
Abstract
Objective:
To establish whether the regular biopsy of red patches (RPs) seen during endoscopic surveillance for bladder cancer is worthwhile and determine a suitable time frame for repeat biopsy of prior histologically benign persistent RPs in patients on endoscopic surveillance for bladder cancer.
Patients and Methods:
Four thousand eight hundred five flexible cystoscopy (FC) reports over a 12-month period were retrospectively reviewed at a United Kingdom tertiary teaching hospital and those undergoing cystoscopic surveillance for bladder cancer and found to have solitary RPs at FC were included in the study. A proportion of these cases had biopsies taken for histopathologic analysis.
Results:
Two hundred forty-one FC performed on 183 patients on endoscopic surveillance for bladder cancer had RPs and 120 (49.8%) of them had previous intravesical Bacillus Calmette–Guerin therapy. Eighty-five patients (35.3%) underwent biopsy of the RP. Malignancy was found in 20 biopsies (23.5%), of which, 11 out of 20 (55%) were carcinoma in-situ. Sixteen of these recurrences were biopsied previously, of which 11 (68.8%) were benign at last biopsy, 6 of which were in the last 12 months. The remaining four recurrences had no previous biopsy. No cases of malignancy were identified in patients with low-risk bladder cancer.
Conclusion:
We recommend the biopsy of all RPs found during endoscopic surveillance of patients with intermediate-/high-risk bladder cancer due to the significant incidence of malignant recurrence identified, particularly if no biopsy has been performed within the previous 12 months. This is independent of previous biopsy histology.
Introduction
W
Patients and Methods
We performed a retrospective review of 4805 FC reports over a 12-month period. All reports on patients under follow-up for bladder cancer with descriptive terms of the urothelium such as: red patch, redness, red area, erythema, erythematous, or angry-looking were included in the study, as were patients with history of intravesical BCG treatment. Patients with concomitant papillary mucosal lesions or bladder calculi, long-term catheters or features of telangiectasia were excluded. A proportion of RPs underwent biopsy either via flexible or rigid cystoscopy (RC), and the histologic findings were documented.
Results
A total of 409 FC reports documented the appearance of RPs in the bladder, and of these, 241 (58.6%) were found in 183 patients undergoing endoscopic surveillance for bladder cancer. The remaining RPs were found in patients under investigation for hematuria, recurrent urinary tract infections, and troublesome lower urinary tract symptoms (Table 1). All patients had urine dipstick testing immediately before cystoscopy and were clear of infection.
LUTS = lower urinary tract symptoms; RPs = red patches; UTI = urinary tract infection.
Median age was 73 years (37–92) with 205 males (85.1%), 36 females (14.9%) in the endoscopic surveillance cohort, and 120 RPs (49.8%) were found in patients with a history of intravesical BCG therapy. Overall, 85 out of 241 patients (35.3%) had their RP biopsied—32 (13.3%) had an immediate biopsy at FC and 53 (22.0%) underwent a RC and biopsy under general/regional anesthesia. Sixty patients (24.9%) were not biopsied immediately but instead brought back 4 to 6 weeks later for a repeat FC, sooner than their usual follow-up protocol required (Table 2). On this repeat FC, one case of CIS and two cases of high-grade TCC were diagnosed; 33 continued routine endoscopic surveillance, 11 had inflammation on biopsy, 5 had spontaneously resolved, and 8 patients did not attend follow-up. These findings are included in the final analysis below. The most common biopsy finding was inflammation found in 21 out of 32 RP biopsies (65.6%) at FC and 24 out of 53 RP biopsies (45.3%) at RC, 52.9% overall. There were 189 (78.4%) RPs found in patients on follow-up for high-risk bladder cancer with just 5 cases (2.1%) on follow-up for G1pTa TCC.
Request rereferral from primary care if persistent visible or nonvisible hematuria.
