
Abstract
Background:
The incidence of spina bifida (SB) is ∼1:1000, and risk of stone disease is substantially raised in SB. This is the unique published study of the outcome of patients with SB undergoing percutaneous nephrolithotomy (PCNL) compared to a neurologically intact historically matched control group at the same institution.
Patients and Method:
A series of 96 PCNLs in 13 SB and 50 non-SB patients was analyzed. The following measurements were recorded: (1) Comorbidities; (2) Preoperative: (renal function, American Society of Anesthesiologists [ASA] score); (3) Intraoperative: (anesthesia time, number of tracks, stone-free rate); and (4) Postoperative: (sepsis, intensive therapy unit and total length of stay, transfusion rate, stone composition, rate of stone disease-related nephrectomy).
Results:
Retrograde access to the ureter was impossible in all cases of SB. The median ASA grade (OR 10.5, 95% confidence interval [CI] 2.6–42.7) and operative time (median difference 30 minutes, 95% CI 20–40) were both higher in the SB cohort. Surgeon's estimate of stone-free rate was significantly lower in the SB cohort (46% vs 82%). Intensive care requirement (0.29 days/PCNL vs 0.1 days/PCNL); total hospital stay (7 days vs 4 days); postoperative transfusion rate (11.8% vs 1.6%); and sepsis rate (38% vs 1.6%) were all significantly higher in the SB group. Repeat PCNL and nephrectomy for recurrent stone disease were both significantly increased in SB cohort compared to control group.
Conclusions:
PCNL in patients with SB is associated with multiple parameters of poor outcome. Patients with SB should be counseled about increased peri-operative risk and likelihood of stone recurrence. In an era where hospitals are judged according to comparative outcomes, a case may be made for comparing PCNL in this cohort of patients separately because of the significantly increased peri- and postoperative morbidity.
Introduction
U
In addition to dietary factors, stone formation is associated with a number of risk factors including neurological dysfunction of the urinary tract. 1,2,6 Spina bifida (SB) is a major contributor to this latter group. SB represents a spectrum of disease in which the neural tube fails to close, resulting in variable caudal neurological impairment affecting function of lower urinary tract, large bowel, and lower limb somatosensory function. 7
This is the first consecutive case–control study of patients that addresses peri- and postoperative outcome of PCNL in patients with SB undergoing PCNL with historically matched controls with particular reference to perioperative morbidity, technical challenges of surgery, and postoperative outcome reported to date.
Patients and Methods
All patients with a diagnosis of SB undergoing operative intervention for urinary tract calculi were retrospectively reviewed and historically matched with a cohort of neurologically intact patients undergoing PCNL. All PCNLs at our institution have been prospectively recorded and controls were randomly chosen from this database to provide a historically matched control cohort. Case notes were reviewed and data recorded. All surgical procedures relating to stone disease were recorded, in addition to medical and surgical past history. PCNL on both SB and non-SB patients was performed to a standard protocol in our institution with patient prone in “swimmer's position” (arm raised on ipsilateral side of stone). Puncture was performed by sub-specialist uro-radiologist with dilute contrast containing methylene blue available via ureteric catheter placed supine immediately before patient repositioning for PCNL. Access was obtained using fluoroscopy and/or ultrasound (US) scanning according to radiologist preference. Detailed analysis was undertaken on all PCNLs. Surgical and anesthetic records were used to obtain preoperative serum creatinine, time under anesthesia, American Society of Anesthesiologists (ASA) score, surgeon assessment of stone-free status, and number of percutaneous tracks required for each PCNL. Intra- and postoperative complications (pyrexia >38°C, culture-positive sepsis, blood transfusion rate) were recorded, along with length of admission to intensive care unit (ICU) and total length of hospital stay. Stone-free rates were additionally assessed from postoperative imaging. Because of the nature of this retrospective study, the method of imaging was variable (unenhanced CT, US, and/or intravenous urogram).
