After all stones in the middle and lower calices are moved and gathered into the upper calix, stones are broken into small fragments by using holmium laser, and they are repeatedly grasped and retrieved from the kidney by using a stone basket. Next, the remaining stone fragments within the upper calix following the removal of stone fragments are further broken into tiny sandy stones (dusts) by using holmium laser, which cannot be removed with a stone basket owing to their small size. To perform stone dusting, the authors used the Lumenis® PulseTM and VersaPulse® PowerSuite™ 100 W laser systems as a laser machine. The holmium laser for stone dusting was set at lower energy pulse (0.2–0.5 J) and high-frequency rate (35–40 Hz). To evacuate the dusts, a dual-lumen catheter is used in group 1. One channel of the dual-lumen catheter is connected to the continuous irrigation system and the other channel is connected to the suction tube (Fig. 1A). The distal tip of the catheter is placed up to the renal pelvis and upper calix through an 11/13F UAS (Fig. 1B). Fine sandy stones within the upper calix are evacuated using 10 or more passes of alternating manual irrigation and suction, with a gentle back-and-forth motion to maximize the efficiency of evacuation (Fig. 2). The pressure or velocity of intraoperative irrigation pump was, respectively, set at 50–80 cm Hg or 1.0–1.5 L/minute to induce the floating of dusts by irrigation during evacuation. The timing of evacuation termination was determined at the discretion of the surgeon. Whereas after stone dusting using holmium laser following retrieval of stone fragments in group 2, the authors did not perform any additional procedures for removing stone dusts. Consequently, the authors expected the natural drainage of stone dusts along with urine passage within the urinary tract after surgery in group 2. The change of position to the Trendelenburg can aid in effective removal of stone dusts. An intraoperative Double-J stent is routinely indwelled at the end of surgery in almost all patients.
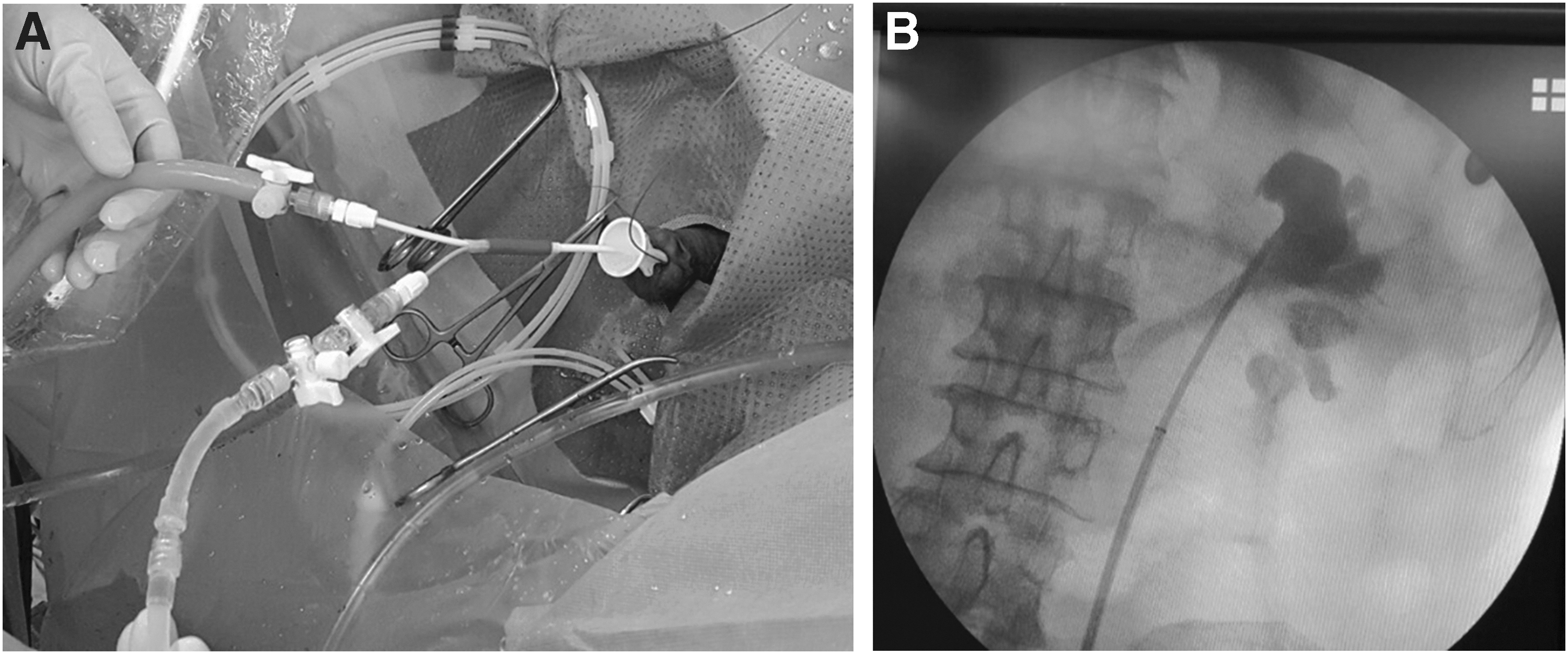
The use of a dual-lumen catheter during retrograde intrarenal surgery.
