
Abstract
Objectives:
Mayo adhesive probability (MAP) score quantifies adherent perinephric fat (APF) and is associated with the prolongation of surgery duration or the increase of surgical complication rates.
Patients and Methods:
In this study, 311 patients who underwent robot-assisted partial nephrectomy (RAPN) at our institute were included. APF was quantified using the MAP score calculated using perinephric fat thickness and stranding seen on a preoperative enhanced CT scans. The surgery duration was classified into the dissection (robotic manipulation to hilar clamping) and resection (hilar clamping to robotic surgery completion) phases.
Results:
The MAP score was found to be 0, 1, 2, 3, 4, and 5 in 98 (32%), 86 (28%), 21 (7%), 48 (15%), 44 (14%), and 14 (4%) patients, respectively. The dissection and resection phase times increased with an increase in the MAP score. The median dissection phase times for MAP scores of 0, 1, 2, 3, 4, and 5 were 71.7, 79.1, 88.9, 97.0, 99.7, and 118.8 minutes, respectively. The MAP score was more strongly associated with the prolongation of the dissection phase than with the prolongation of the resection phase. In multivariate analysis for dissection phase time of more than 90 minutes, the body mass index [odds ratio (OR) = 1.09, p = 0.0209], early surgical experience (first 100 cases) (OR = 2.32, p = 0.0024), and MAP score ≥3 (OR = 6.20, p < 0.0001) significantly associated with the prolongation of dissection phase in a logistic regression model.
Conclusions:
The MAP score is a factor significantly associated with the prolongation of the dissection phase during RAPN.
Introduction
T
The Mayo adhesive probability (MAP) score 5 is used to quantify APF and is reportedly valuable for predicting APF in patients undergoing robot-assisted partial nephrectomy (RAPN). However, how the RAPN duration is affected as the MAP score increases remains unclear. Thus, this study analyzed the relationship between the MAP score and the factors associated with RAPN procedures using cases from our facility. In addition, a recent study has reported the relationship between perinephric fat and histology of RCC. 6 We also examined the association of cancer biology with the MAP score.
Patients and Methods
We retrospectively analyzed the clinical cases of 311 patients with renal tumors who underwent RAPN using the da Vinci S Surgical System (Intuitive Surgical, Sunnyvale, CA) at our institute. Three surgeons performed equivalent number of RAPNs, and all were experienced in laparoscopic surgery. The surgical procedures were previously described. 5,7,8 Before surgery, all patients underwent enhanced CT or MRI for defining the clinical stage and anatomic properties of the tumors. Using these images, two urologists (R.I. and T.K.) independently calculated the MAP score before surgery. R.I. was an independent observer, and T.K. was one of the surgeons. If the score differed between the two observers, a consensus was reached together after discussion.
The surgery duration was classified into two phases, the dissection (robotic-manipulation commencement to hilar clamping) and resection (hilar clamping to robotic-manipulation completion) phases.
Robot-assisted partial nephrectomy
A standard surgical procedure was followed for RAPN, 5,7,8 with three robotic arms and a camera port. For assistance, two 12 mm ports were placed; a 5 mm port was placed at the midline below the xiphoid for liver elevation in right renal tumor cases by the transperitoneal approach. The renal hilum was entirely dissected using bulldog clamps on the main trunk of the renal arteries during tumor resection. The renal vein was not clamped. Gerota's fat was isolated from the kidney, and the tumor was identified using intraoperative ultrasound. The tumor was entirely excised with surrounding normal tissue margins using warm ischemia, the inner layer of the collecting system was sutured, and renorrhaphy was performed with early unclamping after suturing.
MAP score assessment
We calculated the MAP score as previously described, evaluating the thickness and stranding of perinephric fat at the renal vein level using enhanced CT or MRI. 5 The length between the renal capsule and the abdominal wall was measured (<10 mm = 0 points, 11–19 mm = 1 point, and >20 mm = 2 points), and the stranding was scored (no stranding = 0 points, mild stranding = 2 points, and severe stranding = 3 points). The scores were summed up to calculate the MAP score (range, 0–5).
Statistical analysis
Continuous variables were analyzed by the Mann–Whitney U-test, and categorical variables were analyzed by Chi-squared test. Univariate and multivariate analyses were performed using a logistic regression model. All statistical analyses were performed using JMP 12.1.0 software (SAS Institute, Cary, NC). A p-value <0.05 was regarded statistically significant.