BCG = Bacillus Calmette-Guerin; CIS = carcinoma in-situ; FC = flexible cystoscopy; GA = general anaesthetic; TURBT = transurethral resection of bladder tumor.
Bladder cancer recurrence was found in 6 out of 32 patients (18.8%) at FC, all with initial intermediate-/high-risk disease: 5 cases of CIS recurrence and one case with G3pTa with CIS in a 69-year-old man who had undergone previous radical external beam radiotherapy for G3pT2 bladder cancer. Malignant recurrence was also found in 14 patients (26.4%) who underwent RP biopsy at RC following detection by FC (Table 3). They consisted of 6 cases of CIS, two cases of G3pT1, four cases of G3pTa, and two cases of G2pTa. Similarly, all 14 had intermediate-/high-risk bladder cancer at first diagnosis.
TCC = transitional cell carcinoma.
In total, 20 malignant recurrences were identified giving an overall bladder cancer recurrence pick-up rate of 23.5% for RPs biopsied during endoscopic surveillance—17 males (85.0%) and 3 females (15%); and 12 patients (60%) had a history of BCG treatment. No patients on low-risk endoscopic surveillance for bladder cancer had malignant histology following RP biopsy nor did any patients younger than the age of 67 years. Sixteen of these recurrences had been biopsied previously, of which 11 (68.8%) were benign at last biopsy, 6 of which were in the last 12 months. The remaining four recurrences had no previous biopsy since diagnosis at first transurethral resection. Seven out of 16 RPs biopsied (43.8%) diagnosed with bladder cancer recurrence were found in patients who had a previous bladder biopsy within the last 6 months (Fig. 1)—two of which were malignant and 5 benign at last biopsy. All five patients who had malignant histology at their last biopsy within the last 12 months again had malignant recurrence at repeat biopsy of the RP; and all five patients who had their last bladder biopsy performed over 12 months ago had benign histology on latest RP biopsy. Finally, there were no complications such as troublesome hematuria, clot retention sepsis, or pain in patients biopsied, even those which were performed with FC under local anesthesia.
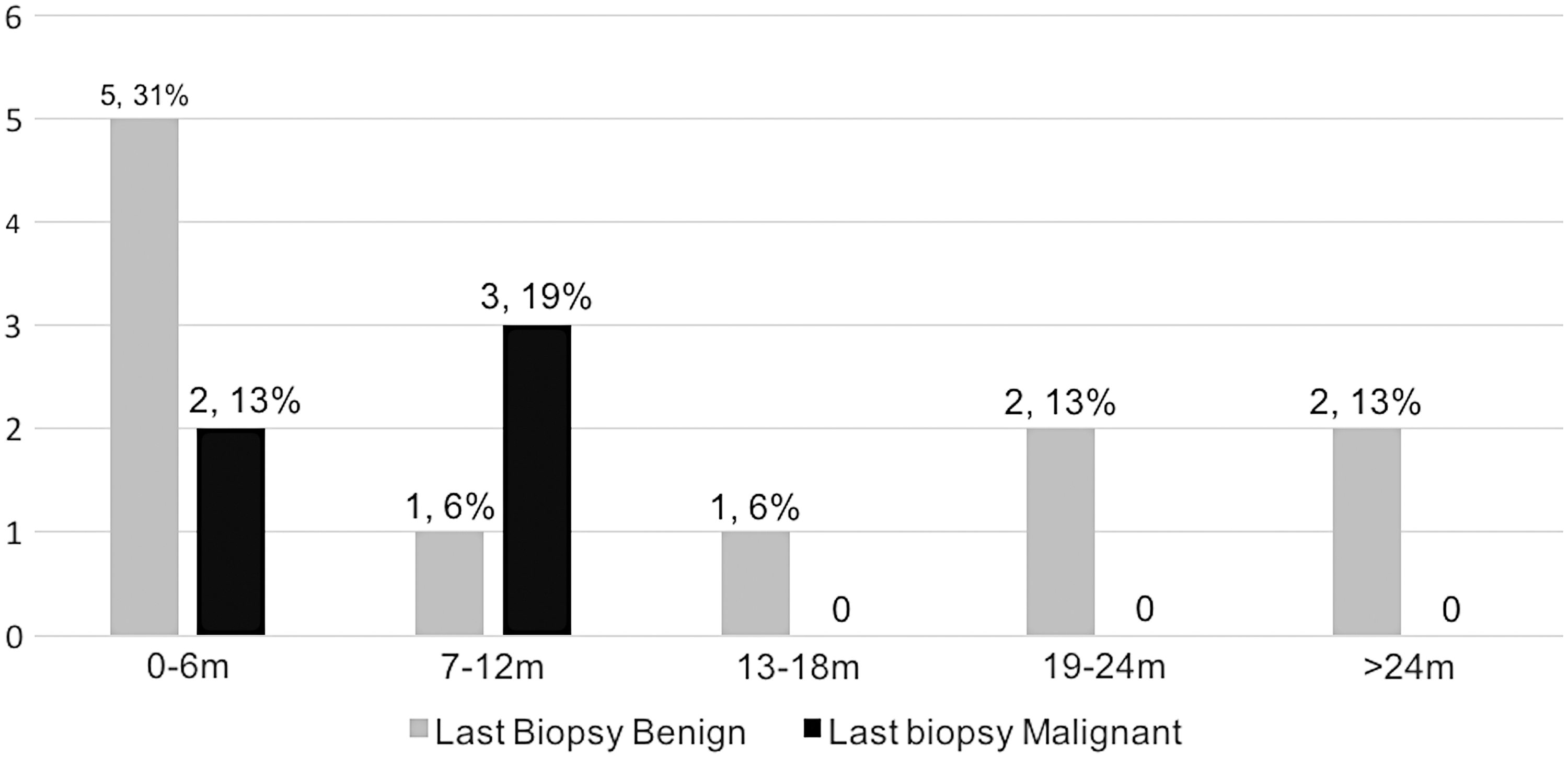
No. of cancers identified in relationship to duration since last biopsy (months) and histology at last biopsy. Total with previous biopsy data was 16 with percentage also given.
Discussion