Statistical methods
Many patients in the dataset had more than one operation, leading to possible correlated outcomes. To avoid double counting, analyses were performed in two ways: first by initial operation only and second including data from all operations. For the set of analyses including all data each observation from within a patient was weighted by the reciprocal of the number of observations for that individual. SB and control groups were compared using different methods to suit the type of data as follows. Variables were described using number (%) for categorical variables, mean (standard deviation) for normally distributed continuous variables, and median (25–75 centile) for non-normal continuous variables; respective analyses give mean difference (along with 95% confidence interval [CI] from a t distribution), median difference (along with rank-based 95% CI) and odds ratios (ORs) or proportional cumulative ORs along with 95% CI derived using logistic regression or ordinal logistic regression respectively. Analyses were performed using Stata® version 11 (StataCorp, College Station, TX).
Results
Preoperative
The overall study consisted of 96 PCNLs performed on 63 patients (13 patients with SB and 50 neurologically intact controls). The total SB cohort numbered 17, but of these, four patients had stone surgery that did not include PCNL. Thirteen patients with SB had a total of 34 PCNLs. The SB cohort had a markedly different distribution of stone procedures compared to control (Table 1). Because of variability in preoperative imaging, it was not possible to derive a precise score for the complexity or volume of stone.
FURS = flexible uretero-renoscopy; PCCL = percutaneous cystolithotomy; PCNL = percutaneous nephrolithotomy; SB = spina bifida; SWL = shock wave lithotripsy.
Preoperative difficulties in the two patient cohorts were summarized into different groups (Table 2), which revealed a high frequency of problems largely, or completely, confined to the SB cohort. Every patient with SB had either had an ileal conduit diversion, or had an anatomically abnormal bladder (augmentation cystoplasty with or without bladder closure and Mitrofanoff diversion), which meant that ureteric catheterization from below was not attempted or successfully achieved before PCNL. Some centers perform ureteric access as a separate prior procedure (i.e., percutaneous cystotomy and ureteric catheter placement) but this is not standard practice at our institution. Mean age was 22 years younger in the SB group (95% CI 15–28), and the SB cohort were more likely to have a high ASA (OR 10.5, 95% CI 2.6–42.7). There were no significant differences in serum creatinine at preassessment before surgery.