Results
Patient and case characteristics
The characteristics of 311 cases included in the cohort are summarized in Table 1. The median age was 60.0 years [interquartile range (IQR): 48.0–67.0]; the median body mass index (BMI) was 23.5 kg/m2 (21.5–26.0); 255 cases (82%) were in clinical stage T1a and 56 cases (18%) were in T1b; the median tumor size was 28.0 mm (IQR: 20.0–35.0); tumor location was anterior kidney in 31%, posterior kidney in 30%, and other in 39% of cases; and transperitoneal and retroperitoneal approaches were followed in 94% and 6% cases, respectively. The Nephrometry Score showed low-, intermediate-, and high-complexity tumors in 38%, 49%, and 13% cases, respectively. The MAP scores were 0, 1, 2, 3, 4, and 5 in 98 (32%), 86 (28%), 21 (7%), 48 (15%), 44 (14%), and 14 (4%) patients, respectively. Patients with a higher MAP score (≥3) consisted of significantly more males (p < 0.0001), older individuals (p < 0.0001), and individuals with high BMI (p < 0.0001) and high American Society of Anesthesiologists score (p = 0.0013) compared with those with a lower MAP score (≤2).
Bold values indicate statistical significance p < 0.05.
ASA = American Society of Anesthesiologists; BMI = body mass index; MAP = Mayo adhesive probability; IQR = interquartile range.
Surgical results
Table 2 summarizes the surgical results in the cohort. The median surgery duration was 174 minutes (IQR: 152–204 minutes), the median console surgery duration was 129 minutes (IQR: 106–152 minutes), the median time required for the dissection phase was 81.0 minutes (IQR: 65.0–101 minutes), and the median time for the resection phase was 44.0 minutes (IQR: 37.0–55.0 minutes). The median ischemia time was 18.0 minutes (IQR: 14.0–22.0 minutes). The median estimated blood loss was 30.0 mL (IQR: 10.0–71.2 mL), 30 cases (9.6%) had postoperative complications of Clavien grade ≥3a, and the median days of postoperative hospital stay were 4 days (IQR: 4–5). Patients with a higher MAP score (≥3) showed significantly longer surgery durations (p < 0.0001), console surgery durations (p < 0.0001), dissection phases (p < 0.0001), resection phases (p < 0.0001), and ischemia times (p = 0.0333), compared with those with lower MAP scores (≤2). No statistical significance was found in estimated blood loss (p = 0.3536), postoperative complications of Clavien grade ≥3a (p = 0.9273), or the days of postoperative hospital stay (p = 0.3279). No case was converted to open surgery. A positive surgical margin was found in two patients with a higher MAP score, but this was not statistically significant. Two patients with a lower MAP score developed recurrence at distant organs, but this too was not statistically significant.
Bold values indicate statistical significance p < 0.05.
Association between the MAP score and cancer biology
Table 3 summarizes the pathologic outcomes. Here, 251 cases (88%) were in pathologic stage T1a; 28 (10%), T1b; 1 (<1%), T2a; and 3 (1%) T3a. Furthermore, 218 cases (70%) were diagnosed with clear cell carcinoma; of these, 25 cases (8%) were papillary cell carcinoma, 28 cases (9%) were chromophobe carcinoma, 13 (4%) were another malignancy, and 27 (9%) were benign tumors. Moreover, 38 cases (14%) were classified as Fuhrman grade 1, 181 cases (64%) as grade 2, 60 cases (21%) as grade 3, 4 cases (1%) as grade 4; and 44 cases showed the presence of lymphovascular invasion. There was no significance in pathologic parameters between patients with a MAP score of ≤2 and those with a MAP score of ≥3, including pathologic T stage (p = 0.4109), histologic subtype (p = 0.1847), Fuhrman grade (p = 0.3647), and lymphovascular invasion (p = 0.9202).
Prolongation of the dissection and resection phases according to the MAP score
Figure 1 compares the median dissection and resection phase times during RAPN according to the MAP score. The dissection and resection phase time prolonged as the MAP score increased. The median dissection phase times were 72.0, 77.5, 92.0, 94.0, 99.0, and 115.0 minutes for the MAP scores of 0, 1, 2, 3, 4, and 5, respectively. The MAP score was more closely related with the prolongation of the dissection phase than with that of the resection phase.