The endoscopic diagnosis of bladder cancers, which are not always visible at white light cystoscopy (e.g., CIS) as well as distinguishing benign from malignant isolated RPs within the bladder, remains a challenge for many urologists. Several new applications are currently available to solve this problem, however, not all centers in the United Kingdom currently have access to them. Photodynamic diagnostics via RC using blue light and hexaminolevulinate is available in the United Kingdom and already well documented to increase detection and reduce recurrence of nonmuscle invasive bladder cancer, 3 but is not used in routine practice in our department nor is the routine use of urine cytology. This technique requires general/regional anesthesia for use with a rigid cystoscope, so is often not seen as a logistically or economically viable option. Narrow-band imaging, on the contrary, can be used via flexible and rigid cystoscopes and has been shown to improve tumor detection, resection, and recurrence. 4
The overall cancer detection rate in this study was high at 23.5%, more than double that was found in a similar study by Swinn and colleagues. 5 This may be due to differences between the two populations of patients and their primary histologic diagnosis, but likely due to differences in study methodology. For example, although it is not specifically stated whether this was a prospective or retrospective data collection, the authors identified 1088 patients who underwent cystoscopy (compared with 4805 in our study), and within this cohort, 193 RPs were found and biopsied in 167 patients. When analyzed for only patients on endoscopic surveillance, 138 RPs were found and biopsied with 16 malignancies identified, giving a cancer detection rate of 11.6%. Our study, being a retrospective one, meant that we could only analyze histology results of RPs which were biopsied. The RP biopsy rate was 32.4%, which could mean that there were clinical operator-dependent reasons for not proceeding with biopsy in the remaining 67.6% of cases. The likelihood is that the RPs were not biopsied because they were thought not to look particularly sinister at the time of FC, hence, our higher detection rate of malignant histology in those that were biopsied. The study of Swinn and colleagues similarly did not diagnose any malignancies in patients younger than the age of 60 years, despite similar average age and age ranges in the two studies. However, this is most likely due to bladder cancer being a disease of older people, and less than a third of patients biopsied in the study were younger than this age. Nevertheless, the differences between the two studies are likely to be multifactorial, with a low RP biopsy rate in our study and smaller overall numbers in the aforementioned study contributing factors.