Patient with previous treatment for posterior urethral valves.
ACE = antegrade continent enema; UTIs = urinary tract infections; VP = ventriculo-peritoneal.
Intraoperative
Operative time was significantly longer in the SB group (median difference 30 minutes, 95% CI 20–40; Fig. 1). Despite the increased number of tracks, and longer anesthesia time, the surgeon-reported stone-free rate (a combination of nephroscopy and image intensifier screening intraoperatively) at the end of the operation for SB patients undergoing PCNL was 46% compared to 82% in the control group. It should be emphasized that as a tertiary referral center, the neurologically intact control group tend to have stones of above average complexity. As such a lower stone-free rate would be anticipated when compared to national averages. Subset analysis of single track PCNLs in the control cohort demonstrated a stone-free rate of 37/40 (92.5%).
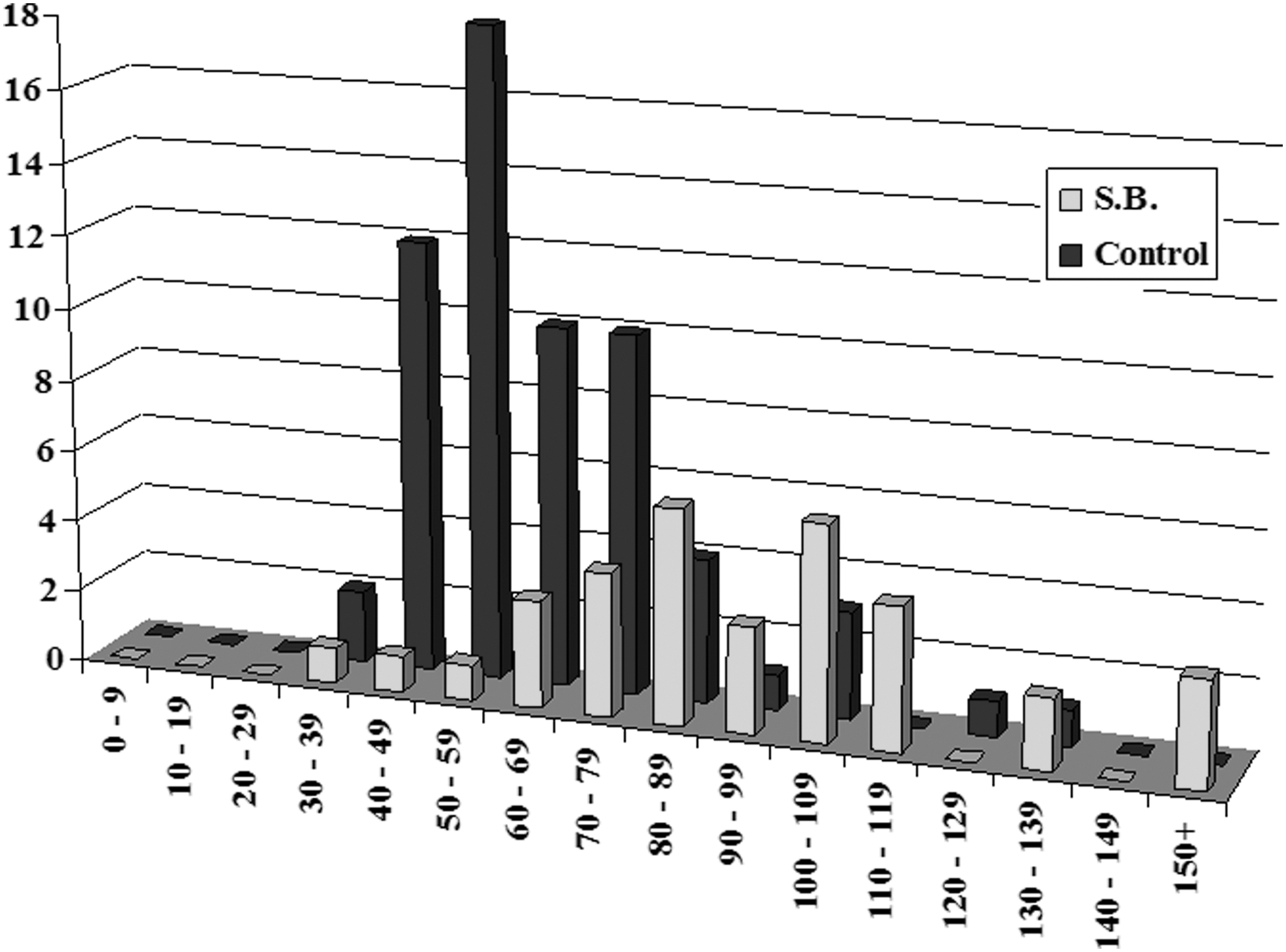
Anesthesia time for PCNL in SB cohort (red) compared to control group (blue). y-Axis frequency (number); x-axis time (minutes). PCNL = percutaneous nephrolithotomy; SB = spina bifida.
Intraoperative problems recorded in the operative record occurred in 8 of 34 PCNLs performed in the SB group (23.5% of cases), of which 6 were surgical and 2 anesthetic. The surgical intraoperative difficulties encountered were bleeding sufficient to impair location of stone (n = 3), renal pelvic perforation (n = 1), and difficult access as a consequence of distortion of normal anatomy (n = 2). The two anesthetic complications were slipped endotracheal tube (n = 1) and intraoperative aspiration on induction leading to the surgery being abandoned (n = 1). This compares to 3 cases of intraoperative difficulty in 62 PCNLs (4.9% of cases) in the control group (bleeding and poor view in all cases). This gave a significant OR of 6.1 (95% CI 1.3–37.5) in favor of intraoperative problems in the SB cohort (Table 3).
Data were analyzed in two different ways: (1) by initial operation only (Table 3a) and (2) including data from all operations (Table 3b). For the set of analyses including all data each observation from one patient was weighted by the reciprocal of the number of observations for that individual.
ASA = American Society of Anesthesiologists; CI = confidence interval; ICU = intensive care unit; IQR, interquartile range; PCOR = proportional cumulative odds ratio; SD = standard deviation.