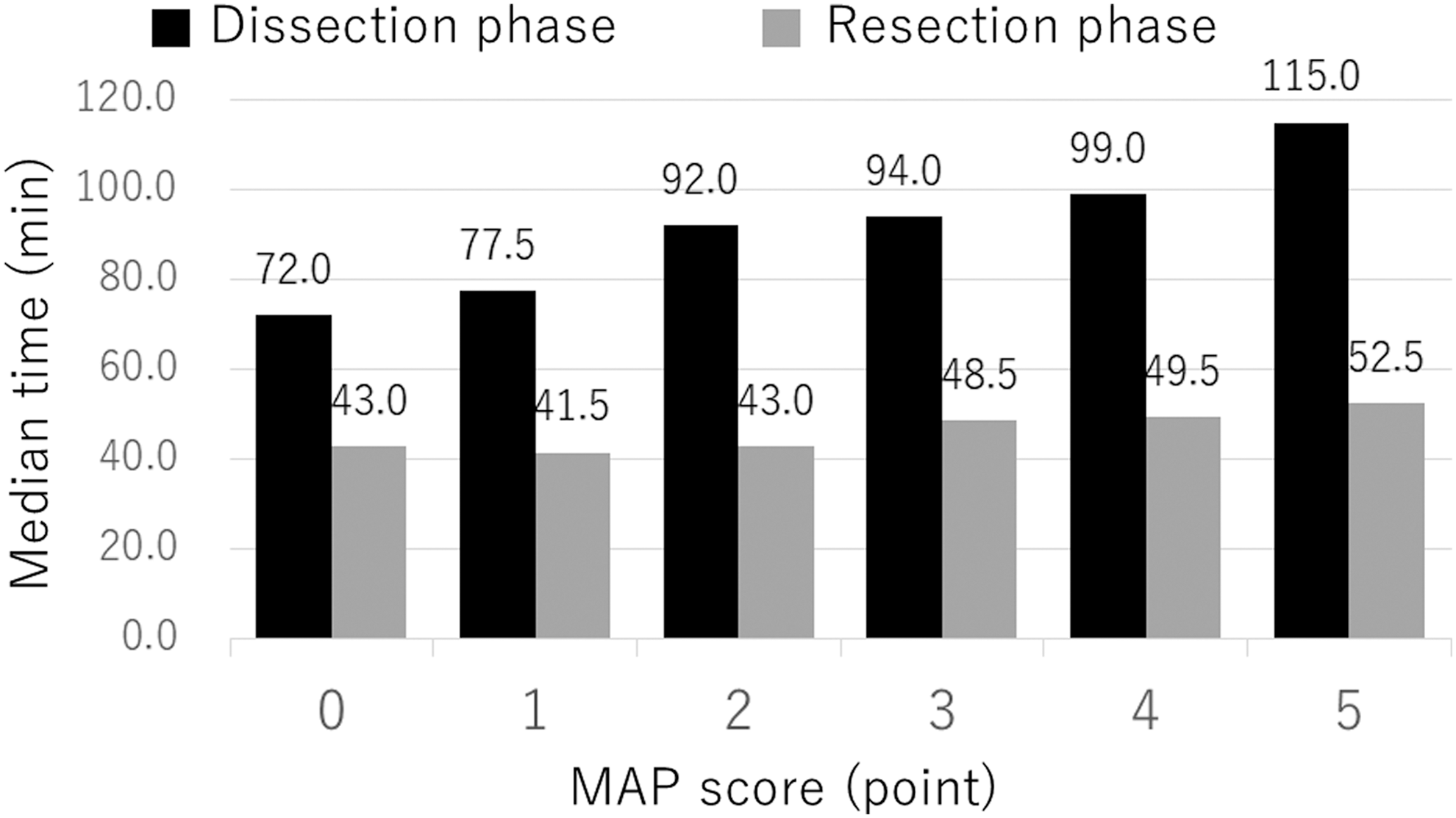
The duration of dissection and resection phases during robot-assisted partial nephrectomy according to MAP score. Comparisons of the median duration between dissection and resection phase according to MAP score (range, 0–5). Black bar indicates the median duration of the dissection phase; Gray bar indicates the median duration of the resection phase. MAP = Mayo adhesive probability.
Factors associated with the prolongation of the dissection phase by univariate and multivariate analyses
Table 4 shows the univariate and multivariate analyses in association with a dissection phase of over 90 minutes, using the logistic regression model. As the multivariate analysis indicates, BMI [odds ratio (OR) = 1.09, p = 0.0209], MAP score ≥3 (OR = 6.20, p < 0.0001), and 1st to 100th cases (OR = 2.32, p = 0.0024) were significant factors for the prolongation of the dissection phase.
Bold values indicate statistical significance p < 0.05.
CI = confidence interval; OR = odds ratio.