The incidence of RPs and malignant recurrence was almost six times more common in men than women in this study (Table 1)—17 males and 3 females diagnosed with malignant recurrence—despite the United Kingdom bladder cancer incidence being only 2.7 times more common in men. 6 This may be due to sampling artefact of the study, in that, possibly men are more likely to have RPs in the bladder because of incomplete bladder emptying due to the presence of the prostate, particularly after administration of intravesical BCG. This may lead to more urothelial reaction and, hence, increased occurrence of RPs at surveillance cystoscopy. Furthermore, 12 out of 20 (60%) malignant recurrences identified were in patients who had previous intravesical BCG immunotherapy. Thus, more men will be biopsied making it more likely to diagnose recurrence men than women. However, a prospective study with biopsy of all RPs seen in such a cohort is required to clarify this finding.
In a similar study by Fernando and colleagues, they retrospectively examined the results of 50 patients who underwent cystoscopy for hematuria and lower urinary tract symptoms only and had their RP biopsied. They did not include patients with a history of bladder cancer. They found four patients (8%) to have CIS, of whom urine cytology was positive in only two of them. 7 It has been reported that urine cytology has a sensitivity of 48% (16% for low-grade and 84% for high-grade tumors) and specificity of 86%. 8 A study by Dalbagai and colleagues evaluated cystoscopy findings at 3 months in patients who received intravesical BCG. Interestingly, urothelial carcinoma was found in 5 of 11 patients, with RPs and positive urine cytology compared to none of 37 with RP and negative cytology, 9 suggesting that biopsy is only required if urine cytology is positive. Our retrospective analysis revealed that not all patients had urine cytology performed, and from the evidence described above, positive findings in association with isolated RPs would mandate immediate biopsy, and negative cytology could spare some patients from undergoing biopsy. However, the negative predictive value remains unclear from the relatively small numbers (n = 37) included in that study, in whom no malignancy was identified after RP biopsy with negative cytology. Nor can we safely assume that negative cytology in the presence of an RP means it is benign, as most of the patients in our study had not just had induction BCG, and so the study population is different. Ideally, a larger more robust prospective study of all patients on endoscopic surveillance is required to answer this question.
This study suggests that the cancer detection rate is higher for RC compared with FC (26.4% vs 18.8%). This may be a true finding attributed to the clearer images and more robust biopsy equipment that a rigid instrument offers. On the contrary, it could be due to bias on the part of the endoscopist, as there may be an instinct to perform biopsies of RPs, which look more severe for a rigid biopsy rather than attempting one via FC.
Currently, persistent RPs are being biopsied without any formal protocol of guidelines. Overall, 11 cancers (55%) were picked up in patients who had bladder biopsies within the last 12 months, and 7 of these were benign at last biopsy (Fig. 1). Hence, if RPs persist, rebiopsy is worthwhile.
Conclusions
This study yielded a positive predictive value for bladder cancer recurrence at RP biopsy of 23.5%, therefore, we advocate the routine biopsy of RPs in patients undergoing endoscopic surveillance of intermediate-/high-risk bladder, particularly, if no biopsy has been performed within the last 12 months.
Footnotes
Acknowledgment
Our thanks go to Tracy Pringle, Urology Department Administrator, for her assistance in this study.
Author Disclosure Statement
No competing financial interests exist.