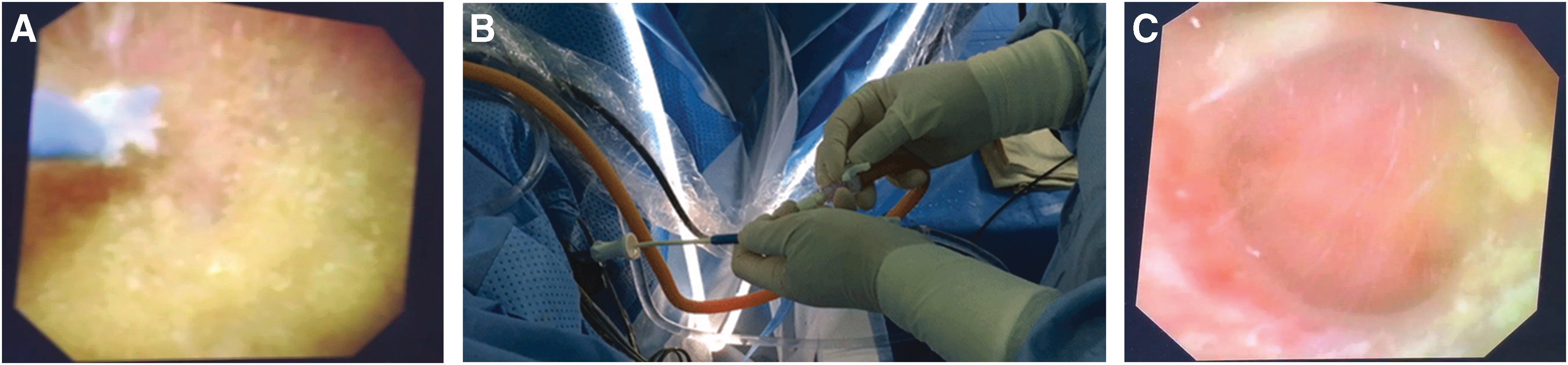
The process of dual-lumen catheter technique for the evacuation of dusts during retrograde intrarenal surgery.
Assessed clinical variables
The authors investigated the following patient-related parameters: age at surgery, gender, body mass index, comorbidities, including diabetes and hypertension, serum creatinine level, estimated glomerular filtration rate, and serum hemoglobin level. The stone-related parameters evaluated were as follows: previous treatment (SWL/URS/PCNL), history of urinary stone, presence of preoperative hydronephrosis, preoperative Double-J stenting, stone laterality, the number of stones, maximal stone size, total stone volume, infundibulopelvic angle, Hounsfield unit, and stone composition. Total stone volume was presented as the sum of each stone volume, which was calculated as 0.523 × length × width × height (mm3) measured on preoperative CT. Hounsfield unit was measured by using an ellipsoidal region of interest on the axial images of CT scans. Intra- and postoperative parameters, including operation time, intraoperative Double-J stenting, hospital stay, Double-J stent indwelling period, postoperative complications (fever/acute pyelonephritis/sepsis), and presence of RFs and dusts, were also recorded.
Preoperatively, all patients received a nonenhanced CT scan and kidney, ureter, and bladder radiography to examine the location, the number of stones, stone density, and size of the stones. Within 1 month after the planned RIRS, nonenhanced CT scan was performed in patients to assess the presence of RFs and dusts. The main outcomes of interest in this study were the presence of postoperative RFs and dusts depending on the application of dual-lumen catheter technique during RIRS. We defined RFs as particles measuring 2 mm or more. Sandy stones (dusts) were defined as tiny remnant particles with maximal diameter ≤1 mm.
Statistical analyses
To adjust for the impact of variables other than the dual-lumen catheter technique that may influence the stone-free rate (SFR), propensity scores were calculated for each subject using multivariate logistic regression based on gender, the number of stones, stone size, and stone laterality. Next, we matched the 25 patients (group 1) with the remaining patients (group 2) in a 1:2 ratio based on propensity score analysis. Consequently, group 1 included patients who received the dual-lumen catheter technique during RIRS and group 2 included patients who only underwent RIRS without the dual-lumen catheter technique. Finally, we compared the baseline variables between the two groups using nonparametric statistics within the propensity score-matched population. Continuous variables were recorded as median and interquartile range and compared by using the Mann–Whitney U test. Categorical variables were expressed as absolute number and percentages and compared by using the chi-square test and Fisher's exact test. Univariate and multivariate logistic regression analyses were conducted to assess the factors associated with the presence of dusts. All statistical analyses were performed with IBM SPSS ver. 21.0, all tests were two sided, and p < 0.05 was considered statistically significant.