Postoperative
The time spent in intensive therapy unit (ITU) was higher in the SB cohort (0.294 days/PCNL in SB cohort compared to 0 (unplanned ITU admission) and 0.097 days/PCNL (planned ITU admission) in control.
The 6 days planned ITU admissions in the control group reflected one patient with severe ischemic heart disease and bilateral symptomatic staghorn calculi who had 4 and 2 days on ITU, respectively, for cardiac monitoring following staged PCNLs on each kidney. Similarly, total length of stay was a median of 3 days longer in the SB cohort (95% CI 2–5; Fig. 2). Postoperative sepsis sufficiently severe to require parenteral antibiotics and extended hospital stay was greatly increased in the SB cohort (38% risk) compared to control (1.6%), giving a highly significant OR of 37.8 (95% CI 4.9–630) in favor of risk of sepsis in the SB cohort. Postoperative transfusion rate was also significantly higher in the SB compared to the control cohort [4 out of 34 (11.8%) PCNLs requiring transfusion in SB cohort compared to 1 out of 62 (1.6%) PCNLs in control cohort, equating to 0.24 units/PCNL in SB compared to 0.05 units/PCNL in control group]. Units/PCNL were used as a more accurate reflection of degree of hemorrhage rather than the simple binary “transfusion yes/no” that does not indicate volume of blood required.
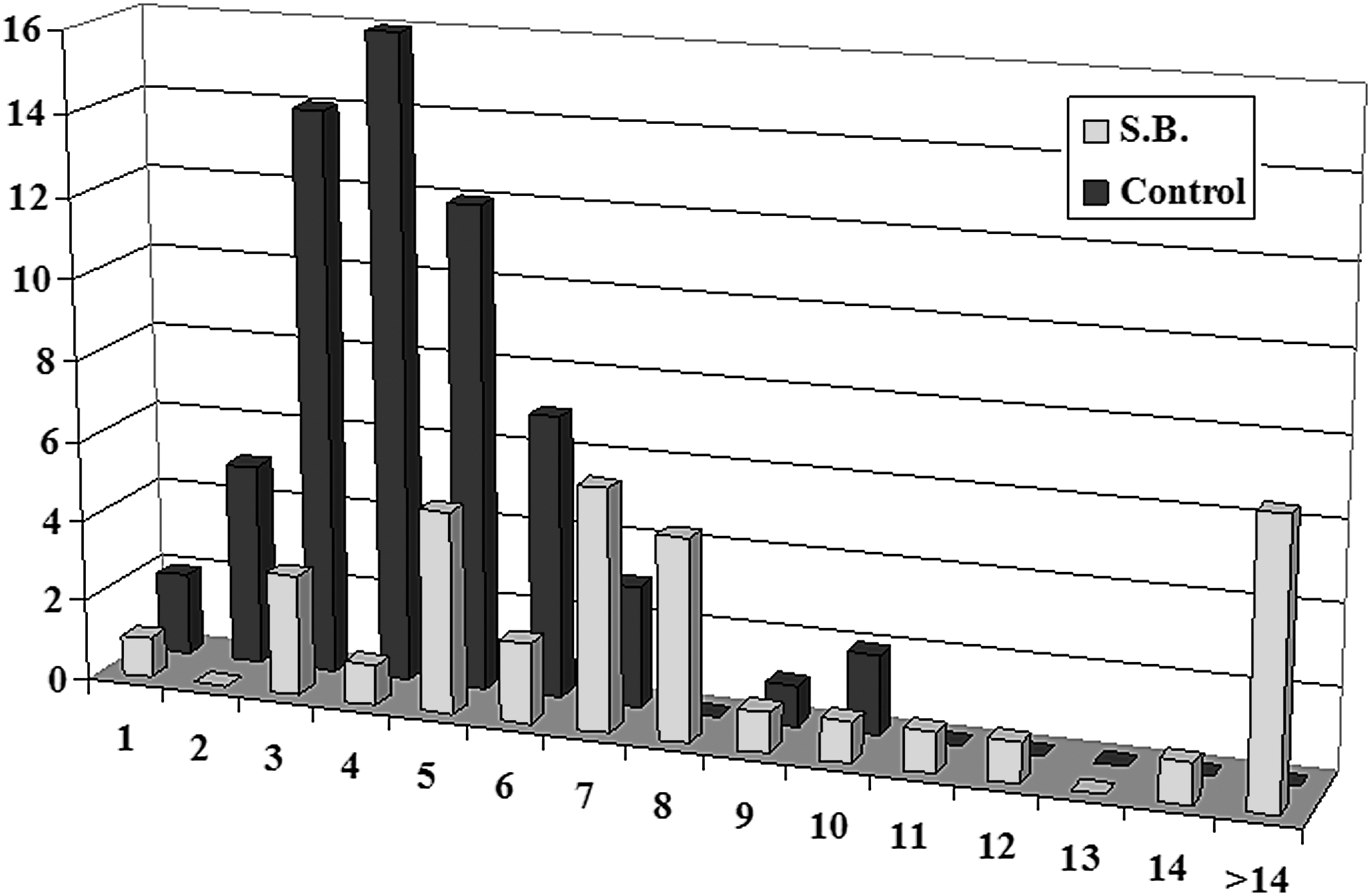
Total hospital stay for PCNLs performed in patients with SB (red) and neurologically intact controls (blue). y-Axis frequency (number) and x-axis total inpatient stay (days). Note that the only patient in the SB cohort who stayed for 1 day had the procedure abandoned because of slippage of the endotracheal tube.
Stone size and composition were not recorded in all cases, but available data showed that matrix stones and complete staghorn calculi were more common in the SB cohort (Table 3). A typical case is shown in Figures 3 to 5. The difficulties posed by the diagnosis of SB in terms of abnormal anatomy of the kidneys and large stone burden are well illustrated by this example.