Discussion
Urologic surgeons can experience difficulty with both open and laparoscopic procedures when significant abdominal fat is present. BMI has been used to evaluate vesical fat before surgery. However, BMI has been reported to have no association with complications in PN with almost lowest invasion. 4,9 –12 Gorin et al. 4 reported that patients with high intra-abdominal fat (IAF) have a risk of experiencing surgical complications such as bleeding, pseudoaneurysm formation, and urine leak in PN, and that visceral adiposity affects surgery duration in laparoscopic nephrectomy and is a risk for Clavien grade III and IV complications in RAPN procedures. Morris et al. 13 reported that, in abdominal surgery, IAF was a better predictive factor for postoperative complications and mortality than BMI. However, a more integrated scoring system appears to be necessary for a comprehensive evaluation of APF, and a qualitative evaluation of IAF before surgery will help predict perioperative complications.
Davidiuk et al. 7 developed MAP score for the qualitative evaluation of APF. The MAP score evaluates fat quality based on the thickness and stranding of perinephric fat in PN. The MAP score showed a more significant association with APF in PN than BMI or fat thickness alone. 7 Dariane et al. 14 evaluated APF and analyzed the factors associated with APF. Their results also showed that the MAP score was a significant predictive factor for APF. APF is easier to evaluate with the MAP score than with other indicators because the calculation of MAP score only requires thickness measurement and evaluation of perinephric fat stranding, without cumbersome imaging. To the best of our knowledge, the MAP score is the only available means for the comprehensive quantification of APF, 15,16 and can be easily used in clinical practice and patient counseling.
Our study shows that the duration of surgery, console surgery, dissection phase, resection phase, and ischemia were significantly associated with a MAP score of ≥3, and in particular, the dissection phase duration was more prolonged than the resection phase duration as the MAP score increased. In addition, a MAP score of ≥3 was also significantly associated with a prolonged dissection phase in multivariate analysis (OR = 6.20, p < 0.0001). Our study suggests that APF presence is mainly associated with the prolongation of the dissection phase, in which the APF is peeled from the renal capsule and other tissues, compared with the prolongation of the resection phase, in which the tumor is excised from the renal parenchyma. Therefore, we hypothesize that APF evaluated by the MAP score is a predictive factor for complexity of perinephric fat dissection in RAPN procedures.
Dariane et al. 14 reported an association between surgical outcomes and APF evaluated by intraoperative findings during PN. Their results showed that the total surgery duration in the surgical cases with APF was significantly longer than that in cases with no APF, which is similar to the results from our study. However, our study differed from theirs in two points. First, in our study, the APF was evaluated using the MAP score before RAPN. In clinical practice, it appears that it is important to evaluate APF and predict surgical complexity using preoperative imaging before surgery. Second, our study analyzed the MAP score with the time required for each of the two phases, by dividing the surgery duration into dissection and resection phases. This enabled us to show the adverse influence of APF evaluated by the MAP score especially on procedures in the dissection phase, including the dissection of renal vessels and identification of the tumor and renal capsule surrounding the tumors. Thus, our study suggests that there is a relationship between APF evaluated by the MAP score before RAPN and the complexity of manipulations in RAPN procedures.
Recently, a potential association between perinephric fat and the histology of RCC has been inferred. Thiel et al. 6 reported that a high MAP score is related with decreased progression-free survival in patients who undergo surgical treatment for clinically localized RCC in comparison with a low MAP score, suggesting that perinephric visceral adiposity or inflammation is associated with RCC oncology. No significant difference was shown in this study between the MAP score and the pathologic outcomes, including pathologic T stage, histologic subtype, Fuhrman grade, and lymphovascular invasion. However, this may be because of some limitations in our study, including the small cohort or its retrospective nature; thus, further studies would be required to reach a definitive conclusion.
In addition to the abovementioned limitations, the techniques used by the three surgeons were not completely consistent. In this study, we excluded procedures performed by inexperienced surgeons. Thus, all cases analyzed herein were performed only by experienced laparoscopists. Finally, the BMI range in our population was different from that of other populations from the United States and Europe. In our study, the median BMI was 23.5, which was lower than 28.9 reported by Davidiuk et al. 5 Thus, our results may not be applied to other populations.
Conclusions
The MAP score is a significant factor associated with the prolongation of the dissection phase in RAPN procedures. Use of this factor makes it possible to assess the risk of prolonged surgery duration before RAPN. Our study mainly described the association between the MAP score and surgery duration. Further studies will be required to determine whether the MAP score representing APF affects perioperative complications and postoperative kidney function.
Footnotes
Acknowledgment
The authors thank Ms. Nobuko Hata (Tokyo Women's Medical University) for secretarial work.
Author Disclosure Statement
No competing financial interests exist.