In addition, considering the number of missing data observed after propensity score matching, we adopted the inverse probability weighting (IPW) method for the entire population to maximize the use of raw data. 13,14 Each patient was weighted by the inverse probability of being treated by RIRS using the dual-lumen catheter technique or conventional RIRS. The probability of being “assigned” to a particular treatment was calculated using multivariate logistic regression models based on several variables, including age, gender, stone laterality, stone size, and the number of stones. Generally, the size of the pseudopopulation obtained by the IPW is much bigger than that of the original population, which may induce false-positive results. Therefore, to adjust this limitation of the IPW, we used the stabilized weight (SW) method to construct a pseudopopulation similar to the size of the original population. 15 Next, multivariate logistic regression analyses were performed to evaluate the predictors of the presence of RFs and dusts in the pseudopopulation created by the SW. All statistical analyses were carried out using SAS 9.3 (SAS Institute, NC), all tests were two sided, and statistical significance was set at p < 0.05.
Results
Results of comparative analyses between the two groups
In the prepropensity study cohort (n = 172), the maximal size (20 mm vs 14 mm, p < 0.001) and total volume of stones (2092 mm3 vs 925.7 mm3, p < 0.001) in group 1 were significantly larger than those in group 2 (Supplementary Table S1; Supplementary Data are available online at
To minimize selection bias, patients in group 1 were matched with those in group 2 at a 1:2 ratio based on the propensity scores calculated for several variables such as gender, the number of stones, stone size, and stone laterality. Consequently, the population size after propensity score matching was 75. Table 1 summarizes the clinical characteristics of the postpropensity population. After propensity score matching, there were no significant differences in patient- and stone-related characteristics, including maximal stone size and total stone volume, between the two groups. Other surgery-related parameters, such as operation time, hospital stay, ureteral stent indwelling period, and postoperative complications, did not differ significantly between both groups. With respect to postoperative SFRs, the RF-free rate was not significantly different between the two groups (72% vs 88%, p = 0.109), but dust-free rate was significantly higher in group 1 than in group 2 (92% vs 40%, p < 0.001).
Patient and Stone Characteristics After Propensity Score Matching
GFR = glomerular filtration rate; IQR = interquartile range; n.s. = nonsignificant; PCNL = percutaneous nephrolithotomy; SWL = shock wave lithotripsy; URS = ureterorenoscopy.
Results of logistic regression analyses
On performing logistic regression analyses in the postpropensity population, the use of dual-lumen catheter was significantly associated with the absence of postoperative dusts (odds ratio [OR], 0.058; 95% confidence interval [CI], 0.012–0.274, p < 0.001) (Table 2). Moreover, this correlation was significantly maintained after multivariate regression analysis adjusting for other covariates (OR, 0.040. 95% CI, 0.070–0.220, p < 0.001), implying that the use of dual-lumen catheter during RIRS may promote the evacuation of tiny sandy stone particles.
Logistic Regression Analysis Results Predicting the Presence of Dusts in the Entire Propensity Score-Matched Cohort (n = 75)
CI = confidence interval; OR = odds ratio.
Given that there were a large number of unmatched patients (n = 97) after propensity score matching, the authors used the SW method to estimate the pseudopopulation similar to the scale of the original study cohort for the purpose of maximizing the use of raw data. Consequently, the population size estimated by using the SW method was ∼168, consisting of 149 patients in the conventional RIRS group and 19 patients in the RIRS group using dual-lumen catheter technique. Table 3 presents the results of multivariate logistic regression analyses conducted in this pseudopopulation. Notably, for evacuating stones during RIRS, although the use of dual-lumen catheter might adversely affect the presence of postoperative RFs (OR, 4.711; 95% CI, 1.203–18.447, p = 0.026), it showed an excellent association with the absence of postoperative dusts (OR, 0.049; 95% CI, 0.007–0.347, p = 0.003).
Multivariate Logistic Regression Analysis Results Predicting the Presence of Residual Fragments and Dusts in the Pseudopopulation Made by Stabilized Weight (n = 168)
RF = residual fragment.