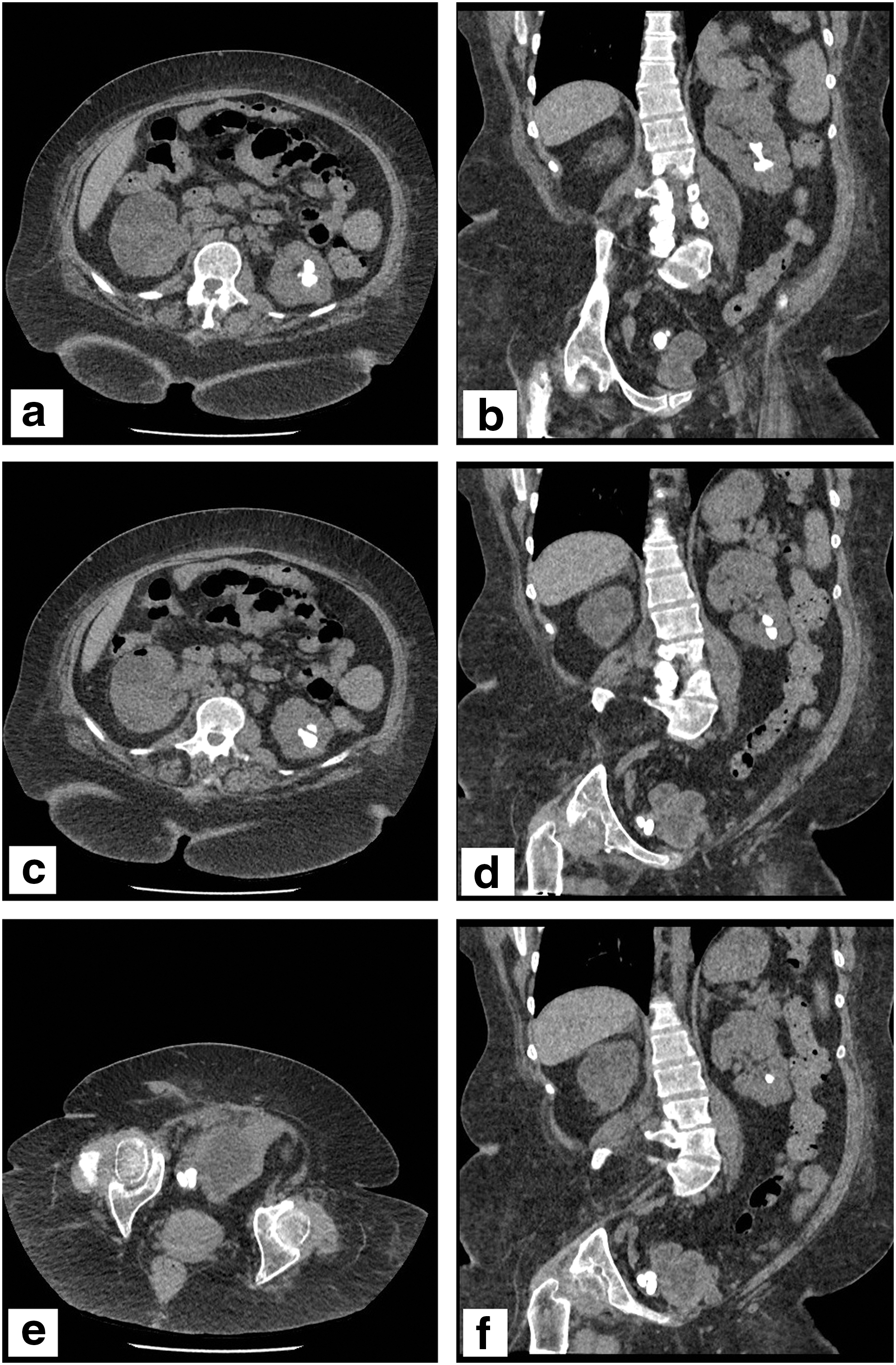
Preoperative axial and coronal CT images showing a partial left lower pole staghorn stone, with an additional lower calyceal stone in a parallel-lying calyx

Intraoperative fluoroscopic images showing radiopaque stones, for which two tracks were performed. Wire access was secured to both tracks

Postoperative axial
Perhaps of most concern is that the number of nephrectomies performed for symptomatic nonfunctional kidneys as a consequence of recurrent stone disease was 3/13 patients with SB, and 0/50 in the control group (p = 0.004, Fisher's exact test). This occurred despite long-term surveillance in the SB cohort, which clearly demonstrated a progressive loss of function in kidneys associated with recurrent stone disease and repeated surgical intervention. Kidneys removed for other reasons (n = 0 in SB cohort; n = 1 in non-SB cohort [subsequent renal carcinoma]) were excluded from analysis.
Discussion
The impact of spinal cord dysfunction on the prevalence, recurrence, and management of urinary lithiasis has been investigated in only a handful of publications, almost all of which investigated patients with a variety of underlying neurological abnormality, including SB, spinal cord injury, multiple sclerosis, and a variety of other underlying diagnoses. 8 –13 None of these compared their outcome data to non-neurologically impaired controls. Although these series report an association between neurological impairment and various surrogate markers of poor outcome, such as increased ASA score, major complication rate, and intensive care support, in the absence of matched controls, the significance of neurological disability remains undefined, since the data are not comparative to the local non-SB denominator. In all but a single report of five