Discussion
There are various treatment options in the management of renal stones, especially medium-sized stones ranging from 1 to 2 cm. Depending on the current guideline, although SWL is usually regarded as the treatment of choice and it achieves good SFRs for medium-sized renal stones, RIRS, minimally invasive renal stone surgery using fURS, can be a good alternative therapeutic option that shows comparable SFRs to SWL in case of patients who have unfavorable factors for SWL, including steep infundibulopelvic angle, long lower pole calix, and radiolucent stones. 16 In addition, over the past few decades, therapeutic approaches for medium-sized renal stones have consistently evolved with the adoption and development of novel technologic and treatment advances, 6 and therefore, urologists' interest in RIRS using fURS has increased. In a questionnaire-based survey study, the majority of endourologists (60%–70%) considered fURS as the first-line treatment modality for renal stones <2 cm and lower pole calculi. 4 Also, according to the report analyzing the surgical trend for renal stones in the United States, there was a steady increase in the use of URS from 40.9% to 59.6% and a corresponding decrease in the use of SWL from 54% to 36.3% between 2003 and 2013. 5
Thus, RIRS using fURS is currently being widely used as an effective therapeutic modality in the management of renal stones. The goal of RIRS is to actively remove the fragments as much as possible as well as to break the stones into fragments, because these fragments have the potential to act as a nidus for stone regrowth, stone recurrence, stone-related complications, including urinary tract infection and obstruction, resulting in the need for additional intervention. 17,18 However, a consensus has not been reached thus far with respect to the definition of the size of fragments requiring active removal during procedures for renal stones. Historically, in reference to SWL, fragments ≤4 mm that were nonobstructing and asymptomatic were considered “clinically insignificant residual fragments (CIRFs),” which were expected to have a high likelihood of spontaneous passage and low rates of retreatment. 17,19 However, this term has been regarded as a misnomer as several follow-up studies of CIRFs after multiple procedures, including SWL, PCNL and RIRS, for renal stones showed significant rates of reintervention caused by stone-related events and complications. 11,17 –21 A recent survey analysis targeting endourologists suggested that the majority of respondents (71.3%) defined the clinical stone-free state as 2 mm or smaller. 4 In addition, in our recent report investigating the natural history of remnant particles after RIRS, it was found that even dusts, defined as measuring ≤1 mm, showed a long spontaneous passage time (9.0 months) and a high likelihood of growth in size (∼18%) after the 2-year follow-up period. 12
Therefore, we strongly recommend thorough evacuation of the RFs and dusts during RIRS to attain complete stone-free status. To achieve this goal, the authors used a dual-lumen catheter and named the method “dual-lumen catheter technique.” To the best of our knowledge, our study is the first report on this technique because the authors introduced this method for the first time. The dual-lumen catheter can aid in irrigation and suction of the remnant particles during RIRS as a hybrid approach. In our practice, the authors first break the stones into pieces that are not dust particles but are still small enough (2–3 mm) to be collected with use of the dual-lumen catheter. The procedures can be completed by evacuating all remaining fine particles as in the dusting procedure. Multivariate regression analyses in the present study supported the claim that this technique had an excellent effect on the evacuation of dusts. However, the use of dual-lumen catheter had an adverse effect on removal of RFs. These results may be attributable to the luminal diameter of the dual-lumen catheter, which may be large enough to evacuate dusts, but not large enough to remove the RFs. Because the data included the initial experience of trial and error, the dual-lumen catheter technique may seem to have an adverse effect on removal of RFs. Thus, the authors recommend complete removal of RFs using a stone basket before the application of dual-lumen catheter technique at the time of RIRS.
Major drawbacks of the current study are as follows: First, despite a comparative analysis between the two groups, there was a lack of randomization process due to the retrospective nature of the study. Because the study population was divided into two groups depending on the use of dual-lumen catheter technique, a possible selection bias cannot be strictly excluded. To minimize this selection bias, the authors implemented 1:2 matching based on propensity scores for the adjustment of several variables, including gender, the number of stones, stone size, and stone laterality. Consequently, the distribution of clinical variables showed no statistically significant differences between both groups after matching. Second, the sample size of the study cohort may seem to be small (n = 172) and there were a number of missing data (n = 97) after propensity score matching. To overcome this limitation, the authors used the IPW and SW statistical methods to increase the sample size and to maximize the use of raw data, 13 –15 which resulted in a sufficient number of subjects in the pseudopopulation. As a result, the results of multivariate regression analyses performed in the pseudopopulation corresponded to those conducted in the propensity score-matched population.
Conclusions
Our data suggest that the use of dual-lumen catheter during RIRS for renal stones can facilitate the evacuation of tiny dusts, which may contribute to the achievement of complete stone-free status. However, additional well-designed, prospective randomized trials are needed to confirm the usefulness of this technique in real clinical practice.
Footnotes
Authors' Contributions
Conception and design: H.S.K., S.Y.C.; data acquisition: H.S.K., S.Y.C.; data analysis and interpretation: H.S.K., S.Y., S.Y.C.; article drafting: H.S.K.; critical revision of the article for scientific and factual content: S.Y.C.; statistical analysis: H.S.K., S.Y., S.Y.C.; supervision: S.Y.C.
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.