patients with SB, 13 the underlying neurological abnormality was heterogeneous and unlikely therefore to have a homogeneous impact on the natural history of stone disease. Additionally, surgical access for PCNL is likely to be more challenging in patients with SB compared to spinal cord injury sustained as an adult, since the latter group are more likely to have normal Cobb scoliosis angles and an anatomically normal bladder.
Similar findings were reported in a publication interrogating the National Inpatient Sample (NIS) database in which patients with SB were compared to non-SB patients. 14 The NIS provides data from a 20% stratified probability sample of American Hospitals, and first began in 1988, with eight states within the United States contributing data. This publication reported on over 4 million individual stone-related admissions, of which just over 12,000 were in patients with a diagnosis of SB (0.3%). Adjustments were made for factors such as hospital size, teaching hospital status, insurance status, year, and comorbidity. Statistically highly significant differences were seen in multiple outcomes measures such as urinary or respiratory infection, bleeding, prolonged ventilation and so on. The report does not make clear whether patients undergoing repeat stone surgery (the database was interrogated between 1998 and 2011) were counted once or multiple times, and given the pooled nature of the database, there was no analysis of outcome variance from one hospital to another. In addition, no neurological diagnosis was investigated in the control group (such as spinal cord injury, etc.). Although this is a fascinating and important “snapshot” of large-scale outcome figures of SB patients compared to non-SB, it does not answer the question of the significance of a diagnosis of SB if all other factors, such as hospital volume and surgeon/radiologist experience are (as far as possible) excluded.
We present the first report in a peer-reviewed journal to address preoperative comorbidities, intraoperative difficulties, and postoperative outcome in a cohort of SB patients compared to historical controls in a single regional specialist stone unit. Many of the procedures were performed before operative complication scoring systems such as the Clavien system 15 and because of the difficulties of defining a complication and its severity, we focused on objective outcome data. Our results clearly indicate a statistically, and clinically significant increase in preoperative comorbidity, increased intraoperative technical problems, increased operative time, postoperative complication rate, and increased risk of multiple stone procedures (Figs. 3 and 4). Most worryingly, we have also found a statistically significant risk of loss of renal units associated with multiple stone recurrence and repeated surgical intervention leading to progressive loss of renal function and “end-stage” stone disease within an essentially nonfunctional kidney.
The increased risk in SB patients (Table 4) may be summarized into different groups as follows: (1) Difficult surgical access. Most patients with SB had gross spinal deformity, creating problems positioning on the operating table and obtaining good views with the image intensifier, making percutaneous access difficult. Because this study was retrosepctive, imaging did not allow us to accurately determine the Cobb angle of scoliosis for all patients, but incomplete data demonstrated median Cobb angles above 40° and below 20° for SB and non-SB cohort respectively. Brisk bleeding interfering with vision and stone clearance was far more common in the SB cohort, which correlated to a significantly increased postoperative transfusion rate (0.24 units/PCNL in SB compared to 0.05 units/PCNL in control group). (2) Increased risk of postoperative high dependency care. The SB cohort had a significant increase in mean ASA score. In many patients, this was largely due to a restrictive pulmonary defect as a consequence of deformity of the thoracic cage. Small numbers precluded statistically meaningful comparison of formal lung function testing, but this was a major concern in nearly half of the SB patients compared to no patients in the control group (although one patient in the control group had a significant obstructive pulmonary function defect as a consequence of long-term smoking and chronic obstructive pulmonary disease). As a consequence of worse than expected poor pulmonary function testing, two patients had their procedures delayed to discuss increased risk of pulmonary complications. The risk of brisk bleeding was much higher in the SB cohort (11.8% vs 1.6% of cases), presumably secondary to difficult percutaneous access and high urinary infection rate. Postoperative sepsis occurred frequently in the SB cohort despite parenteral antibiotics administered regularly starting on anesthetic induction and continuing postoperatively (38% in SB cohort compared to 1.6% in control). The risk of admission to ITU for unanticipated complications was much higher in the SB cohort (0.294 days/PCNL in SB cohort compared to 0 (ICU admission for unanticipated complications) and 0.097 days/PCNL (planned ICU admission for monitoring in patient with severe established respiratory disease) in control. (3) Postoperative complications. Nearly all patients in the SB cohort were nonambulant, so postoperative mobilization was a problem, and over 20% had pre-existent pressure sores. Overall hospital stay was significantly increased in the SB cohort (7 days vs 4 days). Risk of blood transfusion, sepsis, and unplanned admission to ICU were all significantly raised in the SB cohort. One explanation for sepsis is the increased prevalence of matrix stone (Table 3). Stone analysis was not available for all patients, but statistical analysis of available results suggests that postoperative risk of sepsis was much higher in the SB cohort even correcting for stone type.
This study is limited by a number of potential shortcomings. It is a nonrandomized retrospective case–control series, and not all data points were available for all patients. There is the potential for selection bias if fitter SB patients were treated in local hospitals, but local referring units have historically not performed any PCNL work at all until recently, and some continue to refer all PCNLs to the regional stone unit. In addition, the complexity of such patients is such that it seems very likely that all SB patients with urinary tract stones would all have been referred, and this study should therefore have reliably captured data for all patients with SB and stone disease within this region. SB were more likely to be obese, and because this was a retrospective audit, we were not able to match patients for obesity. Because of the relative scarcity of SB patients even in this tertiary referral center, available imaging was not sufficiently complete to allow meaningful measurement of skin-stone distance.
Nonetheless, the patient cohort reflect “real” clinical practice, and although SB are therefore more likely to be obese, this reflects one technical challenge of PCNL in this patient group. Due to the length of follow-up, operations were not all performed by the same surgeon or radiologist, but all were performed by consultants with special interest in stone disease and extensive experience of PCNL. Overall therefore, although surgeon's experience may be another potential source of bias, it seems very unlikely to be the underlying cause of such markedly differing outcome data. In terms of postoperative sepsis, antibiotic regimens were not identical across all patients, reflecting surgeon choice and preoperative urine culture results, but the difference is so marked that variation in antibiotic usage is unlikely to be a significant confounding factor. In addition, expert microbiological advice was sought in these cases, and the choice of antibiotic was therefore most appropriate to the patient's culture results. The assessment of stone-free rate after intervention remains a contentious issue within the endourology community. These data are a reflection of day-to-day clinical practice over a number of years, and therefore there is heterogeneity of imaging modalities. Although this may have an impact on stone-free rates, the choice of imaging reflects what was freely available at the time, and since controls are historically matched, this is unlikely to vary between control and SB groups.
There is on-going debate as to whether surgery for complex problems or in patients at high risk should be referred to regional specialist centers. The concentration of major urological surgery, such as pelvic oncology, in high volume specialist centers is already established in many European countries. With respect to pelvic oncological surgery, the response of the U.K. Government was to reorganize treatment of cancer services according to a “hub and spoke” principle that has been adopted as the standard of care over the past two decades. There is a general trend for complex benign surgery to gravitate toward specialized regional centers of expertise, and anecdotal reports suggests that it also happens for complex benign urological conditions such as urethral reconstruction, surgical management of erectile dysfunction and so on. This trend is a source of active debate with respect to PCNL within the United Kingdom. In contrast to European data published by the Clinical Research Office of the Endourological Society, 16 there were no significant differences in outcome when high and low volume centers were compared in the United Kingdom. 17 However, recent figures and subgroup analysis presented at the BAUS Annual conference in June 2016 18 suggest that a trend is emerging toward improved outcome and reduced length of stay in high volume centers within the United Kingdom, and it will be interesting to observe whether these trends become more pronounced and statistically significant as the database matures. Patients with SB and stone disease remain a relatively rare patient group, and we suggest that the value in offering such patients surgery in high volume centers is that they are under the care of specialist endo-urologists and uro-radiologists who have had substantial exposure to PCNL in this patient cohort, and experience managing the frequent complications.
Conclusions
In summary, this report demonstrates that the diagnosis of SB confers adverse risk on multiple intra- and postoperative outcome measures of PCNL such as increased hospital stay, increased risk of admission to ITU, increased risk of recurrent disease, blood transfusion, repeated surgical interventions, and stone disease-related nephrectomy. Although this is a non-randomized retrospective analysis, there are no other published outcome data in patients with SB undergoing PCNL with neurologically intact historically matched controls. As far as possible, we have sought to reduce potential bias within our data, and although retrospective, our recommendations based on our own experience are as follows: (1) Patients with SB should have formal pulmonary function testing before PCNL and senior anesthetic review at the time of preassessment. (2) Patients with SB should have preoperative antibiotic treatment. Our protocol is a minimum of 24 hours parenteral antibiotics before PCNL, but other options such as an extended course of oral antibiotics before surgery are just as valid. (3) Patients with SB should ideally be operated on in high volume specialist stone units with planned postoperative admission to a surgical high-dependency or ITU. (4) Patients with SB should be counseled about substantially increased risk of complications, the long-term risk of recurrent stones, and consequent increased risk of nephrectomy for “end-stage” stone disease.
Footnotes
Author Disclosure Statement
Stephen Mitchell is a consultant to Cambridge Nutraceuticals. Daron Smith is a consultant for Boston Scientific and Porges Coloplast; lecture for Cook Medical; and education for Olympus KeyMed. No competing financial interests exist for the remaining authors.